
International Journal of Mental Health and Addiction (2022) 20:337–361
https://doi.org/10.1007/s11469-020-00363-4
ORIGINAL ARTICLE
Effects of Shinrin-Yoku (Forest Bathing) and Nature
Therapy on Mental Health: a Systematic Review
and Meta-analysis
Yasuhiro Kotera 1 & Miles Richardson1 & David Sheffield1
Published online: 28 July 2020
# The Author(s) 2020
Abstract
Shinrin-yoku, immersing oneself in nature using one’s senses, has been receiving in-
creased attention internationally. While most of the existing studies have focused on
physical health, this systematic review and meta-analysis examined the mental health
impacts of shinrin-yoku, using the PRISMA guidelines (PROSPERO registry:
BLINDED). Of 497 articles retrieved on databases including PubMed/MEDLINE,
PsycINFO, Science Direct and Google Scholar, twenty met the inclusion criteria. All
studies were conducted in Asia and Europe, and used a variety of different bathing
approaches (e.g. breathing, walking, yoga). While noting a need for more rigorous
research and extensive follow-up assessments, the findings indicate that shinrin-yoku
can be effective in reducing mental health symptoms in the short term, particularly
anxiety. More careful examination of shinrin-yoku practices is needed; longer follow-
up with participants from a range of countries along with greater examination of potential
mechanisms is needed for shinrin-yoku to be accepted into mainstream interventions.
Keywords Shinrin-yoku . Forest bathing . Nature therapy . Mental health . Meta-analysis
Shinrin-yoku (forest bathing) is a healing practice in Japan, where people immerse themselves
in nature, while mindfully paying attention to their senses. Often involving a walk in a forest, it
aims to integrate and harmonise humans with a forest (Miyazaki 2018). Contents of shinrin-
yoku programmes include breathing yoga, meditation, walking and other recreational activities
(e.g. cooking) that are often aimed at producing relaxation effects (Forest Therapy Society
2005). The word ‘shinrin-yoku (“森林浴”)’ was coined in 1982, for ‘yoku (bathing)’ implies
Electronic supplementary material The online version of this article (https://doi.org/10.1007/s11469-020-
00363-4) contains supplementary material, which is available to authorized users.
* Yasuhiro Kotera
Y.Kotera@derby.ac.uk
1 Human Sciences Research Centre, University of Derby, Derby, Derbyshire, England

338
International Journal of Mental Health and Addiction (2022) 20:337–361
the holistic nature of our health. Shinrin-yoku then began to be introduced into Japanese
clinical fields (Hansen et al. 2017).
Literature reviews reported diverse health benefits of shinrin-yoku: on immune system
functioning by increasing natural killer cells, and the cardiovascular and respiratory systems
(Williams 2016). The health benefits of shinrin-yoku are not limited to physical well-being;
improvements have been described in mood disorders and stress, and mental relaxation (Park
et al. 2012).
There are a number of theories that account for the health benefits of exposure to nature.
Kaplan’s Attention Restoration Theory claims that spending time in nature restores our
concentration through practice of effortless attention (Kaplan and Kaplan 1989). Stress
Reduction Theory asserts that being in an unthreatening natural environment reduces stress
and improves relevant physiological functions such as heartrate and blood pressure (Ulrich
et al. 1991). Indeed, Song, Ikei and Miyazaki noted that natural stimuli help to reduce stress
and strengthen our immune system. More recent studies explored the mechanism of shinrin-
yoku and found that the benefits of shinrin-yoku accord with Gilbert’s (2014) model of affect
regulation (Richardson et al. 2016). Although the benefits of nature for affect regulation are
often overlooked (Korpella et al., 2018), it is essential to health and well-being (Gross 2013).
Forest bathing and connecting with nature can help us regulate our emotions, through soothing
and calming (i.e. the parasympathetic system), instead of fear, anxiety and drive (i.e. sympa-
thetic system) (Richardson et al. 2016).
Humans are more familiar with spending time in nature than in urban environments: over
seven million years of human history, we have spent 99.99% of the time in nature (Miyazaki
2018); this may partially explain why we feel better in nature (Miyazaki 2018). Women living
in a green-rich area had a 12% lower rate of mortality than those living in a green-poor area
(James et al. 2016). Spending time in nature is related to lower rates of depression and high
blood pressure, and the frequent visits to nature was related to social cohesion (Shanahan et al.
2016). Participants who viewed a towering tree for 1 min scored high awe scores, associated
with more prosocial helping behaviours, than people who viewed a building with the same
height (Piff et al. 2015). A three-day shinrin-yoku programme increased the number and
activity of natural killer cells compared with 3 days of walking in a city (Li 2010). Likewise, a
90-min walk in nature reduced the level of rumination (negative repetitive thoughts, linking
with mental health problems) and the activities of subgenual prefrontal cortex (part of brain
that is related with mental health problems) (Bratman et al. 2015). Finally, there is recent
evidence that visits and time in nature may be acting as proxy measures for nature connect-
edness (Martin et al. 2020).
While our physical health has markedly improved in the twentieth century, our mental
health has arguably worsened (Mental Health Foundation 2016). In 1995, the World Health
Organization (WHO) launched an initiative called ‘Nations for Mental Health’ aiming to raise
awareness of mental health and innovate mental health treatment (WHO 2002). Mental health
action plan 2013–2020 was passed at the 66th WHO Summit, promoting universal mental
health care (WHO 2013). Approximately 1.1 billion people were estimated to have a mental
health problem in the world in 2016 (15% of the population): most prominent disorders being
anxiety (4%), depression (3%) and alcohol use disorders (1%; Ritchie and Roser 2018). The
global costs of mental illness were estimated about £2.5 trillion in 2010, which was projected
to increase to £6 trillion by 2030. About two-thirds of those costs are not directly associated
with mental health issues, for example, reduced productivity and income (Marquez and Saxena
2016). Among developed countries, the costs related to mental disorders are 2–4% of GDP

International Journal of Mental Health and Addiction (2022) 20:337–361
339
(Hewlett 2014), and they were estimated to be substantially higher in developing countries
(Patel 2007). Unsurprisingly, many countries have enacted government-led initiatives. For
example, in the UK, mental health has been high on the national agenda and the budget for
mental health care has been increasing (Department of Health 2011). In Japan, poor mental
health has also been a major national issue (e.g. the high suicide rates), and new policies for
supporting people with mental health problems were established in 2004, improving citizens’
mental health awareness and care (Ministry of Health, Labour and Welfare [MHLW] 2004).
This led to a revision of the law, further enhancing the country’s mental health care (MHLW,
2014).
These reports suggest that mental health is a worldwide concern, and affordable, accessible
and effective mental health solutions are needed. Treatment and care using nature may be one
solution that can satisfy those needs (Hunter et al. 2019). Some of the benefits have been
reviewed recently (Richardson et al. 2016; Farrow and Washburn 2019; Payne and Delphinus
2019), but no review has specifically focused on mental health benefits. Accordingly, the
present review systematically evaluated empirical findings noting the effects of shinrin-yoku
on mental health. The most prevalent mental health problems are depression, anxiety and
stress; therefore, these were our foci (Farmer and Dyer 2016). In addition, we also examined
whether shinrin-yoku’s effects on anger, as it is associated with depression, anxiety and stress
(Walsh et al. 2018).
Methods
The present article followed the preferred reporting items for systematic review and meta-
analysis (PRISMA; Moher et al. 2009) guidelines, to systematically review the literature and
appraise the quality of evidence for the mental health effects of shinrin-yoku. Additionally, to
maintain the validity of this systematic review, Klassen et al.’s (1998) framework was
employed, focusing on question, criteria, missing articles, quality of the studies, assessment
and results. The extended version of the PICO (population, intervention, control and out-
comes) format (Boland et al. 2013) was used to construct a researchable question by dissecting
the question into those components to help organise relevant information (Sackett et al. 1997).
The main research questions of this review were the following: (i) how effective is shinrin-
yoku in improving mental health outcomes? And (ii) what quantity and quality of evidence is
reported?
Literature Search
The literature search was conducted clarifying (i) where (i.e. databases), (ii) when the
literature was searched, (iii) who searched the literature, (iv) how (i.e. keywords), (v)
what amount of articles retrieved at each combination of the keywords and (vi) why
some articles were included/excluded (i.e. selection criteria) (Callahan 2010). Litera-
ture on PubMed/MEDLINE, PsycINFO, Science Direct and Google Scholar were
searched, after a consultation with a subject librarian. Articles published before the
30 October 2019 were searched in November 2019. The search terms ‘shinrin-yoku
(including ‘shinrin yoku’) (n=205), ‘forest bathing’ (n = 148) and ‘nature therapy’ (n =
129) retrieved 481 articles in total (‘nature therapy’ as synonymous with shinrin-yoku;
Hansen et al. 2017).
340
International Journal of Mental Health and Addiction (2022) 20:337–361
Eligibility Criteria
To be eligible for further analysis, articles needed to (i) be published in a peer-
reviewed academic journal using English language; (ii) employ a shinrin-yoku inter-
vention; (iii) report an empirical intervention study, using pre- and post-intervention
measures; and (iv) use mental health measures for depression, anxiety, stress and
anger. Exclusion criteria were articles that (i) were not interventions, (ii) were case
studies or qualitative studies and (iii) did not measure depression, anxiety, stress and
anger (Table 1).
Outcome Measures
Outcome measures were instruments that evaluate the levels of depression, anxiety, stress and
anger. Because there were various measurement tools used, we did not have principal
summary measures set. Mental health outcomes measured in the included studies were
depression (k = 19), anxiety (k = 22), anger (k = 14) and stress (k = 1).
