

International Journal of
Environmental Research
and Public Health
Article
Short-Term Effects of Forest Therapy on Mood States:
A Pilot Study
Francesco Meneguzzo 1,2,* , Lorenzo Albanese 1, Michele Antonelli 3 , Rita Baraldi 4,
Francesco Riccardo Becheri 5, Francesco Centritto 6, Davide Donelli 3, Franco Finelli 2, Fabio Firenzuoli 7 ,
Giovanni Margheritini 2, Valentina Maggini 7 , Sara Nardini 8 , Marta Regina 9, Federica Zabini 1,*
and Luisa Neri 4
Citation: Meneguzzo, F.; Albanese, L.;
Antonelli, M.; Baraldi, R.; Becheri, F.R.;
Centritto, F.; Donelli, D.; Finelli, F.;
Firenzuoli, F.; Margheritini, G.; et al.
Short-Term Effects of Forest Therapy
on Mood States: A Pilot Study. Int. J.
Environ. Res. Public Health 2021, 18,
9509. https://doi.org/10.3390/
ijerph18189509
Academic Editor: Pier Mannuccio
Mannucci
Received: 24 August 2021
Accepted: 7 September 2021
Published: 9 September 2021
Corrected: 4 March 2022
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
1 Institute of Bioeconomy, National Research Council, 10 Via Madonna del Piano, I-50019 Sesto Fiorentino, Italy;
lorenzo.albanese@cnr.it
2 Italian Alpine Club, 19 Via E. Petrella, I-20124 Milano, Italy; franco.finelli55@libero.it (F.F.);
giomarghe@yahoo.com (G.M.)
3 Local Public Health Authority, AUSL- IRCCS, I-42122 Reggio Emilia, Italy; michele.antonelli@ausl.re.it (M.A.);
davide.donelli@ausl.re.it (D.D.)
4 Institute of Bioeconomy, National Research Council, 101 Via Gobetti, I-40129 Bologna, Italy;
rita.baraldi@cnr.it (R.B.); luisa.neri@ibe.cnr.it (L.N.)
5 Pian dei Termini Forest Therapy Station, 2311 Via Pratorsi, I-51028 San Marcello Piteglio, Italy;
ricerca@terapiaforestale.it
6 “Cesare Alfieri” Political Science School, University of Florence, 60 Via Vittorio Locchi, I-50141 Firenze, Italy;
francescocentritto08@gmail.com
7 CERFIT, Careggi University Hospital, I-50134 Florence, Italy; fabio.firenzuoli@unifi.it (F.F.);
valentina.maggini@unifi.it (V.M.)
8 A.M.I.S.I. Italian Medical Association for the Study of Hypnosis, 28 Via Paisiello, I-20131 Milano, Italy;
nardini_s@libero.it
9 Mindfulness Association UK, Edinburgh EH9 1AR, UK; marta@martaregina.com
* Correspondence: francesco.meneguzzo@cnr.it (F.M.); federica.zabini@cnr.it (F.Z.);
Tel.: +39-392-985-0002 (F.M.); +39-333-379-2947 (F.Z.)
Abstract: Immersion in forest environments was shown to produce beneficial effects to human
health, in particular psychophysical relaxation, leading to its growing recognition as a form of
integrative medicine. However, limited evidence exists about the statistical significance of the effects
and their association with external and environmental variables and personal characteristics. This
experimental study aimed to substantiate the very concept of forest therapy by means of the analysis
of the significance of its effects on the mood states of anxiety, depression, anger and confusion.
Seven forest therapy sessions were performed in remote areas and a control one in an urban park,
with participants allowed to attend only one session, resulting in 162 psychological self-assessment
questionnaires administered before and after each session. Meteorological comfort, the concentration
of volatile organic compounds in the forest atmosphere and environmental coherence were identified
as likely important external and environmental variables. Under certain conditions, forest therapy
sessions performed in remote sites were shown to outperform the control session, at least for anxiety,
anger and confusion. A quantitative analysis of the association of the outcomes with personal
sociodemographic characteristics revealed that only sporting habits and age were significantly
associated with the outcomes for certain psychological domains.
Copyright: © 2021 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
Keywords: anger; anxiety; confusion; depression; forest therapy; mental health; volatile organic
compounds
1. Introduction
The direct exposure to forest environments was attributed a wide range of straight
benefits to human health. Such benefits cover primarily the psychological sphere (mental
processes, stress, anxiety and emotions), cognitive processes, social life (skills, interactions,
Int. J. Environ. Res. Public Health 2021, 18, 9509. https://doi.org/10.3390/ijerph18189509
https://www.mdpi.com/journal/ijerph

Int. J. Environ. Res. Public Health 2021, 18, 9509
2 of 21
behavior and lifestyle) and spiritual wellbeing [1–4]. On the physiological side, significant
effects emerged with regards to the improvement of the cardiovascular functions and the
hemodynamic, neuroendocrine, metabolic, immune, inflammatory and oxidative indices [5,6].
As pointed out by a recent comprehensive review, the impact on the psychophysical
well-being of humans by immersion in forest environments was by far the most studied and
revealed statistically significant and sometimes intense results [7]. However, in the same
review, the results of experiences with patients affected by various diseases and addictions
were reported, such as improving sleep quality in patients with gastrointestinal cancers [8].
In addition, in-patients with affective and psychotic disorders received significant benefits
to their mental health from forest therapy programs, with the type and extent of the
improvements related to the characteristics of the given disorder [9].
Individual benefits can turn into benefits for the society as a whole due to cost savings
for healthcare systems, insurance and safety, as well as gains in productivity. A recent study
showed that the economic value of natural protected areas, assessed on the basis of the
mental health of visitors, amounts to about 8% of the global gross domestic product, i.e.,
around USD 6 trillion [10]. Such an amount, being 100 to 1000 times greater than the budget
of the agencies managing the natural protected areas, could justify any scientifically based
effort aimed at increasing the efficiency and expanding the functions and ecosystem services
of the natural and protected areas towards human mental and physiological health [10].
The preventive and healing effects directly delivered by forest environments have
been widely documented in the scientific literature, and, in most cases, concern experiences
of free walking or meditation in the absence of appreciable physical exercise [11]. The
beneficial effects towards the psychological and physiological aspects of human health
are often significant, dose-dependent (e.g., duration and frequency of the experiences and
concentration of airborne bioactive substances), related to the structure and tree species
composition of the forest and to the season and time of the day [11]. Personal characteristics
such as gender, age, psychological traits and physical health contribute to modulating the
extent of beneficial effects of the forest immersion. In particular, a recent study performed
in Hungary showed that walking in the forest for 2 h, with minimal guidance and aimed at
maintaining a slow pace, resting, observation, breathing and touching the wood produced
a significant decrease of systolic blood pressure both in late spring and winter [12]. As well,
a significant stimulation of NKbright cells and activation of various immune cell subsets was
observed in late spring, while a slight activating and a balancing effect regarding TIM-3,
an inhibitory immune checkpoint molecule, were observed in winter, thus suggesting
positive forest healing effects throughout the year [12].
The forest healing effects can be wide-spectrum, such as in the case of the immune
system [13], long-lasting and devoid of undesirable side effects. Just 15–20 min of forest
immersion are enough to convey, at least, significant psychological benefits, two hours
(even not continuously) allow enhanced wellbeing for a week, irrespective of individual
characteristics such as age and presence of chronic diseases [14]. Three or more days of
forest immersion can reinforce the immune defense system for a month [15].
An additive effect (constantly growing benefits) deriving from the regular repetition
of sessions was observed, which was larger in the case of subjects with depressive tenden-
cies [16]. A recent study, consisting of free forest immersion sessions (four weekly sessions
each lasting four hours), suggests the persistence of psychological benefits (indicators of
stress, wellbeing and positive emotions) up to a month after the end of the sessions, con-
trary to virtual immersion experiences [17]. Indeed, virtual experiences showed significant
psychological effects but only in the short term [18].
Forest experiences, where professionals assist participants according to structured pro-
tocols, often based on psychotherapy, meditation and mindfulness practices [19], showed
significant and remarkable therapeutic superiority over both similar activities carried out
in non-forested environments and free immersion in forest, for example, in the treatment
of depressive symptoms [11,20]. The actual forest therapy foresees not only the individual
free immersion in a forest environment, often called forest bathing, but also the guidance by

Int. J. Environ. Res. Public Health 2021, 18, 9509
3 of 21
suitable professionals, such as psychologists and psychotherapists, according to protocols
aimed at boosting the health outcomes [11,20]. Indeed, the very possibility of issuing
green prescriptions in the frame of medical phytotherapy protocols was conditioned on the
availability of forest therapy providers [21].
The benefits of forest immersion are mediated by all human senses. Viewing repetitive
natural structures (fractals), such as trees, and hearing the typical sounds of forests convey the
perception of a relaxing and unchallenging environment, in which it is much easier to adapt
and increase one’s own perceptive fluidity [22,23], even in virtual experiences [18]. Touching
the wood of the trees induces significant physiological and psychological relaxation [24].
Smell plays a key role through the inhalation of biogenic volatile organic compounds
(BVOC) emitted by plants and soil in the forest atmosphere, in particular, certain terpenes
endowed with antioxidant and anti-inflammatory activities, as well as beneficial to psycholog-
ical and cognitive processes [25]. First of all, the concentration and type of such substances in
the forest atmosphere depends on the emission rate by plants and thus on the tree species [26]
and their vegetative status (thus, the season) [27]. At any forest site and in any season (es-
pecially during the warm season), the time of the day plays a very important role due to
changing atmospheric conditions (temperature, solar irradiance and surface stability), leading
to distinct and regular peaks and troughs in the total BVOC concentration levels [28,29].
The benefits and potential of forest therapy were officially recognized by the United
Nations in the framework of the green recovery from the COVID-19 pandemic [30]. The
main challenges were identified in informing, educating and persuading healthcare systems
and professionals and citizens with regard to green prescriptions, for example, based on
those that have been issued for years in Japan and South Korea [5,31,32]. In those countries,
as well as in Taiwan and China, green prescriptions have been framed into preventive
medicine, as a means to improve physiological health and ease stress levels [33]. Another
urgent challenge was identified in the certification of professional providers of services
related to forest therapy meant to effectively enable green prescriptions and allow interested
people to access a widespread and high quality offer [21,34].
Despite the growing scientific evidence, many countries, especially in the Western
world, lag behind in the rigorous identification of sites and trails for forest therapy practices,
including preliminary selection and qualification based on actual functionality (observed
psychological and physiological benefits) according to structured programs of activities.
First, the following consolidated evidence was seldom incorporated: while exposure to
most greenspaces allows for improvements in mood and wellbeing, specific and significant
preventive effects with regard to the risk of depression were attributed only to natural
environments, in particular forested ones, remote from urban areas [35,36]. This is par-
ticularly important because depression is a pandemic illness, especially in the developed
world [35], with immense human, social and economic costs [36]. Thus, natural remedies
such as forest therapy performed in suitable locations can lead to substantial savings for
healthcare and welfare systems and gains in terms of productivity [34].
Second, especially in the Western world, forest therapy experiences in remote forest
areas involving large numbers of participants, according to structured and repeatable
programs and including control sessions in urban settings, were seldom performed, let alone
the search for the main determinants of health outcomes that would allow the generalization
of qualification criteria. Despite recent improvements in the methodological rigor, the
recommendations issued in a comprehensive review published in 2017 are still relevant [37].
The main motivation of this study was to quantitatively assess the effectiveness of
a few forest therapy sessions performed in remote areas on the improvement of certain
mood states, i.e., anxiety, depression, anger and confusion, compared with a control session,
thus substantiating the very concept of forest therapy. Another aim was to contribute to the
preliminary identification of the main determinants of the outcomes of forest therapy ses-
sions, taking advantage of the different environments involved, the relatively large number
of participants and the representativeness in terms of sociodemographic characteristics.

Int. J. Environ. Res. Public Health 2021, 18, 9509
4 of 21
The main hypotheses of this study were: (1) forest therapy carried out in remote forest
areas is more effective than in urban parks; (2) forest therapy (professionally guided) is more
effective than forest bathing (free); (3) different environmental conditions, either structural
or variable, and personal characteristics, affect the outcome of forest therapy sessions.
2. Materials and Methods
2.1. Forest Therapy Sessions: Basic Features and Measures
The Italian Alpine Club and the Institute of Bioeconomy of the National Research
Council arranged seven forest therapy sessions from August to October 2020. All sessions,
named FTS1 to FTS7, were performed in Italy at remote forest areas (at least 20 km from
the nearest town with more than 10,000 inhabitants or trafficked road). All sessions had
a duration of 3.5 ± 0.5 h, along paths with total lengths not exceeding 4 km and uphill
gradients smaller than 150 m.
A further control session, named FTSC, was performed in June 2021, in an urban park
with an area of about 4 hectares, located downtown in the city of Florence, Italy (about
400,000 inhabitants) and surrounded by buildings and trafficked roads.
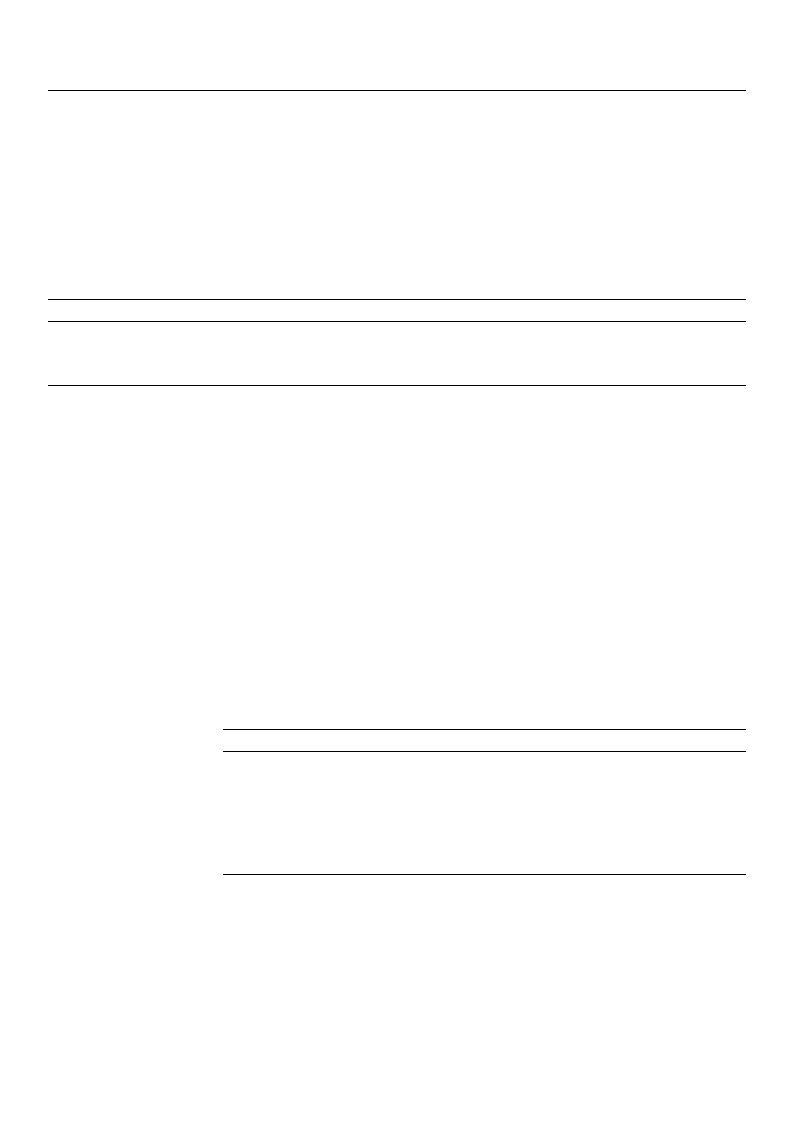
Figure 1 shows the location of the forest therapy sites in central and northern Italy.
Figure 1. Locations of forest therapy sessions (FTS1 to FTS7 and FTSC) in central and northern Italy.
During each session, the concentration of total volatile organic compounds (TVOCs)
was continuously collected by means of a portable (0.72 kg) photoionization detector (PID,
model Tiger VOC detector, Ion Science Ltd., Fowlmere, Royston, UK), with detection limits
from 1 µg/m3 to 20,000 µg/m3. The PID was equipped with a pump, sucking in ambient air
at a rate of 220 mL/min, and an ultraviolet, 10.6 eV lamp, allowing the ionization of organic
substances present in the sampled air, including all the monoterpenes (MTs) found in
biogenic VOCs (BVOCs). The resulting electric current flowing between two electrodes was
measured, amplified and transformed into a concentration level of the ionized substance
or group of substances. TVOC concentration could be considered representative for BVOC
concentration, although clearly higher due to the presence of VOCs other than MTs, at
least at forest sites far from anthropogenic pollution sources where the change in TVOC
concentration is mainly driven by plants’ emissions, as explained in a previous study [28].
Finally, the average temperature during each session was assessed based on data collected
at nearby weather stations.
The first session (FTS1), which can be classifiable as forest bathing, was performed
without professional guidance, suggesting to participants to relax in the woods during
two stops lasting between 20 and 30 min each, and providing scientific information about
the surrounding environment (botany and geology) and the sessions meaning for one’s
Int. J. Environ. Res. Public Health 2021, 18, 9509
5 of 21
own health. All the other sessions were performed with professional guidance, according
to the method of conducting illustrated in Section 2.2. However, the control session FTSC,
which was performed in an urban park downtown the city of Florence, Italy, although
including professional guidance, was carried out according to a method of conducting that
was different and substantially simplified in comparison with the method illustrated in
Section 2.2, in particular based on the immersion in nature with mindful use of the senses
of sight, hearing, touch and smell.
Volunteer participants were enrolled and insured by local sections of the Italian Alpine
Club following information spread by means of standard channels (newsletters, social
media, etc.). No selection was applied except for age (>18 years) and the requirement of
being healthy. Participants were allowed to attend only one session, to prevent any contri-
bution from the possible persistence of the effects. Overall, 207 participants were recruited,
returning 162 valid self-assessment questionnaires, the nature of which is described below
in Section 2.1. Table 1 shows the basic information about forest therapy sessions.
Table 1. Basic features of forest therapy sessions performed in Italy.
Session
Place, Municipality/Date/
Initial Time 1
Lat/
Lon/
Altitude
Weather, Temperature/
Tree Species/
Water Bodies—Streams
TVOC
Average (Peak)
Unit: µg/m3
Participants/
Valid Question-
naires 2/Gender 3
FTS1
Torre dei Sogni, Empoli and
Montespertoli (FI)
22 August 2020
14:30
43◦41 11.77 N
11◦0 0.69 E
100–200 m
Sunny, weak wind, 30 ◦C
Cypress, maritime pine,
holm oak, lentisk
68 (120)
35
24
M: 11; F: 13
FTS2
Monte Duro, Vezzano sul
Crostolo (RE)
6 September 2020
08:30
44◦32 34.49 N
10◦32 26.49 E
500–600 m
Sunny, calm, 23 ◦C
Scots pine, field maple,
black and white hornbeam,
elderberry, dogwood
27 (50)
35
21
M: 8; F: 13
FTS3
Parco del Respiro, Fai della
Paganella (TN)
11 September 2020
13:30
46◦10 33.25 N
11◦4 39.98 E
900–1000 m
Sunny, calm, 22 ◦C
Spruce, beech
Water streams, waterfalls
38 (108)
39
33
M: 8; F: 25
FTS4
Parco del Respiro, Fai della
Paganella (TN)
12 September 2020
08:30
46◦10 33.25 N
11◦4 39.98 E
900–1000 m
Sunny, calm, 17 ◦C
Spruce, beech
Water streams, waterfalls
28 (65)
22
17
M: 5; F: 12
FTS5
Battisti Refuge, Ligonchio
(RE)
27 September 2020
08:00
44◦15 42.24 N
10◦24 45.58 E
1750 m
Cloudy, windy, 4 ◦C
Beech, silver fir, mountain
pine
10 (20)
9
8
M: 5; F: 3
FTS6
Torre dei Sogni, Empoli and
Montespertoli (FI)
17 October 2020
14:00
43◦41 11.77 N
11◦0 0.69 E
100–200 m
Partly cloudy, weak wind,
15 ◦C
Cypress, maritime pine,
holm oak, lentisk
50 (90)
21
18
M: 11; F: 13
FTS7
Fonte del Borbotto, San
Godenzo (FI)
18 October 2020
09:00
43◦52 57.78 N
11◦41 10.65 E
1250–1350 m
Sunny to cloudy, calm, 7 ◦C
Beech, scattered silver fir
Water streams, pond
15 (30)
33
29
M: 12; F: 17
FTSC
Villa Vogel urban park,
Firenze (FI)
23 June 2021
09:00
43◦46 33.54 N
11◦12 23.89 E
39 m
Sunny, calm, 28 ◦C
Holm oak, stone pine and
other species
Water pond
15 (56) 4
13
12
M: 8; F: 4
1 Local solar time. 2 Number of self-assessment questionnaires further considered for analysis. 3 Data referred to valid questionnaires
(M: male; F: female). 4 Urban park surrounded by buildings and trafficked roads. TVOC levels could not be considered representative of
plant emissions.