Data Extraction and Synthesis
The lead author comprehensively examined the search results, and articles were shortlisted for
possible inclusion if the title and abstract indicated that the study might satisfy the eligibility
criteria. Additional manual reference searches on previous systematic reviews on shinrin-yoku
(n = 15) identified 16 additional articles that might fit with the inclusion criteria, thus
shortlisted (Rojon et al. 2011; Appendix 1). To counter any potential bias, the other co-
authors independently reviewed the entire selection process. Full papers of shortlisted articles
Table 1 Extended PICO for this review
Review How effective is shinrin-yoku in helping to improve mental health outcomes? What quantity and
questions quality of evidence is reported?
Inclusion criteria
Exclusion criteria
Population Any population
–
Intervention Shinrin-yoku (forest bathing)
Others (e.g. only examining one or few
and nature therapy
sensory stimulus such as smell of trees
or view of forest from a window;
combined with other therapies, except
for mindfulness and walking*).
Comparator Any comparator including no
–
intervention
Outcomes Mental health measures (depression,
Other measures used
anxiety, stress and anger) used at least at
pre- and post-intervention
Study
Empirical intervention study
Single case studies, qualitative studies,
design
reviews, discussion articles, articles introducing
theories/concepts/models/applications
Other
Published in a peer-reviewed academic Conference proceedings, theses, dissertations
journal in English
*Interventions combining shinrin-yoku and mindfulness and/or walking were included as they are common in
shinrin-yoku practice, immersing with nature while paying attention to five senses (Miyazaki 2018)

International Journal of Mental Health and Addiction (2022) 20:337–361
341
were independently reviewed by all co-authors. Lastly, a discussion was held among the co-
authors to confirm whether the selected articles had met the eligibility criteria and revisited the
excluded studies to ensure the reasons for exclusion were accurate (Appendix 2). Forward and
backward reference searches of relevant articles revealed no additional studies.
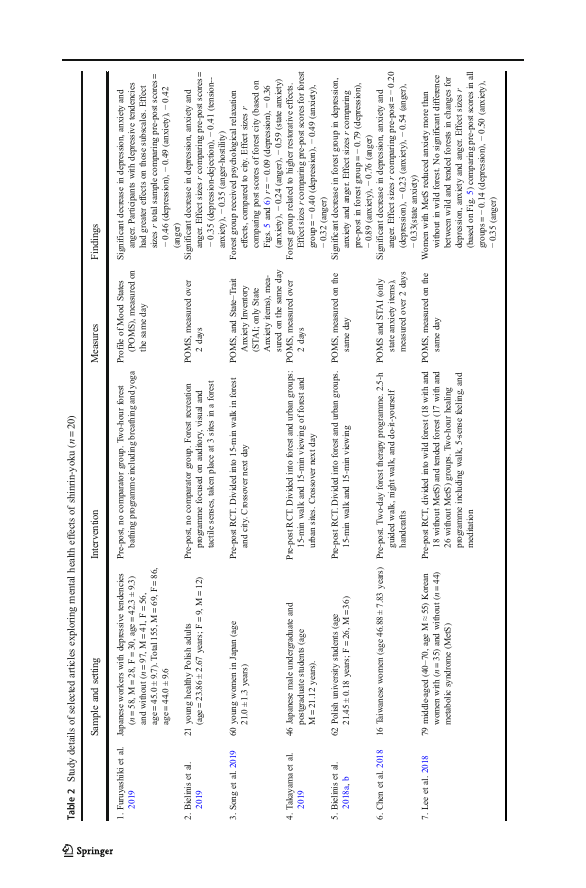
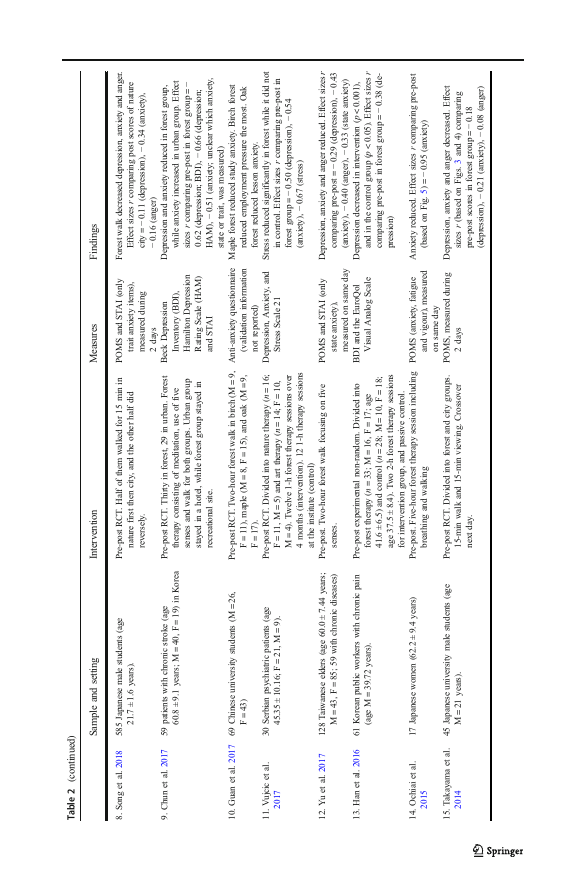
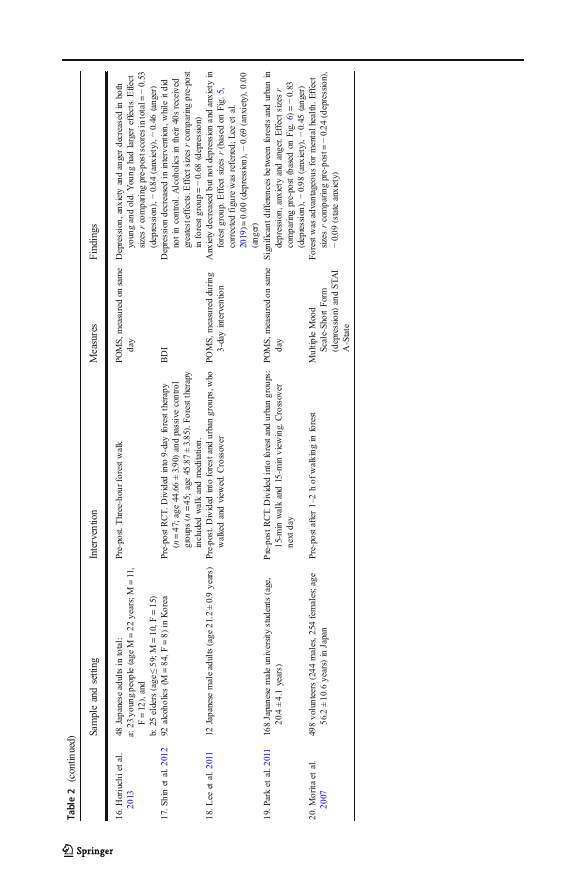
Data were extracted focusing on study aims, characteristics, participants, intervention
details, outcome measures and main findings (Table 2). Data were synthesised by the mental
health outcomes examined in the selected articles, further categorised into the four measures of
mental health—depression, anxiety, stress and anger (Table 3).
Meta-analyses were conducted focusing on depression, anxiety and anger; meta-analysis of
stress data was not possible (k = 1). We compared Pearson’s product-moment correlations to
determine effect size for the shinrin-yoku intervention. Data were entered into Meta-Essentials
(Van Rhee et al. 2015).
Variability was examined using Cochran’s Q and I2. Heterogeneity among effect sizes was
determined by a significant Q value (p < 0.10). The I2 statistic indicates the degree of
variability in effect sizes (low heterogeneity, 1–49; moderate heterogeneity, 50–74; high
heterogeneity, 75–100). In the case of significant heterogeneity, subgroup and moderator
analyses were undertaken.
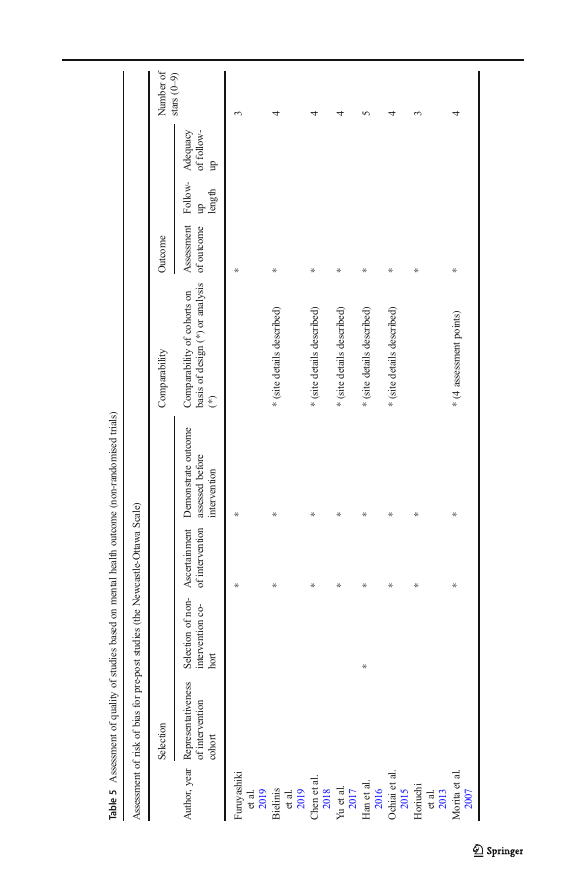
Quality Appraisal: Risk of Bias
The quality of the included non-randomised studies was assessed using the Newcastle-
Ottawa Scale (NOS; Wells et al. 2000). Using a star system, three assessors rate the
quality of studies from 0 to 9 stars (high risk, 0–3; medium risk, 4–6; low risk, 7–9) in
three domains: (i) representativeness of study group selection (max. 4), (ii) compara-
bility of groups (max. 2) and (iii) ascertainment of either the exposure or outcome of
interest (max. 3). Some adjustments were made to NOS because many of the included
studies recruited samples who had no mental disorders (while NOS was originally
developed for medical research attended by clinical samples): (i) the word ‘exposure’
was changed to ‘intervention’, (ii) the fourth scale item was changed from ‘Demon-
stration that outcome of interest was not present at start of study’ to ‘Demonstration
that the measured outcome was assessed before the intervention’ (because some mental
health outcomes exist before intervention, e.g. stress) and (iii) in respect of the first
item in the outcome assessment, a star was awarded if the outcome was assessed using
a validated scale (instead of medical records).