′″
Int. J. Environ. Res. Public Health 2021, 18, 9509
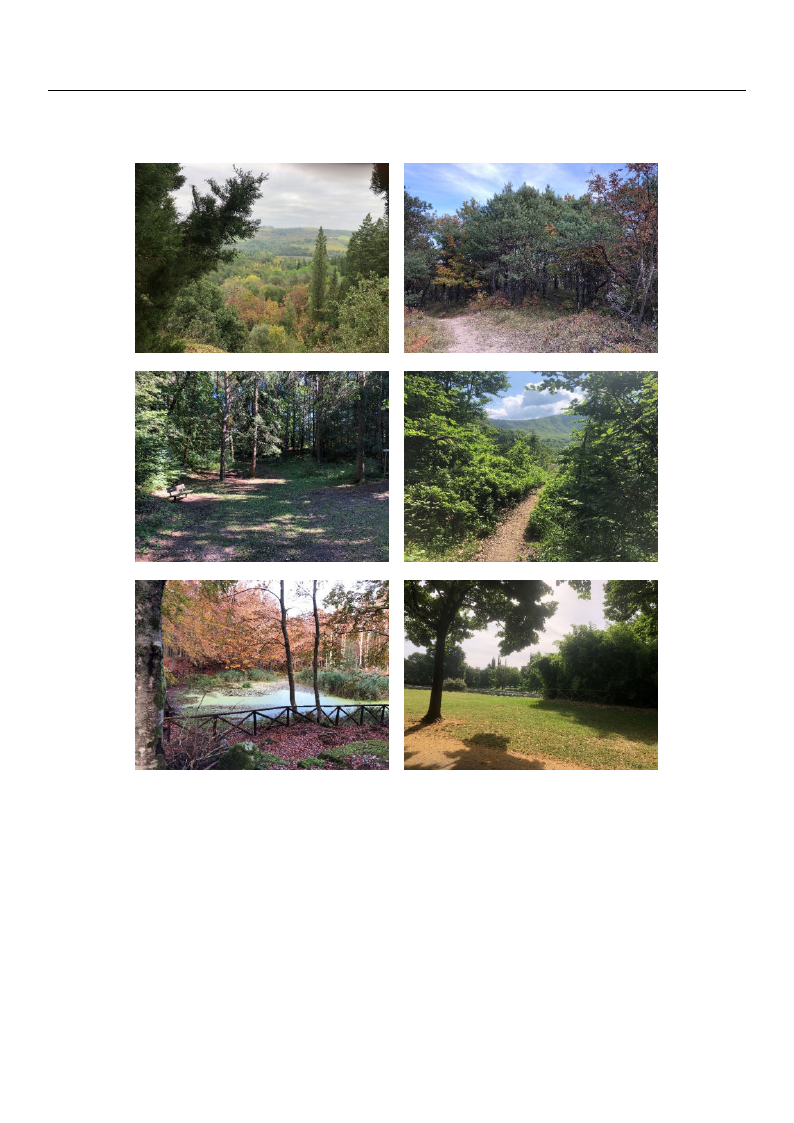
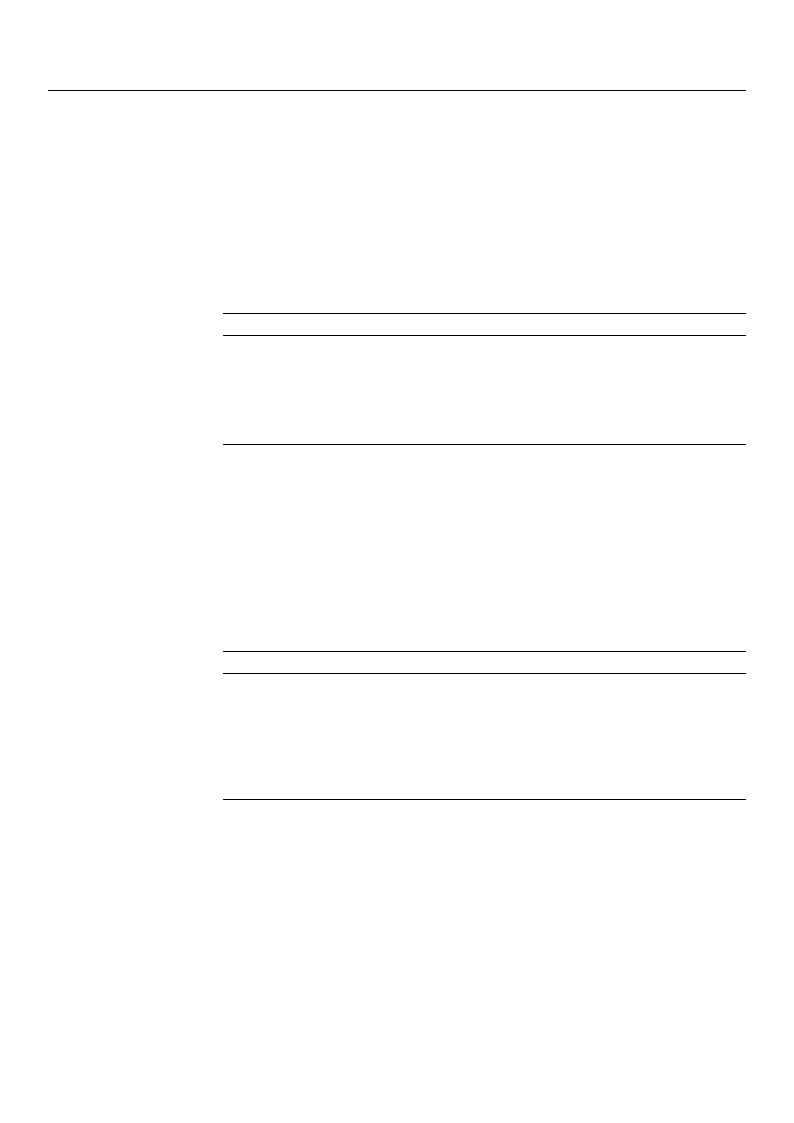
Figure 2a–f shows representative pictures of forest therapy sites.
6 of 21
(a)
(b)
(c)
(d)
(e)
(f)
Figure 2. Representative pictures of forest therapy sites: (a) FTS1 and FTS6; (b) FTS2; (c) FTS3 and FTS4; (d) FTS5; (e) FTS7;
(f) FTSC.
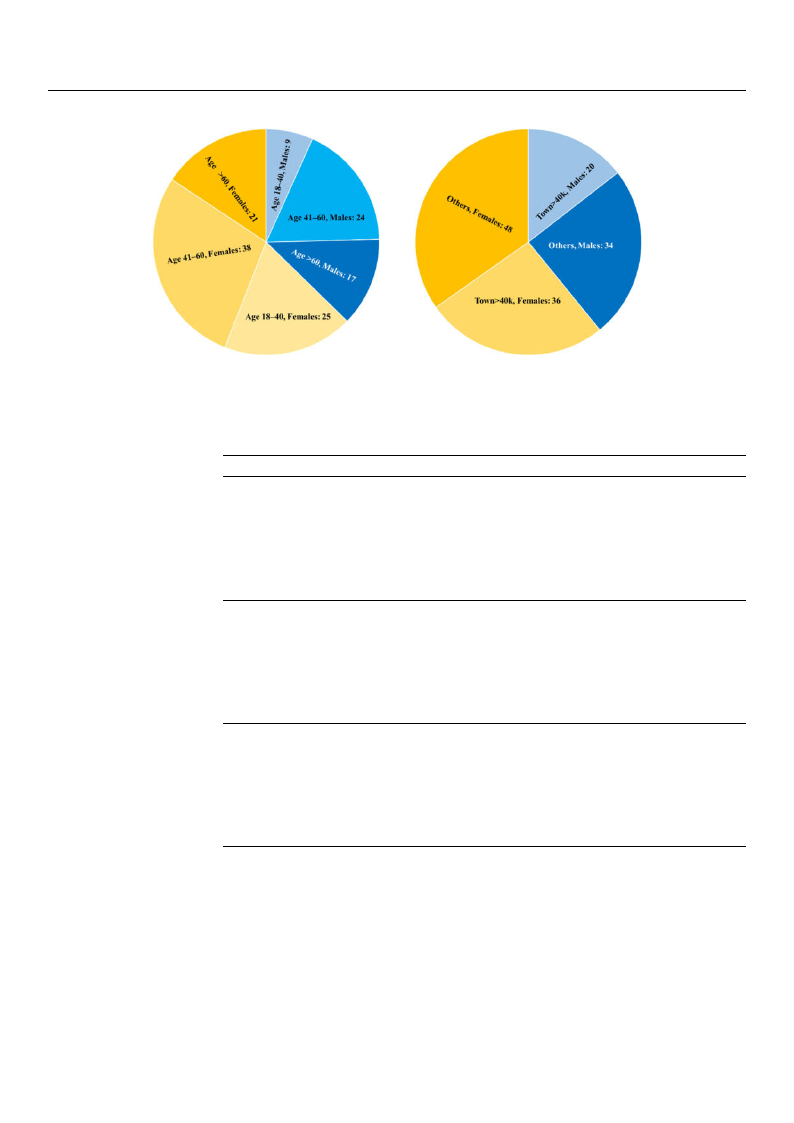
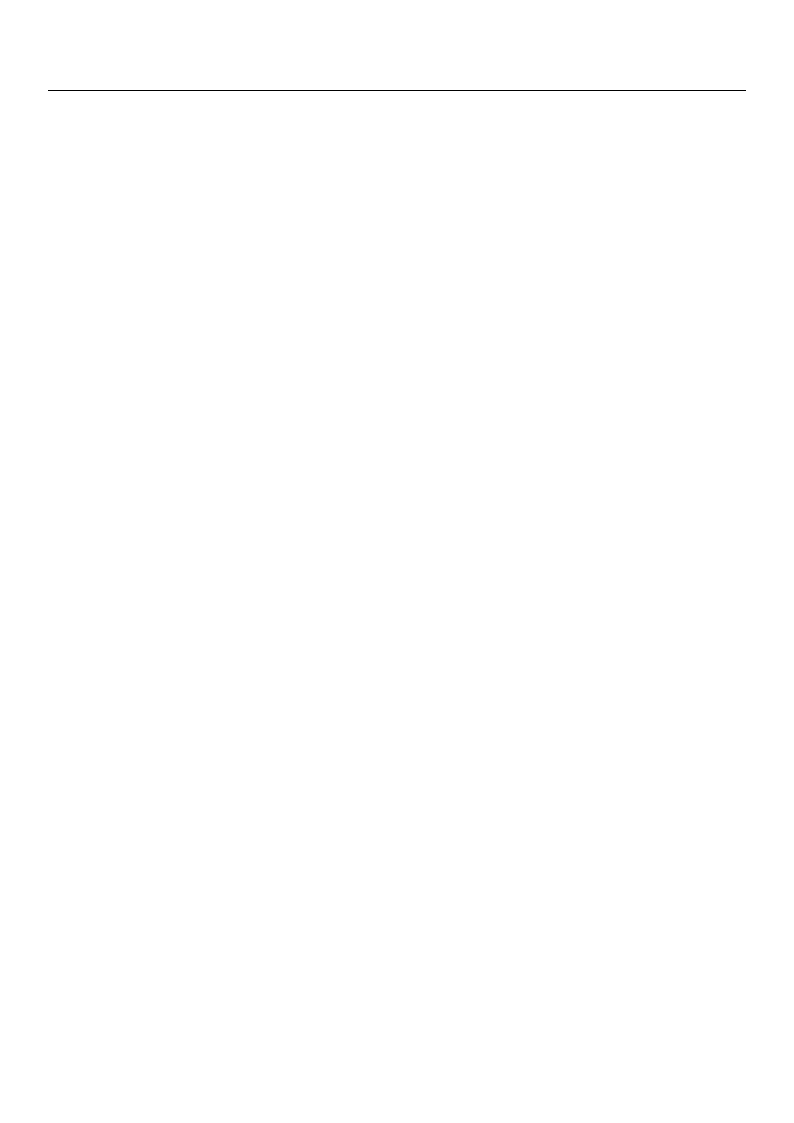
Limited to participants that returned valid questionnaires and relevant demographic
data, there were more female (84) than male (50) participants, the age group 41–60 was the
most represented for both genders (almost half of total) and the place of residence of more
than 59% of participants was outside towns with more than 40,000 inhabitants. Figure 3a,b
shows the basic demographic features of participants to forest therapy sessions.
Ryan–Joiner test for normality was performed for height and weight variables for the
entire study population, resulting in a non-normal distribution (height: p = 0.044; weight:
p < 0.01). Moreover, chi-square test matrix for homogeneity among categorical variables
was performed for the entire study population for sex, study degree, job, smoking and
residence variables, resulting in homogeneity only for sex variable (p = 0.182). Table 2
shows the data about age, height and weight for each forest therapy session.
Int. J. Environ. Res. Public Health 2021, 18, 9509
7 of 21
(a)
(b)
Figure 3. Basic demographic features of participants to forest therapy sessions: (a) Distribution by age group and gender;
(b) Distribution by residence and gender.
Table 2. Data about age, height and weight of participants to each forest therapy session.