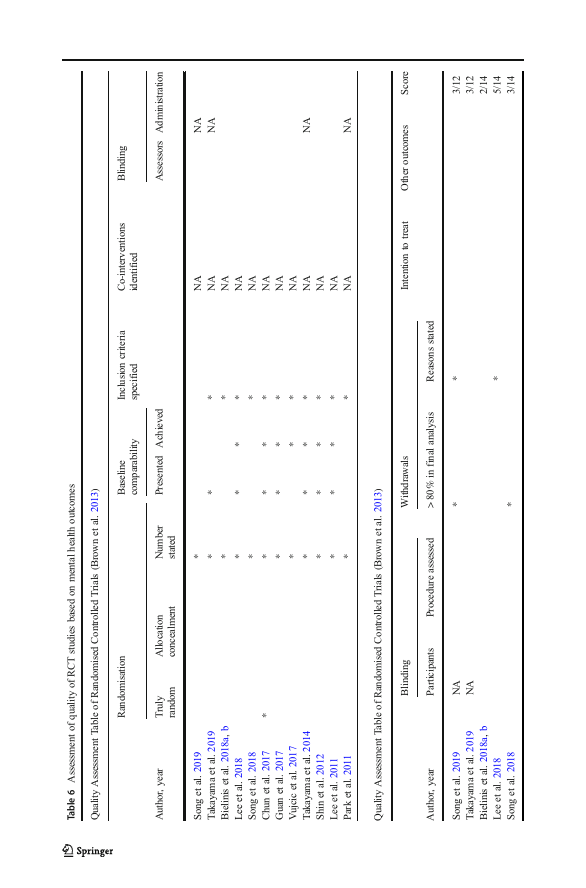
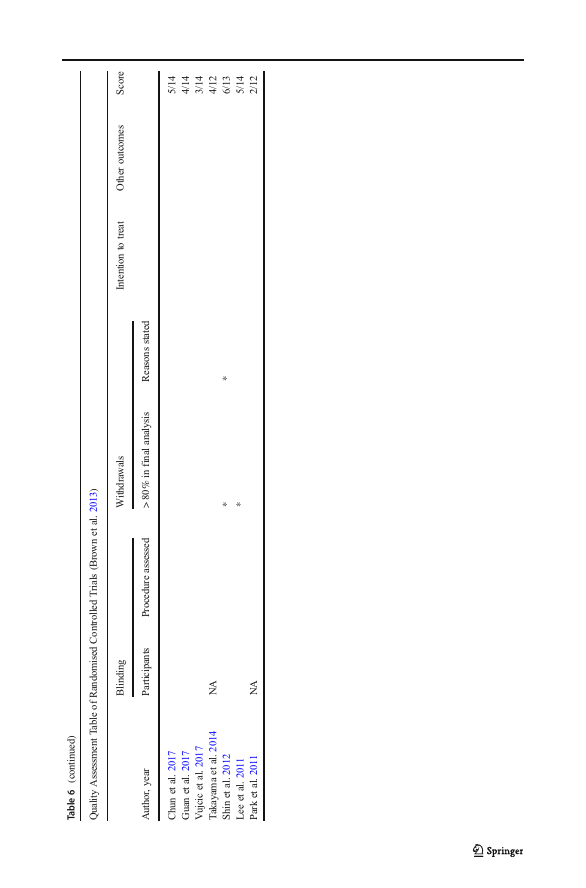
Randomised controlled trials were appraised using the Quality Assessment Table of
Randomised Controlled Trials (Brown et al. 2013).
Results
Search Results
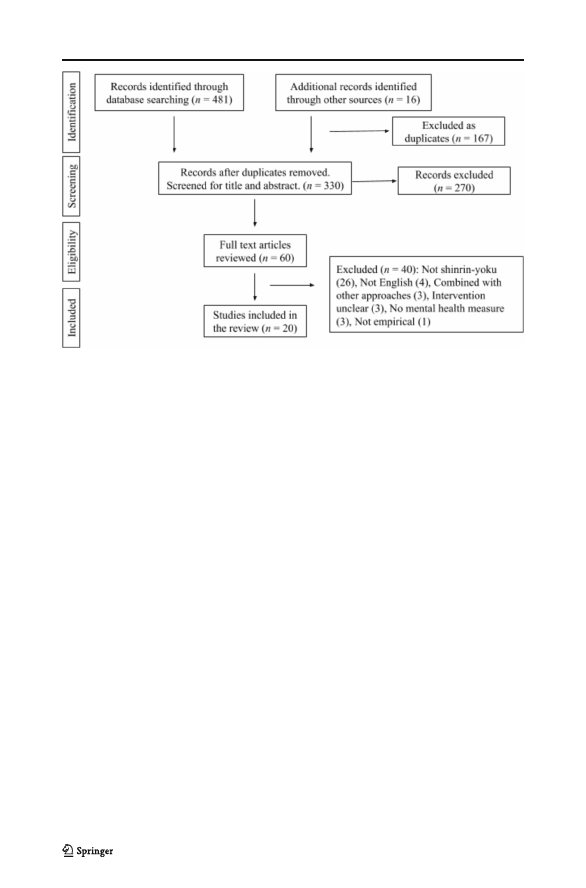
The article selection process was illustrated in Fig. 1. Of the 497 articles (481 from the
databases and 16 from manual reference search), 167 articles were removed for duplication.
The remaining 330 articles were screened for their title and abstract by authors. Sixty articles
were selected for full-text review, of which 40 were excluded (Appendix 2) and 20 were
included (Table 2).
342
International Journal of Mental Health and Addiction (2022) 20:337–361
International Journal of Mental Health and Addiction (2022) 20:337–361
343
344
International Journal of Mental Health and Addiction (2022) 20:337–361
International Journal of Mental Health and Addiction (2022) 20:337–361
345
Table 3 Included studies organised by mental health measures
Measured
outcome (s)
POMS STAI BDI (3) AAQ DASS (1) EQVAS (1) HDR (1) MMS (1)
(14)
(6)
(1)
Depression Anxiety Depression Anxiety Depression Depression/ Depression Depression
Anxiety
Anxiety anxiety
Anger
Stress
Furuyashiki ✓*
et al.
2019
Bielinis
✓*
et al.
2019
Song et al. ✓*
✓
2019
Takayama ✓*
et al.
2019
Bielinis
✓*
et al.
2018a, b
Chen et al. ✓*
✓
2018
Lee et al. ✓*
2018
Song et al. ✓*
✓
2018
Chun et al.
✓*
✓*
2017
Guan et al.
✓
2017
Vujcic et al.
✓*
2017
Yu et al. ✓*
✓
2017
Han et al.
✓*
✓
2016
Ochiai et al. ✓*
2015
Takayama ✓*
et al.
2014
Horiuchi ✓*
et al.
2013
Shin et al.
✓*
2012
Lee et al. ✓*
2011
Park et al. ✓*
2011
Morita et al.
✓*
2007
✓
✓*
POMS = Profile of Mood States; STAI = State-Trait Anxiety Inventory; BDI = Beck Depression Inventory;
HDR = Hamilton Depression Rating Scale; AAQ = Anti-Anxiety Questionnaire; EQVAS = EuroQol Visual Ana-
log Scale; MMS = Multiple Mood Scale. * = included in meta-analyses
346
International Journal of Mental Health and Addiction (2022) 20:337–361
Fig. 1 PRISMA flow diagram of the article selection process
Characteristics of Included Studies
Twenty included studies were relatively recent, the oldest one being published in 2007 (Morita
et al.). The majority of the studies were conducted in Asia (n = 18; 86%): ten in Japan
(Furuyashiki et al. 2019; Horiuchi et al. 2013; Lee et al. 2011; Morita et al. 2007; Ochiai
et al. 2015; Park et al. 2011; Song et al. 2018, 2019; Takayama et al. 2014, 2019), four in
Korea (Chun et al. 2017; Lee et al. 2018; Han et al. 2016; Shin et al. 2012), two in Taiwan
(Chen et al. 2018; Yu et al. 2017) and one in China (Guan et al. 2017). Three studies were
conducted in Europe: two in Poland (Bielinis et al. 2018a, b; Bielinis et al. 2019), and one in
Serbia (Vujcic et al. 2017) (Table 2). No studies were identified in Africa, Oceania and South
and North America. Eight studies were non-randomised trials (Table 5), and twelve were
randomised controlled trials (RCT; Table 6). All the non-randomised studies employed a pre-
post design; two studies had a comparator condition. Twelve RCTs included six studies using
crossover (e.g. a forest group walked in a city, while a city group walked in a forest on the
second day; Lee et al. 2011; Park et al. 2011; Song et al. 2018, 2019; Takayama et al. 2014;
Takayama et al. 2019), and one study where groups were categorised by different types of trees
(Guan et al. 2017). Interventions included walking and meditation, and time duration ranged
from 15 min to 9 days. While all studies involved paying attention to the five senses (Table 1
for eligibility criteria), 18 (90%) studies involved walking (Bielinis et al. 2018a, b; Chen et al.
2018; Chun et al. 2017; Furuyashiki et al. 2019; Guan et al. 2017; Han et al. 2016; Horiuchi
et al. 2013; Lee et al. 2011; Lee et al. 2018; Morita et al. 2007; Ochiai et al. 2015; Park et al.
2011; Shin et al. 2012; Song et al. 2019; Takayama et al. 2014, 2019; Vujcic et al. 2017; Yu
et al. 2017), four (20%) involved meditative activities (Furuyashiki et al. 2019; Lee et al. 2018;
Shin et al. 2012; Ochiai et al. 2015) and three (15%) involved recreational activities (Bielinis
et al. 2019; Chen et al. 2018; Han et al. 2016).
A total of 2257 participants (M = 1478, F = 779; age range 18–79 years old) were involved
in these included studies, indicating shinrin-yoku’s wide applicability. Six studies involved

International Journal of Mental Health and Addiction (2022) 20:337–361
347
clinical samples: metabolic syndrome (Lee et al. 2018), chronic stroke (Chun et al. 2017),
psychiatric disorders (Vujcic et al. 2017), chronic diseases (Yu et al. 2017), chronic pain (Han
et al. 2016) and alcoholism (Shin et al. 2012).
Measures
Table 3 presents all included studies organised by the mental health measures. POMS was
frequently used in shinrin-yoku research (n = 14); other measures used in more than one paper
were the State-Trait Anxiety Inventory (STAI; n = 6), and the Beck Depression Inventory
(BDI; n = 3).
Outcomes
Depression was measured using six scales: POMS, BDI, the Depression Anxiety and Stress
Scale (DASS), the EuroQol Visual Analog Scale (EQVAS), the Hamilton Depression Rating
Scale (HDR). Anxiety was also measured using six scales: POMS, STAI, the Anti-Anxiety
Questionnaire (AAQ), DASS, EQVAS and the Multiple Mood Scale (MMS). Anger was
measured using a single scale: POMS.
Meta-analyses
The depression subscales in POMS, DASS21, MMS and BDI were considered for
meta-analysis of depression; EQVAS was excluded as it measures depression and
anxiety together. Chun, Chang and Lee’s study (2017) used HDR and BDI, so
HDR was removed because HDR emphasises physical symptoms (Hamilton 1960).
The anxiety subscales in POMS, STAI and DASS21 were considered for meta-
analysis of anxiety, and the anger subscale in POMS was considered for meta-
analysis of anger (* in Table 3). The anxiety score in STAI from Chun et al.’s study
(2017) was not included as whether the 20 items used were related to state or trait
anxiety was not reported. Likewise, the anxiety score in AAQ (Guan et al. 2017) was
not included as whether this scale has been validated was not reported. For studies
that employed two anxiety subscales, namely POMS and STAI (Chen et al. 2018;
Song et al. 2018, 2019; Yu et al. 2017), POMS was considered as it is more
commonly used. The random effects models were used as the included studies
included diverse populations; thus, heterogeneity was assumed (mean effect sizes =
small, 0.10–0.29; moderate, 0.30–0.49; high, ≧ 0.50; Cohen 1992).
First, data from six RCT studies were analysed (Bielinis et al. 2018a, b; Chun et al. 2017;
Lee et al. 2011; Shin et al. 2012; Takayama et al. 2014, 2019). Song et al.’s RCT studies (2018,
2019) were excluded as these studies only reported post-intervention scores. Lee et al. (2018)
and Guan et al. (2017) were excluded as their RCTs compared different types of forest. Lastly,
Vujcic et al. (2017) was excluded as their RCT did not employ a comparable control group.
Second, 16 studies that reported pre-intervention and post-intervention scores were
analysed (Bielinis et al. 2018a, b, 2019, Chen et al. 2018, Chun et al. 2017, Furuyashiki
et al. 2019, Horiuchi et al. 2013, Lee et al. 2011, 2018, Morita et al. 2007, Ochiai et al. 2015,
Park et al. 2011, Shin et al. 2012, Takayama et al. 2014, 2019, Yu et al. 2017, Vujcic et al.
2017).
348
International Journal of Mental Health and Addiction (2022) 20:337–361
As significant heterogeneity was identified in each symptom, three moderator analyses (i, ii
and iii) and three subgroup analyses (iv, v and vi) were conducted to appraise whether (i)
crossover of the two groups, (ii) participants being Asian, (iii) participants being Japanese, (iv)
the length of the intervention, (v) gender (female-male ratio) and (vi) age accounted for the
variability made difference in the effects. The first moderator (i) crossover was not examined in
the 16 pre-post studies, as it was not applicable. Lastly, publication bias was examined. Table 4
summarises the results of our meta-analysis.
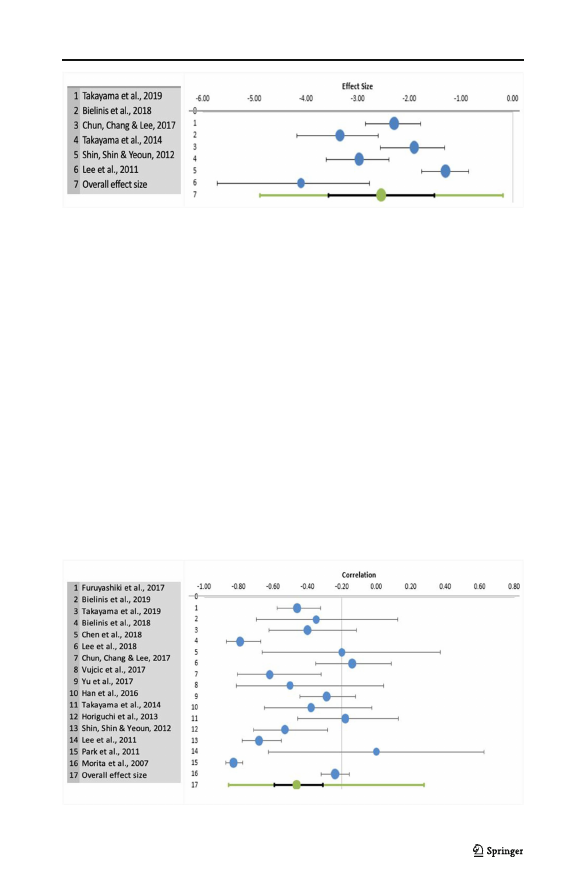
Depression in RCT
The total sample size for RCTs measuring depression was 417 (range 12–47) from six studies.
Figure 2 shows the forest plot for the meta-analysis with depression in RCT. There was a small
mean negative effect size, g = − 2.54, 95% CI(− 3.56, − 1.52), which was significant. Hetero-
geneity of effects was significant (Q = 38.84, p < 0.001) and inconsistency was high (I2 =
87.13%); in all studies, the effect was negative—depression decreased more in the forest
setting compared to the urban setting.
The three moderators—(i) whether group crossover was done or not (p = 0.27), (ii) whether
participants were Asian or not (p = 0.26) and (iii) whether participants were Japanese or not
(p = 0.27)—were not significant predictors. In subgroup analyses, the length of the interven-
tion (iv) was a significant predictor of effect size for depression (slope = 0.04, p = 0.002).
However, the intervention length was not significant (p = 0.11) when one extreme value (Shin
et al. 2012) was removed. The female-male ratio (v) was not a significant (slope = 0.09, p =
0.97), whereas average age (vi) was a significant predictor for depression (slope = 0.04, p =
0.04). Possible evidence of publication bias was identified (Appendix 3).
Table 4 Effect sizes (g) and p values for moderators and subgroups in each variable (depression, anxiety and
anger)
Moderators
Subgroups
Effect size
95% CI
Crossover Asian Japanese Intervention Gender Age
length
Depression RCT (n = 6)
Anxiety
Anger
Pre-Post
(n = 16)
RCT (n = 5)
Pre-Post
(n = 16)
RCT (n = 4)
Pre-Post
(n = 12)
g = − 2.54
(− 3.56,
− 1.52)p
g = − 1.04
(− 1.47,
− 0.60)p
g = − 8.81
(− 21.91, 3.57)
g = − 1.83
(− 3.07,
− 0.58)p
g = − 1.63
(− 3.25,
− 0.01)p
g = − 0.81
(− 1.17,
− 0.45)p
0.27 0.26 0.27
NA 0.12 0.20
0.003 0.007 0.003
NA < 0.001 < 0.001
0.13 0.13 0.13
NA 0.46 0.15
0.002* 0.97 0.04
0.24* 0.03* 0.22
0.19 < 0.001 0.20
0.02* 0.12 0.01*
NA** 0.47 0.06
< 0.001 < 0.001 < 0.001
*After removing an extreme value, the significance of p value changed. Italicised scores are significant values
p < 0.05. **All studies had the same length of intervention. p Publication bias identified
International Journal of Mental Health and Addiction (2022) 20:337–361
349
Fig. 2 Effect size for depression in RCT
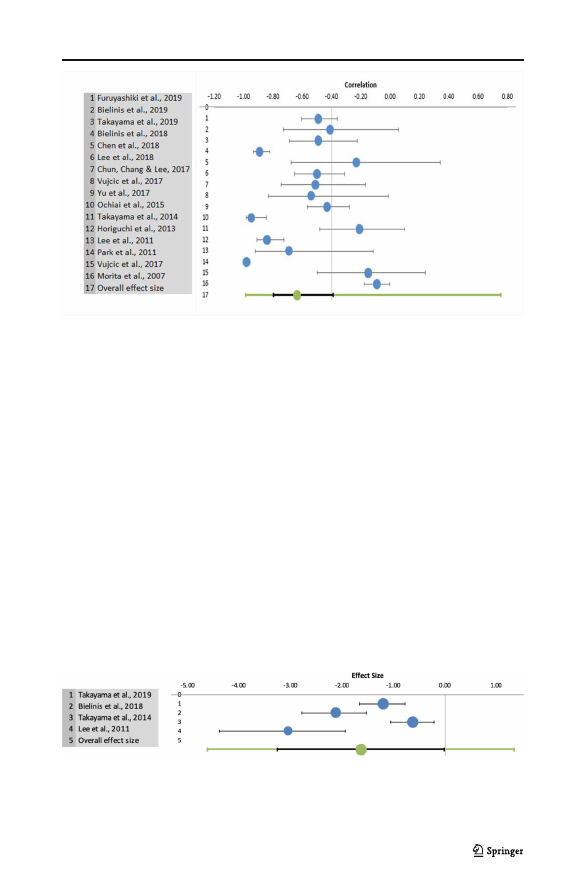
Depression in Studies Reported Pre-Post Scores
The total sample size for pre-post scores measuring depression was 1449 (range 12–498) from
16 studies. Figure 3 shows the forest plot for the meta-analysis with depression in studies that
reported pre-post scores. There was a medium mean negative effect size, g = − 1.04, 95% CI(−
1.47, − 0.60), which was significant. Heterogeneity of effects was significant (Q = 331.57,
p < 0.001) and inconsistency was high (I2 = 95.48%); in all studies, apart from Lee et al.