Variable
Age
Height
Weight
Session
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
Number of Available Data
24
21
33
16
8
17
29
12
23
21
33
16
8
17
29
12
24
21
33
16
8
16
29
12
Mean ± Standard Deviation
52.42 ± 10.32
52.86 ± 9.89
45.58 ± 16.84
44.94 ± 15.15
64.38 ± 7.89
50.76 ± 14.37
51.83 ± 11.69
57.67 ± 15.74
170.74 ± 9.25
170.67 ± 9.03
165.36 ± 8.22
164.13 ± 7.45
166.25 ± 8.46
170.29 ± 11.54
170.28 ± 11.32
170.92 ± 8.84
69.04 ± 10.59
70.52 ±13.24
58.97 ± 15.36
57.56 ± 6.46
71.13 ± 11.43
70.06 ± 13.98
69.62 ± 19.47
72.08 ± 16.75
Participants reached the forest therapy site by car, and the informed consent was
collected on site and in written form from every participant before each session. Overall,
at least half an hour, and up to one hour, elapsed before participants started the forest
therapy session, during which every participant was presented also with a reduced Profile
of Mood States (POMS) questionnaire and listened to a short speech. Such time could
have helped relieving transport-related stress. The POMS questionnaire was completely
anonymous and included information about gender, age, place of residence, job and habits
such as smoking and sports. The POMS questionnaire consisted of 34 questions about
moods perceived at that precise moment, recommended for the analysis of psychological
outcomes of forest therapy sessions [38] and derived from previous studies on sport
psychology [39]. The same questionnaire was recently used in an investigation of stress

Int. J. Environ. Res. Public Health 2021, 18, 9509
8 of 21
reduction of healthcare staff after a short break in nature [40]. However, since no validation
study could be found regarding the specific subset of POMS items, it was decided to limit
the analysis to the psychological domains for which all the items were also included in the
originally validated questionnaire [39]. Thus, the considered domains were the mood states
of anxiety (also called tension in the original version), depression, anger and confusion
according to the recommended classification [39]. The POMS questionnaire was filled
immediately before and after the session. For each questionnaire, single answers to any of
the items were grouped to provide the above-mentioned synthetic indices. Only completely
filled questionnaires were considered for further analyses.
2.2. The Method of Conducting the Forest Therapy Sessions
Except for session FTS1, and for session FTSC that was carried out according to
a different and simplified method of conducting referred to in Section 2.1, a professional
psychologist or psychotherapist took part in each of the other forest therapy sessions,
according to a program named Forestfulness®, partly based on mindfulness practices, in
particular on the Mindfulness-Based Stress Reduction (MBSR) program developed since
1982 [19]. Mindfulness-based meditation is a way to pay attention to the present moment
by observing and accepting whatever experience is occurring.
Mindfulness was shown to reduce pain in a wide range of clinical and non-clinical
problems [41], improve immune functions [42], improve mental health in breast cancer
patients [43], create a higher subjective wellbeing and attenuate emotive reactivity [44],
reduce relapses in depression and blood pressure [45], reduce anxiety and improve mood
state [46]. Mindfulness practiced in forest environments showed significant and remarkable
therapeutic superiority over similar activities carried out in non-forested environments, for
example, in the treatment of depressive symptoms [20].
In the forest environment, mindfulness can be practiced by means of walking mind-
fully, using breathing as the center of attention, observing the surrounding environment
with acceptance and creating a deep connection with nature using the five senses. Walking
meditation is one of MBSR’s main practices, while walking in forests can lower blood
pressure and reduce the concentration level of cortisol (also named the stress hormone),
resulting in relaxation [47,48]. Walking meditation is performed by bringing the attention
to the physical sensations coming from breathing and walking. Although this exercise
could produce good results also indoor or in urban environments, higher benefits were
observed in the woods, including improvement in mood state [49].
Conscious and focused use of all human senses—sight, hearing, smell, touch and
taste—is another milestone of the MBSR program as a means to increase the awareness of
the experience and amplify the effects of forest immersion. Through the perception of the
surroundings, senses provide orientation, rooting into the present an interpretation of our
experiences [50,51]. Indeed, benefits for health from the exposure to forest environments
are effectively conveyed by the mediation of all human senses [33,52,53], which further
motivates the conscious focusing on human senses during forest therapy sessions.
Moreover, in the conduction of the forest therapy sessions, a method of communication
was adopted, which alternated metaphorical speeches with literal verbalizations in order to
stimulate increased emotional involvement in the participants [54]. In the past, the use of
metaphor was considered more an art than a scientific instrument [55], although one with
therapeutic value [56]. However, more recently, this classification has been questioned,
with interesting practical implications. For example, it was established that the educational
metaphors are useful for simplifying difficult concepts during class lessons [57]; in the
clinical field, metaphors help in understanding delicate health conditions [58] and can
be useful for developing scientific theories [59]. In everyday life, metaphorical language
is a tool that is able to promote and guide thought processes and to activate cognitive
maps for problem solving [60]. From a therapeutic point of view, metaphorical discourses
represent a cornerstone of Ericksonian and Neo-Ericksonian Hypnotic Psychotherapy;

Int. J. Environ. Res. Public Health 2021, 18, 9509
9 of 21
for example, a recent study demonstrated the effectiveness of Mindful Hypnotherapy to
reduce stress and create mindfulness [61].
In the context of forest therapy sessions, the attention of the participants to the present
moment was stimulated in order to promote a more effective immersion, in addition
through the conscious use of the five senses, the breath and the movement, looking for
the deep connection with the surrounding environment. Both mindfulness practices and
metaphorical discourses contributed to this purpose, as they could anticipate or deepen
the proposed experience at an imaginative and evocative level and prepare neural maps
for what will be physically practiced. Some neuroimaging studies showed that metaphors
activated cortical areas corresponding to the suggested action; for example, the expression
“she grabbed the idea” could activate the motor cortex [62].
During the structured forest therapy sessions (FTS2 to FTS7 listed in Table 1), in order to
stimulate the sensory activities, the participants were invited to “savor the experience”, to
“touch with the eyes the surrounding environment” and to “listen to their emotions”, to name
a few. The words chosen in these verbalizations aimed at several purposes:
• Generating a sensation of coherence between the internal dimension (feeling) and
the external dimension (acting calmly). The sense of coherence (internal–external),
in accordance with temperament and emotional intelligence, seems predictive of the
individual’s ability to cope with stressful situations [63];
• Facilitating processes of introspection and decoding of the feelings and emotions of
the participants to feed a condition of conscious presence;
• Promoting processes of identification with the elements of nature, which are in dy-
namic balance and can offer more effective learning and working models [64];
• Stimulating the transformative activity of any dysfunctional aspects detected [65].
The method of conducting the forest therapy sessions was structured in six main
steps, briefly:
1. Right attitude and entrance into the woods: Leave behind challenging thoughts, and
smile as if meeting with an old friend;
2. Wearing the most beautiful dress: Embrace the silence, leave behind planning and
commitments, gain space for the emergence of one’s own best part;
3. Walking mindfully: Involves bringing attention to any sensation coming from the feet
in order to keep the wandering mind anchored;
4. Breathing in the woods: By observing the breathing, it is possible to tune in with the
environment and to be aware of the state of mind and body as well; consequently, let
it all go, such as tensions, thoughts and feelings;
5. Using the senses: Intentionally looking at the surrounding environment or a natural
object that is found to be relaxing, recognizing wood fragrances during breathing,
concentrating on typical forest soundscape (birds, wind through the trees, crunch of
branches and leaves underfoot, etc.), touching wood and trees and, when possible,
tasting products of the undergrowth;
6. Meditating with the trees: Choosing a specific tree as the most faithful mirror of
oneself and approaching it with the right attitude and intentions, towards the identifi-
cation with the tree and its qualities such as resilience, vitality and projection towards
the sky and the light.
2.3. Data Analysis
Data reported on the reduced POMS questionnaires described in Section 2.1 were
transferred to Microsoft Excel worksheets. Psychological indices were obtained from the
questionnaires’ data by adding the values of the corresponding items according to the
recommended classification [39]. In addition, the TVOC data collected from the PID were
transferred from the proprietary software of the instrument to Microsoft Excel, and average
and peak concentration levels along the forest therapy paths were computed.
Pre-post average percentage differences of the outcomes for each considered mood
state were computed for each session based on data stored in Microsoft Excel worksheets.
Int. J. Environ. Res. Public Health 2021, 18, 9509
10 of 21
Domain
Anxiety
Depression
Anger
Confusion
Then, Minitab 19 was used for further statistical analyses. One-way ANOVA was preferred
since the samples were small in number and with quasi-normal distributions. For non-
normal samples, the Mann–Whitney test was used. The Ryan–Joiner test was used to
test for normality of continuous variables, while the chi-square test was used to test
for homogeneity among categorical variables. An ANOVA mixed-effects model was
used to test for associations between pre and post changes of each POMS domain and
sociodemographic features.
3. Results
3.1. Overall Psychological Outcomes
In order to ensure that the comparison among different sessions would not be affected
by statistically significant differences in initial mood states (i.e., baseline), a one-way
ANOVA test was performed on the pre-intervention POMS questionnaires [39] across
all forest therapy sessions including the control session (FTSC). The results showed no
statistically significant differences among groups in terms of pre-intervention scores for
all mood states: anxiety (DF = 7; DF error = 154; F = 1.59; p = 0.141), depression (DF = 7;
DF error = 154; F =1.66; p = 0.124), anger (DF = 7; DF error = 154; F = 0.64; p = 0.725) and
confusion (DF = 7; DF error = 154; F = 1.71; p = 0.111). Table 3 shows the relevant statistics.
Table 3. POMS pre-intervention domain scores.
Session
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
Number of Available Data
24
21
33
17
8
18
29
12
24
21
33
17
8
18
29
12
24
21
33
17
8
18
29
12
24
21
33
17
8
18
29
12
Mean ± Standard Deviation
2.125 ± 3.687
2.714 ± 2.918
2.879 ± 2.955
4.180 ± 4.680
2.750 ± 2.605
3.833 ± 3.682
4.586 ± 4.280
1.750 ± 2.261
0.583 ± 1.886
1.000 ± 1.703
2.303 ± 3.127
2.353 ± 3.807
1.500 ± 2.268
2.500 ± 3.698
2.069 ± 2.434
0.750 ± 1.485
0.958 ± 2.579
1.000 ± 1.761
1.455 ± 1.922
1.529 ± 2.004
1.250 ± 1.753
1.500 ± 2.407
1.724 ± 1.869
0.583 ± 1.443
1.792 ± 2.604
1.905 ± 1.998
2.939 ± 2.487
2.882 ± 3.257
2.000 ± 2.070
3.889 ± 3.179
3.310 ± 3.547
1.500 ± 1.784
95% CI
(0.686; 3.564)
(1.176; 4.252)
(1.652; 4.106)
(2.47; 5.89)
(0.258; 5.242)
(2.172; 5.495)
(3.277; 5.895)
(−0.285; 3.785)
(−0.515; 1.682)
(−0.175; 2.175)
(1.366; 3.240)
(1.047; 3.658)
(−0.403; 3.403)
(1.231; 3.769)
(1.069; 3.068)
(−0.804; 2.304)
(0.138; 1.779)
(0.123; 1.877)
(0.755; 2.155)
(0.554; 2.505)
(−0.172; 2.672)
(0.552; 2.448)
(0.977; 2.471)
(−0.577; 1.744)
(0.670; 2.914)
(0.705; 3.104)
(1.982; 3896)
(1.549; 4216)
(0.057; 3.943)
(2.593; 5.185)
(2.290; 4.331)
(−0.087; 3.087)
The differences in scores for any mood states before and after forest therapy sessions
were tested; in particular, data were aggregated for intervention groups (FTS1 to FTS7),
while FTSC was tested separately. A one-way ANOVA was performed to test for pre–post
Int. J. Environ. Res. Public Health 2021, 18, 9509
11 of 21
differences in the aggregated intervention groups (FTS1 to FTS7) and in the control group
(FTSC), resulting in a statistically significant reduction in each POMS domain score for
the aggregated intervention groups, while the control group resulted non-significant for
each POMS domain. Table 4 shows the results, along with the respective F and p values.