(2011), the effect was negative—depression decreased from pre-shinrin-yoku to post-shinrin-
yoku.
The two moderators—(ii) whether participants were Asian or not (p = 0.12), and (iii)
whether participants were Japanese or not (p = 0.20)—were not significant predictors. In
subgroup analyses, the length of intervention (iv) was not significant (slope = − 0.02, p =
0.24); however, after removing an extreme value (Park et al. 2011), it became significant and it
was negative; i.e. the longer the intervention, the smaller the effects (slope = − 0.03, p = 0.01).
The female-male ratio (v) was significant (slope = 1.04, p = 0.03); however, after removing an
extreme value (Park et al. 2011), it became non-significant (slope = 0.58, p = 0.15). Lastly,
average age (vi) was non-significant (slope = 0.01, p = 0.22). Possible evidence of publication
bias was identified (Appendix 4).
Fig. 3 Effect size for depression in studies reported pre-post scores
350
International Journal of Mental Health and Addiction (2022) 20:337–361
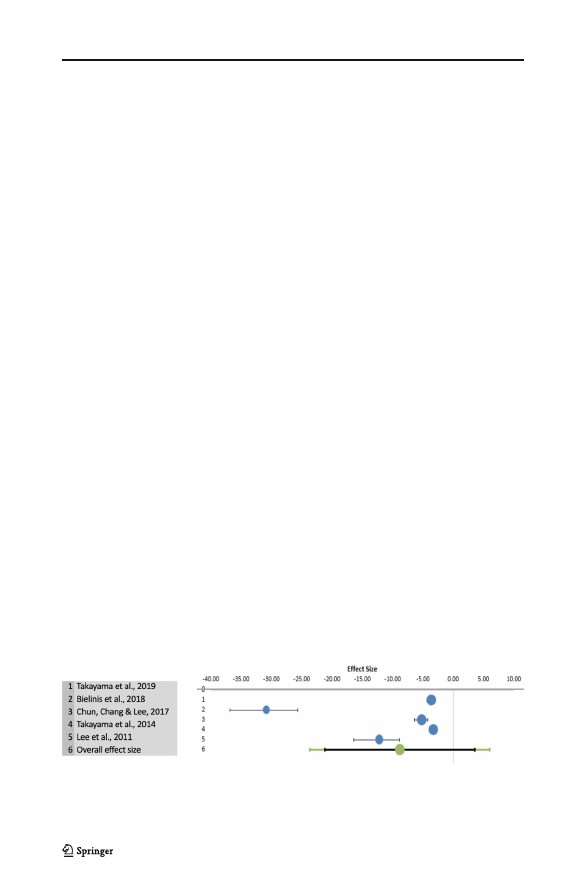
Anxiety in RCT
The total sample size for studies measuring anxiety was 327 (range 12–46) from five studies.
Figure 4 shows the forest plot for the meta-analysis with anxiety. There was a large mean
negative effect size, g = − 8.81, 95% CI(− 21.91, 3.57), which was not significant. Variability
across samples was significant (Q = 125.03, p < 0.001) and high (I2 = 96.80%).
All moderators—crossover (p = 0.003), Asian (p = 0.007) and Japanese (p = 0.003)—were
significant predictors of effect size for anxiety. The length of the intervention (iv) was not a
significant predictor (slope = 0.35, p = 0.19). Female-male ratio (v) was a significant predictor;
i.e. the effects were smaller when there were fewer female participants (slope = − 30.84,
p < 0.001), whereas average age (vi) was not a significant predictor (slope = 0.13, p = 0.20).
Possible evidence of publication bias was not identified (Appendix 5).
Anxiety in Studies Reported Pre-Post Scores
The total sample size for pre-post scores measuring anxiety was 1371 (range 12–498) from 16
studies. Figure 5 shows the forest plot for the meta-analysis with anxiety in studies that
reported pre-post scores. There was a large mean negative effect size, r = − 1.83, 95% CI(−
3.07, − 0.58), which was significant. Heterogeneity of effects was significant (Q = 611.89,
p < 0.001) and inconsistency was high (I2 = 97.55%); in all studies, anxiety decreased from
pre-shinrin-yoku to post-shinrin-yoku.
The two moderators—(ii) whether participants were Asian or not (p = 0.88), and (iii)
whether participants were Japanese or not (p = 0.75)—were not significant predictors. In
subgroup analyses, (iv) the length of the intervention was significant; i.e. the longer the
intervention, the more effects observed (slope = 0.13, p = 0.02); however, after removing one
extreme value (Park et al. 2011), it was not significant (slope = 0.05, p = 0.24). The female-
male ratio (v) was not significant (slope = 1.26, p = 0.12). Lastly, the average age (vi) was a
significant moderator (slope = 0.04, p = 0.01); however, after removing an extreme value (Park
et al. 2011), it became non-significant (slope = 0.01, p = 0.52). Possible evidence of publica-
tion bias was identified (Appendix 6).
Anger in RCT
The total sample size for studies measuring anger was 268 (range 12–46) from four studies.
Figure 6 shows the forest plot for the meta-analysis with anger. There was a medium mean
Fig. 4 Effect size for anxiety in RCT
International Journal of Mental Health and Addiction (2022) 20:337–361
351
Fig. 5 Effect size for anxiety in studies reported pre-post scores
negative effect size, g = − 1.63, 95% CI(− 13.25, − 0.01), which was significant. Variability
across samples was significant (Q = 25.52, p < 0.001) and high (I2 = 88.25%).
For anger, all the three moderators—crossover (p = 0.13), Asian (p = 0.13) and Japanese
(p = 0.13)—were not significant predictors. Likewise, the intervention length (data unidenti-
fied), female-male ratio (slope = − 1.61, p = 0.47) and average age (slope = − 3.40, p = 0.06)
were not significant. Possible evidence of publication bias was identified (Appendix 7).
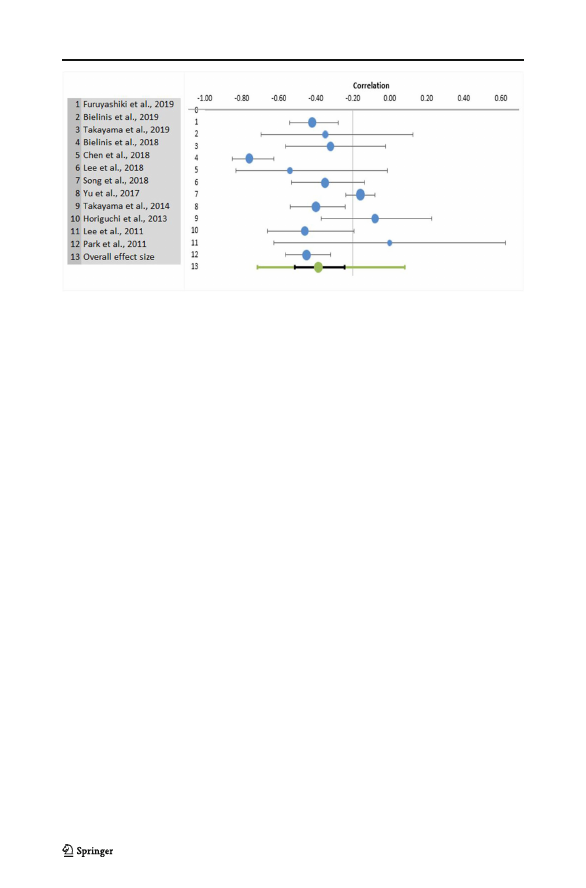
Anger in Studies Reported Pre-Post Scores
The total sample size for pre-post scores measuring anger was 1365 (range 12–498) from 12 studies.
Figure 7 shows the forest plot for the meta-analysis with anger in studies that reported pre-post
scores. There was a medium mean negative effect size, g = − 0.81, 95% CI(− 1.17, − 0.45), which
was significant. Heterogeneity of effects was significant (Q = 153.52, p < 0.001) and inconsistency
was high (I2 = 92.83%); in all studies, anger decreased from pre-shinrin-yoku to post-shinrin-yoku.
The two moderators—(ii) whether participants were Asian or not (p = 0.46), and (iii)
whether participants were Japanese or not (p = 0.15)—were not significant predictors. In
subgroup analyses, all subgroups were significant: the length of the intervention (iv) slope =
− 0.13, p < 0.001; female-male ratio (v) slope = − 0.65, p < 0.001, and average age (vi) slope =
− 0.01, p < 0.001. Possible evidence of publication bias was identified (Appendix 8).
Fig. 6 Effect size for anger in RCT
352
International Journal of Mental Health and Addiction (2022) 20:337–361
Fig. 7 Effect size for anger in studies reported pre-post scores
Risk of Bias
The risk of bias in the non-randomised studies was deemed to be medium for all eight studies
(Bielinis et al. 2019; Chen et al. 2018; Furuyashiki et al. 2019; Han et al. 2016; Horiuchi et al.
2013; Morita et al. 2007; Ochiai et al. 2015; Yu et al. 2017). All of these studies assessed the
mental health outcomes before and after shinrin-yoku (for non-clinical samples, participation
eligibility of no mental health disorder was reported). None of these eight studies commented
on the representativeness of the cohort or conducted follow-up assessments (Table 5).
In the randomised controlled trials, the risk of bias was deemed high to medium: all the studies
scored from two (Bielinis et al. 2018a, b) to six (Shin et al. 2012). For the studies that employed
crossover (Park et al. 2011; Song et al. 2019; Takayama et al. 2014, 2019), blinding administration
and participants were both graded as ‘not applicable (NA)’ as it was impossible for participants to be
unaware of the condition they were assigned to at each time. All studies reported the number of
participants allocated to different groups, and inclusion criteria apart from Song et al. (2019). The
baseline comparability of different groups was reported in seven studies (Chun et al. 2017; Guan
et al. 2017; Lee et al. 2011, 2018; Shin et al. 2012; Takayama et al. 2014, 2019), and achieved in
seven studies (Chun et al. 2017; Guan et al. 2017; Lee et al. 2011, 2018; Shin et al. 2012; Takayama
et al. 2014; Vujcic et al. 2017): Vujcic et al. (2017) did not present demographic details; however,
they noted that the gender and diagnosis distribution were equal. Unsurprisingly, given the type of
intervention, no study maintained allocation concealment and blinding of assessors, administration
and participants; hence, the blinding procedure was poor (Table 6).
Discussion
This systematic review and meta-analysis examined the quality and extent of evidence
reported in studies investigating the effects of shinrin-yoku on mental health. Twenty studies
(eight non-randomised, and twelve randomised controlled trials), involving 2257 participants,
satisfied all of the eligibility criteria for in-depth review and assessment. Shinrin-yoku was
deemed to have a greater effect on anxiety, than depression and anger, and the effects on
anxiety could be predicted by many of the moderators examined, including the gender and
International Journal of Mental Health and Addiction (2022) 20:337–361
353
International Journal of Mental Health and Addiction (2022) 20:337–361
354
355
International Journal of Mental Health and Addiction (2022) 20:337–361

356
International Journal of Mental Health and Addiction (2022) 20:337–361
Japanese or Asian participants (greater proportions of females, Japanese or Asian participants
were associated with larger effects). Potential publication bias was identified in all analyses
apart from RCTs on anxiety. While some studies demonstrated rigorous design and reporting,
our conclusions are tempered by a number of weaknesses concerning study design and
outcomes. Accordingly, in this discussion, we elucidate a number of areas of improvement.
Shinrin-yoku was reported effective for depression, anxiety, stress and anger in both clinical
and non-clinical samples, especially for anxiety. The results reported in the selected studies
were in line with relevant theories: spending time in nature increased restoration (Bielinis et al.
2019) aligning with Attention Restoration Theory (Kaplan and Kaplan 1989). Stress was
reduced through shinrin-yoku (Vujcic et al. 2017; Morita et al. 2007), supporting Stress
Reduction Theory (Ulrich et al. 1991). The role of nature in affect regulation is often overlooked
(Korpela et al. 2018), and although not explicitly explored, findings accord with the three
emotion regulatory systems model (threat, drive, and soothing; Richardson et al. 2016); being in
nature may activate our soothing system, endorsing compassion, safety and connection,
protecting our mental health. Psychological constructs relevant to the soothing system such
as self-compassion and psychological safety need to be examined in shinrin-yoku research.
Further, although likely to activate the pathways to nature connection (Lumber et al. 2017),
none of the studies explored the psychological construct of nature connectedness—oneness
with nature (Nisbet et al. 2009)—which is positively associated with psychological well-being
(Pritchard et al. 2019). Future shinrin-yoku research should also explore nature connectedness.
Although all included studies demonstrated promising results, the risk of bias was deemed
medium to high, and potential publication bias was identified in almost all analyses. This may
explain why benefits were greater for Japanese and Asian participants: people in a culture that
accords with nature’s healing effects may receive greater benefits of shinrin-yoku (e.g. Shintoism,
perceptions of nature differ cross-culturally; Gierlach et al. 2010). Furthermore, none of the RCTs
compared shinrin-yoku with other major therapeutic approaches such as CBT (while there was a
study that combined CBT and nature; Kim et al. 2009): shinrin-yoku was only compared with
spending time in urban settings (Vujcic et al. 2017 compared with art therapy, not a major approach).
Given that being in an urban setting has negative health effects (Lederbogen et al. 2011; Marques
and Lima 2011), shinrin-yoku should be compared with other major therapeutic approaches. Indeed,
in our RCT meta-analyses, all control/urban groups, apart from depression score in Chun, Chang
and Lee’s study (2017), reported increases in mean scores. These points suggest the need for shinrin-
yoku research in Oceania, Africa and North and South America, and the need to compare shinrin-
yoku with other major approaches. Moreover, shinrin-yoku’s effects were particularly salient for
anxiety, which is the most common mental health problem in the world (Ritchie and Roser 2018),
again suggesting more shinrin-yoku research is needed.
Other limitations in shinrin-yoku research included a lack of follow-up assessments and
consideration for sample representativeness. A lack of follow-up assessments can compromise
the validity of clinical research because whether the effects of shinrin-yoku can last or not
remains uncertain (Dettori 2011). The representativeness of the sample was not addressed;
therefore, whether the study recruited people who were interested in, and positively interpreted/
reported the effects of shinrin-yoku or not, was not clarified. In the RCTs, randomisation and
blinding were not addressed. This may be again related to participants’ expectations (Antonelli
et al. 2019): revealing the allocation of the group, participants who were interested in shinrin-
yoku might have become more susceptible to placebo effects. In addition, many RCTs used a
crossover design with no interval (the groups were swapped on the next day), which may
violate the accuracy of the results: the impacts of the first intervention need to be washed out

International Journal of Mental Health and Addiction (2022) 20:337–361
357
before swapping the groups (Enck and Zipfel 2019). Furthermore, failing to blind the re-
searchers can lead to placebo effects in participants; this may be particularly important when
many of the reviewed studies included a prominent shinrin-yoku figure (e.g. Miyazaki, Lee).
Finally, the included RCTs did not conduct intention-to-treat analysis and did not clarify
whether other outcomes were measured or not. Similar to a previous systematic review
(Kamioka et al. 2012), lack of these research items needs to be addressed in the future studies.
Lastly, though we defined that nature-based practice must include integration with nature
engaging with five sensory experience to be recognised as shinrin-yoku (Table 1), shinrin-
yoku practice included diverse forms: most commonly walking, meditation and recreational
activities such as handcrafts. While this indicates high applicability of shinrin-yoku, it could
also leave shinrin-yoku practice rather unguided. This may resemble mindfulness, which can
be practiced in many ways (Williams and Penman 2011), but its flexibility may make
practitioners feel that they were just sitting or sleeping (Bojic and Becerra 2017) and lead to
biased reporting (Schumer et al. 2018). As with other alternative approaches, shinrin-yoku can
benefit from more guidance in practice, to be more accepted as a reliable clinical approach.
Accredited training packages are emerging (e.g. the European Forest Therapy Institute 2019).
While this article offers useful insights, limitations need to be noted. Firstly, unpublished
studies, qualitative studies (e.g. Sonntag-Öström et al. 2015) or studies not published in
English language were excluded (Appendix 9 for articles in Japanese satisfying the other
criteria). Also, some studies examined many variables (Bielinis et al. 2018a, b, 2019;
Takayama et al. 2014, 2019); however, the multiple comparisons problem was not addressed.
These could exaggerate the effects of shinrin-yoku. Lastly, the included studies were conduct-
ed only in two continents. Considering the serious nature of mental health globally, and
different views on nature, research in other continents should be conducted.
Conclusion
The twenty studies included reported that shinrin-yoku is effective for mental health, partic-
ularly anxiety. Shinrin-yoku can be practiced in 15 min to 9 days, and reduce negative mental
health symptoms. While promising results were reported, medium-high risk of bias and
publication bias were identified. Some of the key constructs related to mental health (e.g.
self-compassion, isolation, nature connectedness) have not been explored in shinrin-yoku
research and mechanisms of benefits have not been determined. Additionally, the duration
of benefits and how they compare with other established therapeutic approaches need to be
examined for shinrin-yoku to be accepted as mainstream intervention.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict of interest.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which
permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and
indicate if changes were made. The images or other third party material in this article are included in the article's
Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included
in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or

358
International Journal of Mental Health and Addiction (2022) 20:337–361
exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy
of this licence, visit http://creativecommons.org/licenses/by/4.0/.
References
Antonelli, M., Barbieri, G., & Donelli, D. (2019). Effects of forest bathing (shinrin-yoku) on levels of cortisol as
a stress biomarker: a systematic review and meta-analysis. International Journal of Biometeorology, 63,
1117–1134. https://doi.org/10.1007/s00484-019-01717-x.
Bielinis, E., Omelan, A., Boiko, S., & Bielinis, L. (2018a). The restorative effect of staying in a broad-leaved
forest on healthy young adults in winter and spring. Baltic Forestry, 24(2), 218–227 Retrieved from
https://www.balticforestry.mi.lt/ojs/index.php/BF/article/view/204.