The control group had a limited numerosity; thus, the observed trends toward a reduction
in any of the mood states might become statistically significant with a larger sample,
especially for anxiety (p = 0.191).
Table 4. Statistical significance of outcomes from forest therapy sessions aggregated intervention groups (FTS1 to FTS7) and
control group (FTSC).
Session
Intervention groups (FTS1 to FTS7)
Control group (FTSC)
Anxiety
↓
F = 59.62; p < 0.001
↔
F = 1.82; p = 0.191
Depression
↓
F = 24.64; p < 0.001
↔
F = 0.74; p = 0.399
Anger
↓
F27.48; p < 0.001
↔
F = 0.93; p = 0.345
Confusion
↓
F = 30.98; p < 0.001
↔
F = 0.43; p = 0.521
3.2. Specific Effects of Remote Forest Areas
The possible specific effects due to the remoteness of forest areas and the conditions
under which such effects could arise were investigated by means of the comparison of
outcomes (pre–post differences, i.e., change-from-baseline) of each intervention group
(FTS1 to FTS7) with the corresponding outcomes from the control group in the urban
park (FTSC).
First, Grubb’s test for outliers was performed on the changes-from-baseline for
all mood states derived from the answers to the POMS questionnaires [39] in order to
exclude potential outliers from the analysis (p < 0.05). For anxiety, only one outlier was
removed from session FTS7. For depression, one outlier was removed from each of the
following sessions: FTS1, FTS2 and FTS6. For anger, one outlier was removed from each of
the following sessions: FTS1, FTS2, FTS5, FTS6, FTS7 and FTSC. For confusion, only one
outlier was removed from session FTS1.
Next, a Ryan–Joiner test for normality was performed for the change-from-baseline of
each mood state derived from every forest therapy session. Table 5 shows the results of the
test, where only non-normal distributions are highlighted (p < 0.05).
Table 5. Results of the Ryan–Joiner test for normality of change-from-baseline for any mood state in
any forest therapy session. NN = non-normal; all other distributions were normal.
Session
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
FTSC
Anxiety
NN
NN
NN
Depression
NN
NN
NN
NN
Anger
NN
Confusion
A one-way ANOVA test was applied for comparing normal samples, while a Mann–
Whitney test was applied when the comparison involved at least one non-normal sample.
Table 6 highlights the cases in which a forest therapy session performed in a remote forest
area resulted in improvements of mood states significantly higher than in the FTSC (p < 0.05)
or close to significantly (0.05 ≤ p < 0.10). The latter were added because the limited number
of participants to certain forest therapy sessions might have hindered the achievement of
statistical significance.
Sessions FTS1, FTS2 and FTS5 showed no specific additional benefit compared to
the control session FTSC. Session FTS3 showed an improvement in anger significantly
Int. J. Environ. Res. Public Health 2021, 18, 9509
12 of 21
higher than FTSC and comparative improvements in depression and confusion close to
significance. Session FTS4 again showed an improvement in anger significantly higher
than FTSC and a comparative improvement in confusion close to significance. Session
FTS6 showed improvements in anxiety and confusion significantly higher than FTSC and
a comparative improvement in anger close to significance. Finally, session FTS7 showed
an improvement in anxiety significantly higher than FTSC and a comparative improvement
in anger close to significance.
Table 6. Statistically significant differences between outcomes from each forest therapy sessions FTS1 to
FTS7 and outcomes from the control session FTSC. Green arrows: p < 0.05. Blue arrows: 0.05 ≤ p < 0.10
(close to significance).
Session
FTS1
FTS2
FTS3
FTS4
FTS5
FTS6
FTS7
Anxiety
Depression
Anger
Confusion
↓ (p = 0.027)
↓ (p = 0.042)
↓ (p = 0.084)
↓ (p = 0.023)
↓ (p = 0.028)
↓ (p = 0.088)
↓ (p = 0.072)
↓ (p = 0.082)
↓ (p = 0.093)
↓ (p = 0.024)
3.3. Association of Pshycological Outcomes with Sociodemographic Traits
A mixed model ANOVA was applied to check for any statistically significant associa-
tion among the collected sociodemographic traits of the participants in the forest therapy
sessions, excluding the control session FTSC, and the respective changes-from-baseline for
any mood state. The variance estimation method was the restricted maximum likelihood
and the Kenward–Roger method was used for testing fixed effects. In total, 128 question-
naires were considered, reporting complete sets of sociodemographic information. Table 7
shows the considered factors and their respective values.
Table 7. Factors and respective values used in the mixed model ANOVA for the assessment of the
association of forest therapy outcomes (sessions FTS1 to FTS7) with sociodemographic traits.
Factor
Values
Age
Height
Weight
Job
Education
Residence
Smoke
Sport 5
From 18 onwards (integer)
Any (integer)
Any (integer)
IN; MA; RE; SO 1
SS; HS; UN 2
CI; VI 3
0; 1 4
0; 1; 2; 3 6
1 IN: intellectual worker; MA: manual worker; RE: retired; SO: social worker. 2 SS: secondary school; HS: high
school; UN: university and higher. 3 CI: city greater than 40,000 inhabitants; VI: village below 40,000 inhabitants.
4 0: not smoker; 1: smoker. 5 Sport is understood as a session of physical activity, indoor or outdoor, regardless
of the duration and intensity. 6 0: no sport; 1: 1 to 2 times a week; 2; 3 to 4 times a week; 3: more than 4 times
a week.
The results showed a statistically significant association of the change in anxiety with
sport activity (p = 0.035), in particular, the absence thereof (p = 0.020) with a negative coeffi-
cient, i.e., anxiety decreased significantly for people who never played sports. Changes in
depression were significantly associated with age (p = 0.031), with a positive coefficient, as
well as with sport (0.038), in particular, the absence thereof (p = 0.041), with a negative coef-
ficient. Changes in anger were significantly associated with sports (p = 0.011), in particular,
the absence thereof (p = 0.002), with a negative coefficient. Changes in confusion were not
significantly associated with any considered factors, although the association with age was
close to significance (p = 0.058) with a positive coefficient.

Int. J. Environ. Res. Public Health 2021, 18, 9509
13 of 21
4. Discussion
4.1. Analysis of Presented Results
Based on the results shown in Table 4, the outcomes (i.e., change-from-baseline) from
the intervention groups altogether (forest therapy sessions FTS1 to FTS7, totaling 150 valid
questionnaires) were statistically significant for any of the considered psychological do-
mains (anxiety, depression, anger and confusion). Thus, this study supports the hypothesis
that forest therapy sessions performed in remote forest areas are effective in improving the
considered psychological domains.
Conversely, none of the outcomes from the control group (session FTSC) were signifi-
cant, suggesting that remote forests, where sessions FTS1 to FTS7 were performed, could
bring specific benefits compared to urban forests. However, a main limitation of this study
was the small numerosity of the control group (12 valid questionnaires), which might have
hampered the significance of the respective outcomes.
In order to try to overcome the above-mentioned limitation and provide further insight
into the factors affecting the outcomes of forest therapy sessions, the outcomes from each
of the intervention groups were separately compared with the corresponding outcomes
from the control group. As presented in Section 3.2 and shown in Table 6, few sessions
performed in remote forest areas resulted in specific and significant benefits for some
psychological domains, compared with the control session performed in an urban park. In
particular, both FTS6 and FTS7 significantly outperformed FTSC for anxiety and close to
significantly for anger, while FTS3 and FTS4 significantly outperformed FTSC for anger and
close to significantly for confusion. FTS3 also outperformed FTSC for depression, but only
close to significantly. FTS6 showed the best results, also significantly outperforming FTSC
for confusion. Sessions FTS1, FTS2 and FTS5 did not significantly (or close to significantly)
outperform FTSC. Overall, these results suggest that performing forest therapy sessions at
remote sites could help to enhance its effects compared to urban settings, but only under
certain circumstances.
Excluding FTS1, which was conducted non-professionally, and FTS5, which was
affected by a small numerosity and relatively harsh weather conditions, what peculiar
characteristics could underlie the additional and significant benefits deriving from certain
forest therapy sessions performed in remote sites?
Based on Table 1, FTS6, which was the highest performing session, enjoyed the highest
average concentration of TVOCs and was the only one performed in a Mediterranean
forest, without water bodies or water streams. On the other hand, FTS3 enjoyed the second
highest average concentration of TVOCs (and the highest among peak concentrations) and,
similar to FTS4 (performed on the same site as FTS3), included fascinating water streams
and small waterfalls. Notably, FTS4 enjoyed very good weather comfort, similar to FTS3,
but substantially lower average and peak concentration of TVOCs. FTS7 suffered from
less comfortable weather compared to all the other sessions, along with lower average
concentration of TVOC, but included water streams and a fascinating natural pond. Finally,
FTS2 enjoyed very comfortable weather, concentration levels of TVOCs only slightly lower
than FTS4 and higher than FTS7 and did not include water streams or water bodies.
Based on the available data, essentially on the performances of FTS6 compared with
all the other sessions and of FTS3 compared to FTS4, the hypothesis could be advanced that
the concentration of TVOCs is an effective factor affecting the performance of professionally
conducted forest therapy sessions in remote forests. This can be regarded as an original
experimental result of this study.
However, the matter is further complicated by partially contrasting results about the
systemic absorption of MTs, which represent most of the BVOCs emitted by plants, which,
in turn, are likely to contribute substantially to the observed concentration of TVOCs. To
the best knowledge of the authors, only two studies dealt with this important topic. In
2015, Japanese scholars found that the serum concentration of α-pinene, but not of other
monoterpenes, increased by several folds after walking in a conifer forest for one hour [66].
In 2021, Spanish scholars found that the blood concentration of α-pinene, but not of other

Int. J. Environ. Res. Public Health 2021, 18, 9509
14 of 21
monoterpenes, increased by a much slighter extent and only in subjects starting from the
lowest baselines levels after walking in an evergreen broadleaf forest (holm oak as the most
representative species) for two hours [67].
Although very important and innovative, both studies [66,67] were affected at least
by small sample sizes, by the unknown individual levels of metabolic transformation rates
and by the limited exposure time. Moreover, the health effects produced by MTs could
follow pathways other than by systemic absorption, such as direct effects on the upper
respiratory tract and on the central nervous system through brain absorption [25]. However,
due to the great importance of α-pinene as an anti-inflammatory, analgesic, antioxidant,
anxiolytic, antidepressant and sedative, as well as an antiproliferative agent [25], the
results obtained in this study, although quite limited, could point to some impact of
BVOC concentration on the psychological outcomes after forest therapy sessions lasting
about 3.5 h. Clearly, the detailed analysis of the relative and absolute concentration of
the different monoterpenes available in TVOCs during further forest therapy sessions
involving large numbers of participants will help clarify the possible impact of different
BVOCs on short-term psychological outcomes.
Despite lower levels of weather comfort and concentration of TVOCs, FTS7 generated
few significant results compared with the control session FTSC. Conversely, a very good
weather comfort and concentration levels of TVOCs substantially higher than in FTS7 and
only slightly lower than in FTS4 did not allow session FTS2 to achieve any significant
result in comparison to FTSC, underperforming in comparison to all the other sessions.
The hypothesis could be advanced that water streams and water bodies play an important
role, as already arisen in previous studies, for example, in a controlled experiment using
virtual reality [68]. However, considering that FTS6 lacked water bodies or water streams,
the matter could be more complicated.