Bielinis, E., Takayama, N., Boiko, S., Omelan, A., & Bielinis, L. (2018b). The effect of winter forest bathing on
psychological relaxation of young Polish adults. Urban Forestry & Urban Greening, 29, 276–283.
https://doi.org/10.1016/J.UFUG.2017.12.006.
Bielinis, E., Bielinis, L., Krupińska-Szeluga, S., Łukowski, A., Takayama, N., Bielinis, E., et al. (2019). The
effects of a short forest recreation program on physiological and psychological relaxation in young Polish
adults. Forests, 10(1), 34. https://doi.org/10.3390/f10010034.
Bojic, S., & Becerra, R. (2017). Mindfulness-based treatment for bipolar disorder: a systematic review of the
literature. Europe’s Journal of Psychology, 13(3), 573–598. https://doi.org/10.5964/ejop.v13i3.1138.
Boland, A., Cherry, M. G., & Dickson, R. (2013). Doing a systematic review: a student’s guide. London: Sage.
Bratman, G. N., Hamilton, J. P., Hahn, K. S., Daily, G. C., & Gross, J. J. (2015). Nature experience reduces
rumination and subgenual prefrontal cortex activation. Proceedings of the National Academy of Sciences of
the United States of America, 112(28), 8567–8572. https://doi.org/10.1073/pnas.1510459112.
Brown, T., Pilkington, G., Bagust, A., Boland, A., Oyee, J., Tudur-Smith, C., Blundell, M., Lai, M., Martin
Saborido, C., Greenhalgh, J., Dundar, Y., & Dickson, R. (2013). Clinical effectiveness and cost-effectiveness
of first-line chemotherapy for adult patients with locally advanced or metastatic non-small cell lung cancer: a
systematic review and economic evaluation. Health Technology Assessment, 17(31), 1–278. https://doi.
org/10.3310/hta17310.
Callahan J. L. (2010). Constructing a Manuscript: Distinguishing Integrative Literature Reviews and Conceptual
and Theory Articles. Human Resource Development Review, 9(3), 300–304. https://doi.org/10.1177
/1534484310371492.
Chen, H.-T., Yu, C.-P., Lee, H.-Y., Chen, H.-T., Yu, C.-P., & Lee, H.-Y. (2018). The effects of forest bathing on stress
recovery: evidence from middle-aged females of Taiwan. Forests, 9(7), 403. https://doi.org/10.3390/f9070403.
Chun, M. H., Chang, M. C., & Lee, S.-J. (2017). The effects of forest therapy on depression and anxiety in
patients with chronic stroke. International Journal of Neuroscience, 127(3), 199–203. https://doi.
org/10.3109/00207454.2016.1170015.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159.
Department of Health. (2011). No health without mental health A cross-government mental health outcomes
strategy for people of all ages. London: Retrieved from www.dh.gov.uk/mentalhealthstrategy.
Dettori, J. (2011). Loss to follow-up. Evidence-Based Spine-Care Journal 2(01), 7–10. https://doi.org/10.1055/s-
0030-1267080.
Enck, P., & Zipfel, S. (2019). Placebo effects in psychotherapy: a framework. Frontiers in Psychiatry, 10.
https://doi.org/10.3389/fpsyt.2019.00456.
European Forest Therapy Institute. (2019). Become a guide. Retrieved from https://www.
europeanforesttherapyinstitute.com/become-a-guide/
Farmer, P., & Dyer, J. (2016). The five year forward view for mental health. London: The Mental Health Taskforce.
Farrow, M. R., & Washburn K. (2019). A Review of Field Experiments on the Effect of Forest Bathing on
Anxiety and Heart Rate Variability. Global Advances in Health and Medicine, 8(3), 216495611984865.
https://doi.org/10.1177/2164956119848654.
Forest Therapy Society (2005). What is Forest Therapy? [Shinrin Serapi- toha] Retrieved from https://www.fo-
society.jp/therapy/index.html
Furuyashiki, A., Tabuchi, K., Norikoshi, K., Kobayashi, T., & Oriyama, S. (2019). A comparative study of the
physiological and psychological effects of forest bathing (Shinrin-yoku) on working age people with and
without depressive tendencies. Environmental Health and Preventive Medicine, 24(46), 46. https://doi.
org/10.1186/s12199-019-0800-1.
Gierlach, E., Belsher, B. E., & Beutler, L. E. (2010). Cross-cultural differences in risk perceptions of disasters.
Risk Analysis, 30(10), 1539–1549. https://doi.org/10.1111/j.1539-6924.2010.01451.x.

International Journal of Mental Health and Addiction (2022) 20:337–361
359
Gilbert, P. (2014). The origins and nature of compassion focused therapy. British Journal of Clinical Psychology,
53(1), 6–41. https://doi.org/10.1111/bjc.12043.
Gross, J. J. (2013). Emotion regulation: taking stock and moving forward. Emotion, 13(3), 359–365. https://doi.
org/10.1037/a0032135.
Guan, H., Wei, H., He, X., Ren, Z., & An, B. (2017). The tree-species-specific effect of forest bathing on
perceived anxiety alleviation of young-adults in urban forests. Annals of Forest Research, 0(0), 327–341.
https://doi.org/10.15287/afr.2017.897
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery, and Psychiatry, 23, 56–62.
Han, J.-W., Choi, H., Jeon, Y.-H., Yoon, C.-H., Woo, J.-M., & Kim, W. (2016). The effects of forest therapy on
coping with chronic widespread pain: physiological and psychological differences between participants in a
forest therapy program and a control group. International Journal of Environmental Research and Public
Health, 13(3). https://doi.org/10.3390/ijerph13030255.
Hansen, M. M., Jones, R., & Tocchini, K. (2017). Shinrin-Yoku (forest bathing) and nature therapy: a state-of-
the-art review. International Journal of Environmental Research and Public Health, 14(8). https://doi.
org/10.3390/ijerph14080851.
Hewlett, E. (2014). Making mental health count. Focus on Mental Health. https://doi.org/10.1787
/9789264124523-en.
Horiuchi, M., Endo, J., Akatsuka, S., Uno, T., Hasegawa, T., & Seko, Y. (2013). Influence of forest walking on
blood pressure, profile of mood states and stress markers from the viewpoint of aging. Journal of Aging and
Gerontology. https://doi.org/10.12974/2309-6128.2013.01.01.2.
Hunter, M. R., Gillespie, B. W., & Chen, S. Y.-P. (2019). Urban nature experiences reduce stress in the context of
daily life based on salivary biomarkers. Frontiers in Psychology, 10, 722. https://doi.org/10.3389
/fpsyg.2019.00722.
James, P., Hart, J. E., Banay, R. F., & Laden, F. (2016). Exposure to greenness and mortality in a nationwide
prospective cohort study of women. Environmental Health Perspectives, 124(9), 1344–1352. https://doi.
org/10.1289/ehp.1510363.
Kamioka, H., Tsutani, K., Mutoh, Y., Honda, T., Shiozawa, N., Park, S., et al. (2012). A systematic review of
randomized controlled trials on curative and health enhancement effects of forest therapy. Psychology
Research and Behavior Management, 5, 85. https://doi.org/10.2147/PRBM.S32402.
Kaplan, R., & Kaplan, S. (1989). The experience of nature :a psychological perspective. Cambridge University Press.
Kim, W., Lim, S. K., Chung, E. J., & Woo, J. M. (2009). The effect of cognitive behavior therapy-based
psychotherapy applied in a forest environment on physiological changes and remission of major depressive
disorder. Psychiatry Investigation, 6(4), 245–254. https://doi.org/10.4306/pi.2009.6.4.245.
Klassen, T. P., Jadad, A. R., & Moher, D. (1998). Guides for reading and interpreting systematic reviews: I.
getting started. Archives of Pediatrics & Adolescent Medicine, 152(7), 700–704. https://doi.org/10.1001
/ARCHPEDI.152.7.700.
Korpela, K., Nummi, T., Lipiäinen, L., De Bloom, J., Sianoja, M., Pasanen, T., & Kinnunen, U. (2018). Nature
exposure predicts well-being trajectory groups among employees across two years. Journal of
Environmental Psychology, 52, 81–91. https://doi.org/10.1016/J.JENVP.2017.06.002.
Lederbogen, F., Kirsch, P., Haddad, L., Streit, F., Tostet, H., et al. (2011). City living and urban upbringing affect
neural social stress processing in humans. Nature, 474, 498–501. https://doi.org/10.1038/nature10190.
Lee, J., Park, B.-J., Tsunetsugu, Y., Ohira, T., Kagawa, T., & Miyazaki, Y. (2011). Effect of forest bathing on
physiological and psychological responses in young Japanese male subjects. Public Health, 125(2), 93–100.
https://doi.org/10.1016/j.puhe.2010.09.005.
Lee, K. J., Hur, J., Yang, K.-S., Lee, M.-K., & Lee, S.-J. (2018). Acute biophysical responses and psychological
effects of different types of forests in patients with metabolic syndrome. Environment and Behavior, 50(3),
298–323. https://doi.org/10.1177/0013916517700957.
Lee, J., Park, B.-J., Tsunetsugu, Y., Ohira, T., Kagawa, T., & Miyazaki, Y. (2019). Corrigendum to “Effect of forest
bathing on physiological and psychological responses in young Japanese male subjects” [Public Health 125 (2)
(February 2011), 93–100]. Public Health, 169, 201. https://doi.org/10.1016/j.puhe.2019.03.002.
Li, Q. (2010). Effect of forest bathing trips on human immune function. Environmental Health and Preventive
Medicine, 15(1), 9–17. https://doi.org/10.1007/s12199-008-0068-3.
Lumber, R., Richardson, M., & Sheffield, D. (2017). Beyond knowing nature: contact, emotion, compassion,
meaning, and beauty are pathways to nature connection. PLoS One, 12(5), e0177186. https://doi.
org/10.1371/journal.pone.0177186.
Marques, S., & Lima, M. L. (2011). Living in grey areas: industrial activity and psychological health. Journal of
Environmental Psychology, 31(4), 314–322. https://doi.org/10.1016/j.jenvp.2010.12.002.
Marquez, P. V, & Saxena, S. (2016). Making mental health a global priority. Cerebrum: The Dana Forum on
Brain Science, 2016. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/28058091.
360
International Journal of Mental Health and Addiction (2022) 20:337–361
Martin, L., White, M. P., Hunt, A., Richardson, M., Pahl, S., & Burt, J. (2020). Nature contact, nature
connectedness and associations with health, wellbeing and pro-environmental behaviours. Journal of
Environmental Psychology, 68, 101389. https://doi.org/10.1016/j.jenvp.2020.101389.
Mental Health Foundation. (2016). Fundamental facts about mental health 2016. London: Author.
Ministry of Health, Labour and Welfare. (2004). Revolutional vision for mental health medical welfare
[Seishinhokeniryoufukushi no bijon]. Tokyo. Retrieved from https://www.mhlw.go.jp/kokoro/nation/vision.html
Miyazaki, Y. (2018). Shinrin-yoku: the Japanese way of forest bathing for health and relaxation.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Group, T. P. (2009). Preferred reporting items for
systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097.
https://doi.org/10.1371/journal.pmed.1000097.
Morita, E., Fukuda, S., Nagano, J., Hamajima, N., Yamamoto, H., Iwai, Y., Nakashima, T., Ohira, H., &
Shirakawa, T. (2007). Psychological effects of forest environments on healthy adults: Shinrin-yoku
(forest-air bathing, walking) as a possible method of stress reduction. Public Health, 121(1), 54–63.
https://doi.org/10.1016/j.puhe.2006.05.024.
Nisbet, E. K., Zelenski, J. M., & Murphy, S. A. (2009). The nature relatedness scale. Environment and Behavior,
41(5), 715–740. https://doi.org/10.1177/0013916508318748.
Ochiai, H., Ikei, H., Song, C., Kobayashi, M., Miura, T., Kagawa, T., Li, Q., Kumeda, S., Imai, M., & Miyazaki,
Y. (2015). Physiological and psychological effects of a forest therapy program on middle-aged females.
International Journal of Environmental Research and Public Health, 12(12), 15222–15232. https://doi.
org/10.3390/ijerph121214984.
Park, B.-J., Furuya, K., Kasetani, T., Takayama, N., Kagawa, T., & Miyazaki, Y. (2011). Relationship between
psychological responses and physical environments in forest settings. Landscape and Urban Planning,
102(1), 24–32. https://doi.org/10.1016/J.LANDURBPLAN.2011.03.005.
Park, B.-J., Tsunetsugu, Y., Lee, J., Kagawa, T., & Miyazaki, Y. (2012). Effect of the forest environment on
physiological relaxation—the results of field tests at 35 sites throughout Japan. In Q. Li (Ed.), Forest
Medicine (pp. 55–65). New York: Nova Science Publishers.
Patel, V. (2007). Mental health in low- and middle-income countries. British Medical Bulletin, 81–82(1), 81–96.
https://doi.org/10.1093/bmb/ldm010.
Payne, M., & Delphinus, E. (2019). The most natural of natural therapies: a review of the health benefits derived
from Shinrin-Yoku (forest bathing). Advances in Integrative Medicine, 6, S109–S110. https://doi.
org/10.1016/j.aimed.2019.03.316.
Piff, P. K., Dietze, P., Feinberg, M., Stancato, D. M., & Keltner, D. (2015). Awe, the small self, and prosocial
behavior. https://doi.org/10.1037/pspi0000018.
Pritchard, A., Richardson, M., Sheffield, D., & McEwan, K. (2019). The relationship between nature connect-
edness and Eudaimonic well-being: a meta-analysis. Journal of Happiness Studies, 21, 1–23. https://doi.
org/10.1007/s10902-019-00118-6.
Richardson, M., McEwan, K., Maratos, F., & Sheffield, D. (2016). Joy and calm: how an evolutionary functional
model of affect regulation informs positive emotions in nature. Evolutionary Psychological Science, 2(4),
308–320. https://doi.org/10.1007/s40806-016-0065-5.
Ritchie, H. & Roser, M. (2018). Mental health. Retrieved from https://ourworldindata.org/mental-health.
Rojon, C., McDowall, A., & Saunders, M. N. K. (2011). On the experience of conducting a systematic review in
industrial, work, and organizational psychology. Journal of Personnel Psychology, 10(3), 133–138.
https://doi.org/10.1027/1866-5888/a000041.
Sackett, D., Richardson, W. S., Rosenburg, W., & Haynes, R. B. (1997). How to practice and teach evidence
based medicine (2nd ed.). London: Churchill Livingstone.
Schumer, M. C., Lindsay, E. K., & Creswell, J. D. (2018). Brief mindfulness training for negative affectivity: a
systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 86(7), 569–583.
https://doi.org/10.1037/ccp0000324.
Shanahan, D. F., Bush, R., Gaston, K. J., Lin, B. B., Dean, J., Barber, E., & Fuller, R. A. (2016). Health benefits
from nature experiences depend on dose. Scientific Reports, 6(1), 28551. https://doi.org/10.1038/srep28551.
Shin, W. S., Shin, C. S., & Yeoun, P. S. (2012). The influence of forest therapy camp on depression in alcoholics.
Environmental Health and Preventive Medicine, 17(1), 73–76. https://doi.org/10.1007/s12199-011-0215-0.
Song, C., Ikei, H., Park, B.-J., Lee, J., Kagawa, T., & Miyazaki, Y. (2018). Psychological benefits of walking
through forest areas. International Journal of Environmental Research and Public Health, 15(12), 2804.
https://doi.org/10.3390/ijerph15122804.
Song, C., Ikei, H., Kagawa, T., & Miyazaki, Y. (2019). Effects of walking in a forest on young women.
International Journal of Environmental Research and Public Health, 16(2). https://doi.org/10.3390
/ijerph16020229.
Sonntag-Öström, E., Stenlund, T., Nordin, M., Lundell, Y., Ahlgren, C., Fjellman-Wiklund, A., Järvholm, L. S.,
& Dolling, A. (2015). ‘Nature’s effect on my mind’ – patient’s qualitative experiences of a forest–based
International Journal of Mental Health and Addiction (2022) 20:337–361
361
rehabilitation programme. Urban Forestry and Urban Greening, 14, 607–614. https://doi.org/10.1016/j.
ufug.2015.06.002.
Takayama, N., Korpela, K., Lee, J., Morikawa, T., Tsunetsugu, Y., Park, B.-J., Li, Q., Tyrväinen, L., Miyazaki,
Y., & Kagawa, T. (2014). Emotional, restorative and vitalizing effects of forest and urban environments at
four sites in Japan. International Journal of Environmental Research and Public Health, 11(7), 7207–7230.
https://doi.org/10.3390/IJERPH110707207.
Takayama, N., Morikawa, T., Bielinis, E., Takayama, N., Morikawa, T., & Bielinis, E. (2019). Relation between
psychological restorativeness and lifestyle, quality of life, resilience, and stress-coping in forest settings. International
Journal of Environmental Research and Public Health, 16(8), 1456. https://doi.org/10.3390/ijerph16081456.
Ulrich, R. S., Simons, R. F., Losito, B. D., Fiorito, E., Miles, M. A., & Zelson, M. (1991). Stress recovery during
exposure to natural and urban environments. Journal of Environmental Psychology, 11(3), 201–230.
https://doi.org/10.1016/S0272-4944(05)80184-7.
Van Rhee, H. J., Suurmond, R., & Hak, T. (2015). User manual for meta-essentials: workbooks for meta-analysis
(version 1.0). Rotterdam: Erasmus Research Institute of Management http://www.erim.eur.nl/research-
support/meta-essentials.
Vujcic, M., Tomicevic-Dubljevic, J., Grbic, M., Lecic-Tosevski, D., Vukovic, O., & Toskovic, O. (2017). Nature
based solution for improving mental health and well-being in urban areas. Environmental Research, 158,
385–392. https://doi.org/10.1016/j.envres.2017.06.030.
Walsh, L., Wolk, C., Haimes, E., Jensen-Doss, A., & Beidas, R. (2018). The relationship between anger and
anxiety symptoms in youth with anxiety disorders. Journal of Child and Adolescent Counseling, 4(2), 117–
133. https://doi.org/10.1080/23727810.2017.1381930.
Wells, G. A., Shea, B., O'Connell, D., Peterson, J., Welch, V., Losos, M., & Tugwell, P. (2000). The Newcastle-
Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Retrieved, 15
June 2017, from http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
Williams, F. (2016). This is your brain on nature. Retrieved July 13, 2019, from https://www.nationalgeographic.
com/magazine/2016/01/call-to-wild/
Williams, M., & Penman, D. (2011). Mindfulness: a practical guide to finding peace in a frantic world. London: Piatkus.
World Health Organization. (2002). Nations for mental health final report. Geneva: Retrieved from https://www.
who.int/mental_health/media/en/400.pdf.
World Health Organization. (2013). Mental health action plan 2013–2020. World Health Organization. Retrieved
from https://www.who.int/mental_health/publications/action_plan/en/
Yu, C.-P., Lin, C.-M., Tsai, M.-J., Tsai, Y.-C., & Chen, C.-Y. (2017). Effects of short forest bathing program on
autonomic nervous system activity and mood states in middle-aged and elderly individuals. International
Journal of Environmental Research and Public Health, 14(8), 897. https://doi.org/10.3390/ijerph14080897.
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.