It is further hypothesized that the presence of water streams or water bodies is very
important, but only if appropriate to the specific environment. In fact, FTS6 outperformed
all the other sessions even in the absence of those elements, but one could not expect
their presence in a typically dry Mediterranean forest. Conversely, FTS2 underperformed
all the other sessions, and one would expect to find water streams in a mountainous
environment dominated by Scots pine. It remains unknown whether substantially higher
concentration levels of TVOCs at the site of FTS2 could compensate for a possibly less
efficient environment: ongoing research at that site might help clarify the issue. Indeed,
FTS2 was performed in late summer, while, for Scots pine forests, it was found that young
sprouts in late spring and early summer emit far more BVOCs than mature needles in late
summer [27].
Overall, the coherence among the main natural elements, sometimes called environ-
mental coherence [69], could play a distinct role in boosting the performance of forest
therapy sessions. This coherence could also help explain why FTS7, carried out in a very
humid mountain environment, performed quite well despite low concentration levels of
TVOC and limited weather comfort. Moreover, it should be noted that FTS3 and FTS4,
despite the difference in the concentration of TVOCs, produced very similar results con-
cerning the psychological domains, i.e., significantly better performances compared with
the control session for anger and close to significance for confusion (as well as for depres-
sion, but only in FTS3). The specific and coherent environment characterizing FTS3 and
FTS4 could have been an effective driver for improvements at least in anger and, likely, in
confusion. The possible role of environmental coherence is another original experimental
result of this study, although it requires further research in order to elucidate its nature
and importance.
Session FTS1, which produced no significant outcome compared to FTSC, was per-
formed in the same site as FTS6, although with a remarkably lower level of weather comfort
(temperature of 30 ◦C compared to 15 ◦C in FTS6) and according to a non-professional
method. FTS1 enjoyed the highest average and peak concentration of TVOCs across all
forest therapy sessions. Although the comparison between FTS1 and FTS6 could lead to

Int. J. Environ. Res. Public Health 2021, 18, 9509
15 of 21
hypothesize an important role for the method of conducting forest therapy sessions, with
professional guidance more effective in producing significant outcomes, the large difference
in weather comfort jeopardizes this hypothesis. Further experiments will be needed in
order to gain insight into this matter.
Based on Table 6, among the considered psychological domains, depression was the
least affected by the remoteness of the forest site, at least in comparison to anxiety, anger
and confusion. Possibly, items used to build the depression index would need longer forest
therapy sessions or regular repetitions for their effective marginal reduction in comparison
to sessions performed in urban settings.
The reasons why anxiety was significantly only reduced in FTS6 and FTS7 in compari-
son to the control are hard to assess. Possibly, they have to do with the forest environments
characterizing FTS6 and FTS7 (distanced, mostly brightly colored trees and relatively low
beech trees), which could be regarded as more relaxing, or less aggressive, than in FTS3
and FTS4 (dense, dark-colored spruce trees), but further ongoing field trials will hopefully
clarify this issue.
Overall, anger appears as the most affected psychological domain, having been signif-
icantly reduced in comparison to the control in FTS3 and FTS4 and close to significantly in
FTS6 and FTS7. Possibly, items used to build the anger index were representative of acute
conditions and could have been more easily reduced by means of forest therapy sessions
performed at remote locations. Finally, confusion was significantly reduced compared
to the control in FTS6 and close to significantly in FTS3 and FTS4. Beyond environmen-
tal coherence, the concentration level of TVOCs, which was substantially lower in FTS7
compared to FTS3, FTS4 and FTS6, could have contributed to the result.
Concerning the association of the psychological outcomes from intervention sessions
(FTS1 to FTS7) with the sociodemographic traits presented in Section 3.3, sporting habits
showed the highest degree of association, in particular, the absence of sports. In fact, the
latter was significantly and negatively associated with the size of reduction in anxiety,
depression and anger. The significant association with the absence of sport could mitigate
the missing information on duration and intensity, according to the definition of sports
presented in Table 7. An important question arises as to whether such association means
that people never practicing sport receive substantial benefits from simply walking, ir-
respective of the surrounding environment and method of conducting physical activity,
or the absence of sport is related to a reduced contact with nature and the immersion in
forest environments is the leading factor, irrespective of physical exercise. Further field
experiments will help resolve this issue.
Age was the other trait showing some association in particular with depression
(significant) and confusion (very close to significant). The benefits for depression and
confusion increased with age, which could be ascribed either to increasing trait levels of
such indices with age or to a greater sensitivity of older people to forest immersion. Again,
further research will help clarify this issue.
It is interesting to note that no other sociodemographic characteristics were significantly
associated with the results of this study: neither biometric features such as height and weight,
nor sex, job, education, residence and smoking habits. This evidence could mean that forest
therapy can be successfully applied to most people, irrespective of their conditions.
4.2. International Experiences
A recent systematic review on the effects of nature walks on states of anxiety and
depression evidenced clear and significant effects on anxiety but somewhat inconclusive
effects on depression [70], in agreement with the results of this study. However, most of
previous studies dealing with the short-term effects of forest therapy sessions, in particular,
using POMS questionnaires, appear to lack a proper consideration of the nature of the
statistical distributions of the changes-from-baseline. Thus, comparisons with the results of
this study are difficult to perform.
Research was performed in 2018 based on a 3-day structured forest therapy session
in a semitropical forest in Taiwan, mainly aimed at checking the effects on creativity and

Int. J. Environ. Res. Public Health 2021, 18, 9509
16 of 21
involving 21 participants (8 males, 13 females) across all age groups (52.0 ± 12.54 years,
from 25 to 70 years old) [71]. The analysis of POMS questionnaires returned only the
percentage changes from baseline, along with the Cohen’s d index for the assessment of the
size of the effect [72]. The following changes were presented: anxiety, −49%; depression,
−42%; anger, −38%; confusion, −33%. Based on the above-written, comparisons with this
study are worthless, let alone the fact that sessions considered in this study had much
shorter duration (around 3.5 h).
In a recent study performed in Italy over healthcare staff during the COVID-19 pan-
demic, 77 participants filled the same reduced POMS questionnaires used in this study, be-
fore and after short breaks (20–30 min) in nature (green areas nearby hospital facilities) [40].
The results showed improvements in all the psychological indices, which were greater
for staff directly involved in COVID-19 treatment areas, who were likely more stressed.
Throughout all participants, anxiety, depression and anger reduced by 60–66%, 53–56% and
47 to 84%, respectively, while confusion was reduced by 35–53%. Again, comparisons with
this study are hard to perform.
In a study performed in Taiwan, 128 middle-aged to elderly subjects were recruited
(43 males and 85 females, age range 45 to 86 years, on average 60.0 ± 7.44 years) to attend
structured forest therapy sessions focused on the activation of the senses [73]. Each session
included around 10 participants during 3 h, such duration being comparable to sessions
performed in this study, under conditions of high meteorological comfort. The analysis of
reduced POMS questionnaires returned the following changes: anxiety, −59%; depression,
−50%; anger, −55%; confusion, −44%.
A study was performed in Poland on young adults (21 participants, of which 12 were
males and 9 were females, with an age range between 21 and 29 years and an average age
23.86 ± 2.67 years) according to a forest therapy program structured over two days (indoor
and in forest) [74]. The analysis of reduced POMS questionnaires returned the following
changes: anxiety, −56%; depression, −54%; anger, −43%; confusion, −36%.
Another study was performed again in Poland on young adults based on structured
30-min walks [75]. The analysis of the reduced POMS questionnaires, referring to a conifer
forest, returned the following changes: anxiety, −53%; depression, −35%; anger, −34%;
confusion, −30%.
In a study performed in South Korea, 38 university students with a mean age of
around 22 years, with 24 males and 14 females, were assigned in equal numbers to a forest
therapy group or a control group [76]. The experimental group performed eight, one-hour-
long sessions once a week according to a structured program but without active guidance.
Reduced POMS questionnaires were presented to the participants at the beginning of the
first session and the end of the last session. Except for anger, all other indices improved
substantially: anxiety (−34%), depression (−42%) and confusion (−31%).
In the opinion of the authors, it would be useful to re-examine some of the above-
cited studies based on appropriate and standardized statistical methods in order to build
a really useful international database concerning the performance of forest therapy and the
determinants of the respective outcomes.
4.3. Limitations and Preliminary Technical Guidelines
A few important limitations affected this study. All the forest therapy sessions lasted
3.5 ± 0.5 h, thus, the dose effect could not be investigated. All professionally conducted
forest therapy sessions in remote forest areas followed the same program, thus the effect
of different programs could not be investigated. In this respect, a recent Korean study
performed with elderly individuals showed that forest therapy programs focused on
Qigong or active walking produced specific neuropsychological and electrophysiological
benefits, both beneficial for preventing dementia and relieving related health problems [77].
Moreover, the single session performed without professional guidance (FTS1) was affected
by a low level of weather comfort, which could have played an important role in the
respective insignificant results.
Int. J. Environ. Res. Public Health 2021, 18, 9509
17 of 21
Participants in the forest therapy sessions discussed in this study were allowed to
attend only one session, thus the frequency effect could not be investigated. Neither
the psychological trait conditions nor the follow-up conditions of the participants were
collected; thus, the possible persistence of effects could not be investigated either. Another
limitation was that participants were not asked about their personal frequentation of forest
or green areas, even if the collected information about personal sporting habits might give
some clues to this effect. The latter limitation could have introduced a bias in terms of
persistence of effects for some sessions. Moreover, further information on the duration
and intensity of sport, understood here as a session of physical activity, would be useful to
refine the analysis.
The administration of the POMS questionnaires to the participants allowed collecting
instantaneously perceived mood states, not corroborated by any measure on physiologi-
cal parameters. Only admittedly healthy participants were recruited, thus the effects on
individuals affected by psychological or physiological disorders could not be assessed.
Moreover, no health screening of participants was performed before the forest therapy
sessions, thus it cannot be excluded that some participants were affected at least by acute
physiological, psychological or psychiatric illnesses, or by alcohol and drug abuse.
Although representative enough of different outdoor forest environments in central
and northern Italy, the study sites could not be considered representative of all the pos-
sible environments; for example, chestnut forests, widespread in mid-mountain areas in
the Italian Apennines, were not investigated, along with coastal Mediterranean forests.
Moreover, elements other than forest species and few other natural features (e.g., water
streams or ponds) were not considered, such as artificial elements (fences, tables and chairs,
mountain retreats and their architecture, etc.). Although large enough in comparison
with other experiences reported in the literature, the investigated sample (sites, sessions
and number of participants) could not allow the disentangling of all the possible factors
affecting the considered psychological outcomes, as well as adequately representing all
the relevant age groups, genders and other sociodemographic characteristics. In particular,
the control session FTSC suffered from a relatively scarce number of participants. Finally,
only TVOCs concentration was measured, while individual monoterpenes are known to
potentially produce different and specialized health effects [25], which could be related to
the outcomes of forest therapy sessions.
It is planned to overcome most of the above-listed limitations in the ongoing research
across many other sites by using many more participants and including larger control
groups in urban settings across different seasons and performing more comprehensive
measures such as sociodemographic, psychological (trait and state) and physiological
measures, as well as measuring the relative and absolute concentrations of individual
BVOCs and MTs. In addition to extending the performance database, the continuation of
the study aims at more rigorously identifying the factors affecting the observed healing
effects and further linking the medical and forestry research, as recommended in a recent
study [11].
Another limitation concerns the considered health domains, which were focused only
on mood states. Within the psychological domain, for example, cognitive processes were
shown to receive distinct benefits from forest therapy [25,71] and would be worth being
investigated, such as currently occurring in the frame of a large European project aimed
at fostering knowledge about the relationship between Information and Communication
Technologies and Public Spaces [78].
Based on the results obtained in this study and within its limitations, the following
preliminary guidelines concerning the short-term amelioration of psychological indices
can be advanced. Meteorological comfort, environmental coherence and concentration
levels of TVOCs appear quite important in the determination of the outcomes, especially
contributing to specific additional benefits brought by forest therapy sessions performed
in remote forest areas. Contrary to anxiety, anger and confusion, the depression domain
seems not to receive specific benefits from the remoteness of the forest site. Older people

Int. J. Environ. Res. Public Health 2021, 18, 9509
18 of 21
could benefit more from forest therapy sessions, especially for depression and confusion.
People abstaining from sporting activities, and likely from regular contact with nature,
could benefit more from forest therapy sessions, especially for anxiety, depression and
anger. These preliminary guidelines could help to optimize forest therapy sessions, as well
as to plan suitable sessions targeted to specific groups of participants, for example, those
belonging to a given age group or following certain habits, or aimed at improving specific
psychological indexes.
4.4. Policy Guidelines
The mobilization of financial resources and the introduction of specific legislative
elements aimed at promoting, standardizing and regulating forest therapy programs
were deemed essential to the effective management of the forest ecosystems towards
human health [5]. More specifically, based on the evidence shown in this study, further
fundamental challenges consist in the information, education and motivation of health
facilities and professionals, as well as of citizens, towards green prescriptions, which have
been issued for years in countries such as Japan and South Korea [31].
Further important tasks concern the certification of sites based on structural and
environmental characteristics and direct functionality (observation of health effects), as
well as the certification of professional providers of services connected to forest therapy [34].
In the Western world, the Parks Prescription program introduced by the British Columbia
Parks Foundation in Canada aimed at the prescription of short and slow walks in protected
forest areas as a “superfood of exercise” could serve as a useful model [79].
5. Conclusions
The results achieved in this study confirm, reinforce and expand the knowledge about
the healing effects of forests by means of structured forest therapy sessions. The short-term
reductions in the levels of anxiety, depression, anger and confusion were all significant
for forest therapy sessions performed in remote areas and taken altogether, contrary to
a control forest therapy session performed in an urban park.
Specific effects of remoteness, in comparison to the control session, arose under certain
conditions with anxiety, anger and confusion but not for depression. Some characteristics
of the site appeared to affect the outcomes, especially the level of meteorological com-
fort, the concentration of TVOCs and the environmental coherence, as well as personal
characteristics of the participants, such as sporting habits and age.
Despite several limitations, a few preliminary technical guidelines were issued, which
could help to identify, design and optimize forest therapy stations and sessions also targeted
to specific groups of participants or improving specific psychological conditions.
Author Contributions: Conceptualization, M.A., R.B., F.R.B., D.D., F.F. (Fabio Firenzuoli), V.M., F.M.
and F.Z.; methodology, R.B., F.R.B., G.M., F.F. (Franco Finelli), F.M., S.N., L.N. and M.R.; software,
L.A. and F.M.; validation, M.A., R.B., F.R.B., F.C., D.D., F.F. (Franco Finelli), V.M., L.N. and F.F.
(Fabio Firenzuoli); formal analysis, R.B., F.M., F.F. (Fabio Firenzuoli) and F.Z.; investigation, L.A.,
F.C., F.M., S.N., M.R. and F.Z.; resources, G.M., F.M. and F.Z.; data curation, L.A., F.C. and F.M.;
writing—original draft preparation, F.M. and F.Z.; writing—review and editing, M.A., R.B., D.D., F.F.
(Fabio Firenzuoli), V.M., F.M., S.N., L.N., M.R. and F.Z.; visualization, L.A. and F.M.; supervision,
R.B., F.F. (Franco Finelli), F.F. (Fabio Firenzuoli), G.M., F.M., L.N. and F.Z.; project administration, F.F.
(Fabio Firenzuoli), G.M. and F.Z.; funding acquisition, F.R.B., F.F. (Franco Finelli), F.Z. and G.M. All
authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: The study was conducted according to the guidelines of
the Declaration of Helsinki and approved by the Institutional Review Board of National Research
Council and Italian Alpine Club (N.01/2021, 8 May 2021).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: All data are available by contacting the corresponding authors.

Int. J. Environ. Res. Public Health 2021, 18, 9509
19 of 21
Acknowledgments: The study could not have been performed without the invaluable support
of several Sections of the Italian Alpine Club, among which the Section of Reggio Emilia, the
Section of Firenze and the Section Valdarno Inferiore “Giacomo Toni”, as well as the Consorzio Fai
Vacanze (Fai della Paganella, Trento, Italy) and the Association Foresta Modello delle Montagne
Fiorentine (Florence, Italy). Giuliano Cervi, Sonia Cuseri and Giancarlo Tellini, as the president
of the Central Scientific Committee, president of the Tuscany Scientific Committee “Fiorenzo Gei”
and president of the Tuscany Regional Group of the Italian Alpine Club, respectively, are gratefully
acknowledged for their continuous support and advice. Finally, three anonymous Reviewers are
gratefully acknowledged for their careful and insightful comments and suggestions.
Conflicts of Interest: S.N. and M.R. are owners of the trademark Forestfulness®. The authors declare
no other conflict of interest.
References
1. Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-yoku (Forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ.
Res. Public Health 2017, 14, 851. [CrossRef]
2. Li, Q. Effect of forest bathing (shinrin-yoku) on human health: A review of the literature. Sante Publique 2019, 31, 135–143.
[CrossRef] [PubMed]
3. Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace
exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [CrossRef]
4. Corazon, S.S.; Sidenius, U.; Poulsen, D.V.; Gramkow, M.C.; Stigsdotter, U.K. Psycho-physiological stress recovery in outdoor
nature-based interventions: A systematic review of the past eight years of research. Int. J. Environ. Res. Public Health 2019, 16, 1711.
[CrossRef] [PubMed]
5. Dodev, Y.; Zhiyanski, M.; Glushkova, M.; Shin, W.S. Forest welfare services—The missing link between forest policy and
management in the EU. For. Policy Econ. 2020, 118, 102249. [CrossRef]
6. Andersen, L.; Corazon, S.S.; Stigsdotter, U.K. Nature Exposure and Its Effects on Immune System Functioning: A Systematic
Review. Int. J. Environ. Res. Public Health 2021, 18, 1416. [CrossRef] [PubMed]
7. Antonelli, M.; Donelli, D.; Carlone, L.; Maggini, V.; Firenzuoli, F.; Bedeschi, E. Effects of forest bathing (shinrin-yoku) on
individual well-being: An umbrella review. Int. J. Environ. Health Res. 2021, 1–26. [CrossRef] [PubMed]
8. Kim, H.; Lee, Y.W.; Ju, H.J.; Jang, B.J.; Kim, Y.I. An Exploratory Study on the Effects of Forest Therapy on Sleep Quality in Patients
with Gastrointestinal Tract Cancers. Int. J. Environ. Res. Public Health 2019, 16, 2449. [CrossRef] [PubMed]
9. Bielinis, E.; Jaroszewska, A.; Łukowski, A.; Takayama, N. The Effects of a Forest Therapy Programme on Mental Hospital Patients
with Affective and Psychotic Disorders. Int. J. Environ. Res. Public Health 2019, 17, 118. [CrossRef]
10. Buckley, R.; Brough, P.; Hague, L.; Chauvenet, A.; Fleming, C.; Roche, E.; Sofija, E.; Harris, N. Economic value of protected areas
via visitor mental health. Nat. Commun. 2019, 10, 5005. [CrossRef]
11. Doimo, I.; Masiero, M.; Gatto, P. Forest and Wellbeing: Bridging Medical and Forest Research for Effective Forest-Based Initiatives.
Forests 2020, 11, 791. [CrossRef]
12. Peterfalvi, A.; Meggyes, M.; Makszin, L.; Farkas, N.; Miko, E.; Miseta, A.; Szereday, L. Forest Bathing Always Makes Sense: Blood
Pressure-Lowering and Immune System-Balancing Effects in Late Spring and Winter in Central Europe. Int. J. Environ. Res. Public
Health 2021, 18, 2067. [CrossRef] [PubMed]
13. Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [CrossRef] [PubMed]
14. White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at
least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [CrossRef] [PubMed]
15. Tsao, T.M.; Tsai, M.J.; Hwang, J.S.; Cheng, W.F.; Wu, C.F.; Chou, C.C.K.; Su, T.C. Health effects of a forest environment on natural
killer cells in humans: An observational pilot study. Oncotarget 2018, 9, 16501–16511. [CrossRef]
16. Rajoo, K.S.; Karam, D.S.; Abdullah, M.Z. The physiological and psychosocial effects of forest therapy: A systematic review. Urban
For. Urban Green. 2020, 54, 126744. [CrossRef]
17. Markwell, N.; Gladwin, T.E. Shinrin-yoku (Forest Bathing) Reduces Stress and Increases People’s Positive Affect and Well-Being
in Comparison with Its Digital Counterpart. Ecopsychology 2020, 12, 247–256. [CrossRef]
18. Zabini, F.; Albanese, L.; Becheri, F.R.; Gavazzi, G.; Giganti, F.; Giovanelli, F.; Gronchi, G.; Guazzini, A.; Laurino, M.; Li, Q.; et al.
Comparative Study of the Restorative Effects of Forest and Urban Videos during COVID-19 Lockdown: Intrinsic and Benchmark
Values. Int. J. Environ. Res. Public Health 2020, 17, 8011. [CrossRef]
19. Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness
meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [CrossRef]
20. Rosa, C.D.; Larson, L.R.; Collado, S.; Profice, C.C. Forest therapy can prevent and treat depression: Evidence from meta-analyses.
Urban For. Urban Green. 2021, 57, 126943. [CrossRef]
21. Buckley, R.C.; Brough, P.; Westaway, D. Bringing Outdoor Therapies into Mainstream Mental Health. Front. Public Health 2018, 6, 119.
[CrossRef] [PubMed]

Int. J. Environ. Res. Public Health 2021, 18, 9509
20 of 21
22. Joye, Y.; van den Berg, A. Is love for green in our genes? A critical analysis of evolutionary assumptions in restorative environments
research. Urban For. Urban Green. 2011, 10, 261–268. [CrossRef]
23. Van den Berg, A.E. From green space to green prescriptions: Challenges and opportunities for research and practice. Front.
Psychol. 2017, 8, 268. [CrossRef] [PubMed]
24. Ikei, H.; Song, C.; Miyazaki, Y. Physiological effects of touching wood. Int. J. Environ. Res. Public Health 2017, 14, 801. [CrossRef]
25. Antonelli, M.; Donelli, D.; Barbieri, G.; Valussi, M.; Maggini, V.; Firenzuoli, F. Forest Volatile Organic Compounds and Their
Effects on Human Health: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2020, 17, 6506. [CrossRef]
26. Šimpraga, M.; Ghimire, R.P.; Van Der Straeten, D.; Blande, J.D.; Kasurinen, A.; Sorvari, J.; Holopainen, T.; Adriaenssens, S.;
Holopainen, J.K.; Kivimäenpää, M. Unravelling the functions of biogenic volatiles in boreal and temperate forest ecosystems. Eur.
J. For. Res. 2019, 138, 763–787. [CrossRef]
27. Taipale, D.; Aalto, J.; Schiestl-Aalto, P.; Kulmala, M.; Bäck, J. The importance of accounting for enhanced emissions of monoter-
penes from new Scots pine foliage in models—A Finnish case study. Atmos. Environ. X 2020, 8, 100097. [CrossRef]
28. Meneguzzo, F.; Albanese, L.; Bartolini, G.; Zabini, F. Temporal and Spatial Variability of Volatile Organic Compounds in the
Forest Atmosphere. Int. J. Environ. Res. Public Health 2019, 16, 4915. [CrossRef] [PubMed]
29. Bach, A.; Yañez-Serrano, A.M.; Llusi, J.; Filella, I.; Maneja, R.; Penuelas, J. Human Breathable Air in a Mediterranean Forest:
Characterization of Monoterpene Concentrations under the Canopy. Int. J. Environ. Res. Public Health 2020, 17, 4391. [CrossRef]
30. FAO; UNEP. The State of the World’s Forests 2020. Forests, Biodiversity and People; Food and Agriculture Organization of the United
Nations: Rome, Italy, 2020; ISBN 9789251324196.
31. Nabhan, G.P.; Orlando, L.; Smith Monti, L.; Aronson, J. Hands-On Ecological Restoration as a Nature-Based Health Intervention:
Reciprocal Restoration for People and Ecosystems. Ecopsychology 2020, 12, 195–202. [CrossRef]
32. Sen, M. Forests: At the Heart of a Green Recovery from the COVID-19 Pandemic; United Nations Secretariat: New York, NY, USA, 2020.
33. Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of nature therapy: A review of the research in Japan. Int. J. Environ. Res.
Public Health 2016, 13, 781. [CrossRef]
34. Buckley, R.C. Therapeutic mental health effects perceived by outdoor tourists: A large-scale, multi-decade, qualitative analysis.
Ann. Tour. Res. 2019, 77, 164–167. [CrossRef]
35. van den Bosch, M.; Meyer-Lindenberg, A. Environmental Exposures and Depression: Biological Mechanisms and Epidemiological
Evidence. Annu. Rev. Public Health 2019, 40, 239–259. [CrossRef] [PubMed]
36. Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig,
T.; et al. Nature and Mental Health: An Ecosystem Service Perspective. Sci. Adv. 2019, 5, eaax0903. [CrossRef] [PubMed]
37. Lee, I.; Choi, H.; Bang, K.S.; Kim, S.; Song, M.K.; Lee, B. Effects of forest therapy on depressive symptoms among adults: A
systematic review. Int. J. Environ. Res. Public Health 2017, 14, 321. [CrossRef]
38. Li, Q. Into the Forest. How Trees Can Help You Find Health and Happiness; Penguin Books Limited: London, UK, 2019; ISBN
9780241377604.
39. Grove, R.; Prapavessis, H. Preliminary evidence for the reliability and validity of an abbreviated Profile of Mood States. Int. J.
Sport Psychol. 1992, 23, 93–109.
40. Gola, M.; Botta, M.; D’Aniello, A.L.; Capolongo, S. Influence of Nature at the Time of the Pandemic: An Experience-Based Survey
at the Time of SARS-CoV-2 to Demonstrate How Even a Short Break in Nature Can Reduce Stress for Healthcare Staff. Health
Environ. Res. Des. J. 2021, 14, 49–65. [CrossRef]
41. Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J.
Psychosom. Res. 2004, 57, 35–43. [CrossRef]
42. Davidson, R.J.; Kabat-Zinn, J.; Schumacher, J.; Rosenkranz, M.; Muller, D.; Santorelli, S.F.; Urbanowski, F.; Harrington, A.; Bonus,
K.; Sheridan, J.F. Alterations in brain and immune function produced by mindfulness meditation. Psychosom. Med. 2003, 65,
564–570. [CrossRef] [PubMed]
43. Cramer, H.; Lauche, R.; Paul, A.; Dobos, G. Mindfulness-based stress reduction for breast cancer—A systematic review and
meta-analysis. Curr. Oncol. 2012, 19, e343. [CrossRef]
44. Keng, S.L.; Smoski, M.J.; Robins, C.J. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol.
Rev. 2011, 31, 1041–1056. [CrossRef]
45. Chiesa, A.; Serretti, A. A systematic review of neurobiological and clinical features of mindfulness meditations. Psychol. Med.
2010, 40, 1239–1252. [CrossRef]
46. Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The Effect of Mindfulness-Based Therapy on Anxiety and Depression: A
Meta-Analytic Review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [CrossRef] [PubMed]
47. Li, Q.; Otsuka, T.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Li, Y.; Hirata, K.; Shimizu, T.; et al. Acute
effects of walking in forest environments on cardiovascular and metabolic parameters. Eur. J. Appl. Physiol. 2011, 111, 2845–2853.
[CrossRef] [PubMed]
48. Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A
systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [CrossRef] [PubMed]
49. Farrow, M.R.; Washburn, K. A Review of Field Experiments on the Effect of Forest Bathing on Anxiety and Heart Rate Variability.
Glob. Adv. Health Med. 2019, 8, 216495611984865. [CrossRef]

Int. J. Environ. Res. Public Health 2021, 18, 9509
21 of 21
50. Nisbet, E.K.; Zelenski, J.M.; Murphy, S.A. Happiness is in our Nature: Exploring Nature Relatedness as a Contributor to Subjective
Well-Being. J. Happiness Stud. 2011, 12, 303–322. [CrossRef]
51. Franco, L.S.; Shanahan, D.F.; Fuller, R.A. A review of the benefits of nature experiences: More than meets the eye. Int. J. Environ.
Res. Public Health 2017, 14, 864. [CrossRef] [PubMed]
52. Bang, K.S.; Kim, S.; Song, M.K.; Kang, K.I.; Jeong, Y. The effects of a health promotion program using urban forests and nursing
student mentors on the perceived and psychological health of elementary school children in vulnerable populations. Int. J.
Environ. Res. Public Health 2018, 15, 1977. [CrossRef]
53. Tsunetsugu, Y.; Park, B.J.; Miyazaki, Y. Trends in research related to “shinrin-yoku” (taking in the forest atmosphere or forest
bathing) in Japan. Environ. Health Prev. Med. 2010, 15, 27–37. [CrossRef] [PubMed]
54. Citron, F.M.M.; Goldberg, A.E. Metaphorical sentences are more emotionally engaging than their literal counterparts. J. Cogn.
Neurosci. 2014, 26, 2585–2595. [CrossRef]
55. Kirmayer, L.J. Word magic and the rhetoric of common sense: Erickson’s metaphors for mind. Int. J. Clin. Exp. Hypn. 1988, 36,
157–172. [CrossRef] [PubMed]
56. Halley, J. Uncommon Therapy: The Psychiatric Techniques of Milton H. Erickson, M.D. Fam. Process 1973, 12, 467. [CrossRef]
57. Low, G. Metaphor and education. In The Cambridge Handbook of Metaphor and Thought; Gibbs, R.J., Ed.; Cambridge University
Press: Cambridge, UK, 2012; pp. 212–231.
58. Curran, J. Illness as Metaphor; AIDS and its Metaphors. BMJ 2007, 335, 517. [CrossRef]
59. Kuhn, T.S. Metaphor in Science. In Metaphor and Thought; Ortony, A., Ed.; Cambridge University Press: Cambridge, UK, 1993;
pp. 533–542.
60. Keefer, L.A.; Landau, M.J. Metaphor and analogy in everyday problem solving. Wiley Interdiscip. Rev. Cogn. Sci. 2016, 7, 394–405.
[CrossRef] [PubMed]
61. Olendzki, N.; Elkins, G.R.; Slonena, E.; Hung, J.; Rhodes, J.R. Mindful Hypnotherapy to Reduce Stress and Increase Mindfulness:
A Randomized Controlled Pilot Study. Int. J. Clin. Exp. Hypn. 2020, 68, 151–166. [CrossRef] [PubMed]
62. Boulenger, V.; Shtyrov, Y.; Pulvermüller, F. When do you grasp the idea? MEG evidence for instantaneous idiom understanding.
Neuroimage 2012, 59, 3502–3513. [CrossRef] [PubMed]
63. Szczes´niak, M.; Strochalska, K. Temperament and sense of coherence: Emotional intelligence as a mediator. Int. J. Environ. Res.
Public Health 2020, 17, 219. [CrossRef]
64. Kirmayer, L.J. Healing and the invention of metaphor: The effectiveness of symbols revisited. Cult. Med. Psychiatry 1993, 17,
161–195. [CrossRef] [PubMed]
65. Spurio, M.G. Words that heal. Psychiatr. Danub. 2015, 27 (Suppl. S1), S21–S27.
66. Sumitomo, K.; Akutsu, H.; Fukuyama, S.; Minoshima, A.; Kukita, S.; Yamamura, Y.; Sato, Y.; Hayasaka, T.; Osanai, S.; Funakoshi,
H.; et al. Conifer-Derived Monoterpenes and Forest Walking. Mass Spectrom. 2015, 4, A0042. [CrossRef] [PubMed]
67. Bach, A.; Maneja, R.; Zaldo-Aubanell, Q.; Romanillos, T.; Llusià, J.; Eustaquio, A.; Palacios, O.; Penuelas, J. Human absorption of
monoterpenes after a 2 -hs forest exposure: A field experiment in a Mediterranean holm oak forest. J. Pharm. Biomed. Anal. 2021,
200, 114080. [CrossRef] [PubMed]
68. Wang, X.; Shi, Y.; Zhang, B.; Chiang, Y. The Influence of Forest Resting Environments on Stress Using Virtual Reality. Int. J.
Environ. Res. Public Health 2019, 16, 3263. [CrossRef] [PubMed]
69. Talbot, J.F.; Kaplan, S. Perspectives on wilderness: Re-examining the value of extended wilderness experiences. J. Environ. Psychol.
1986, 6, 177–188. [CrossRef]
70. Kotera, Y.; Lyons, M.; Vione, K.C.; Norton, B. Effect of Nature Walks on Depression and Anxiety: A Systematic Review.
Sustainability 2021, 13, 4015. [CrossRef]
71. Yu, C.P.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban For. Urban Green. 2020,
51, 126670. [CrossRef]
72. Menardo, E.; Brondino, M.; Hall, R.; Pasini, M. Restorativeness in Natural and Urban Environments: A Meta-Analysis. Psychol.
Rep. 2021, 124, 417–437. [CrossRef]
73. Yu, C.P.; Lin, C.M.; Tsai, M.J.; Tsai, Y.C.; Chen, C.Y. Effects of short forest bathing program on autonomic nervous system activity
and mood states in middle-aged and elderly individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [CrossRef]
74. Bielinis, E.; Bielinis, L.; Krupin´ ska-Szeluga, S.; Łukowski, A.; Takayama, N. The Effects of a Short Forest Recreation Program on
Physiological and Psychological Relaxation in Young Polish Adults. Forests 2019, 10, 34. [CrossRef]
75. Janeczko, E.; Bielinis, E.; Wójcik, R.; Woz´nicka, M.; Ke˛dziora, W.; Łukowski, A.; Elsadek, M.; Szyc, K.; Janeczko, K. When urban
environment is restorative: The effect of walking in suburbs and forests on psychological and physiological relaxation of young
Polish adults. Forests 2020, 11, 591. [CrossRef]
76. Kim, J.G.; Jeon, J.; Shin, W.S. The influence of forest activities in a university campus forest on student’s psychological effects. Int.
J. Environ. Res. Public Health 2021, 18, 2457. [CrossRef] [PubMed]
77. Yi, J.; Kim, S.G.; Khil, T.; Shin, M.; You, J.H.; Jeon, S.; Park, G.H.; Jeong, A.Y.; Lim, Y.; Kim, K.; et al. Psycho-electrophysiological
benefits of forest therapies focused on qigong and walking with elderly individuals. Int. J. Environ. Res. Public Health 2021, 18, 3004.
[CrossRef] [PubMed]
78. CyberParks. COST Action TU 1306. Available online: http://cyberparks-project.eu/ (accessed on 23 August 2021).
79. Remick, R.A. A walk in nature: The superfood of physical activities. Br. Columbia Med. J. 2021, 63, 74.