
The Open Journal of Occupational Therapy
Volume 10
Issue 1 Winter 2022
Article 7
January 2022
Ecospirituality in Forensic Mental Health: A Preliminary Outcome
Study
Clark Patrick Heard
The University of Western Ontario - Canada, clark.heard@sjhc.london.on.ca
Jared Scott
The University of Western Ontario - Canada, jared.scott@sjhc.london.on.ca
Stephen Yeo
Martin Luther University College, Laurier University - Canada, stephen.yeo@sjhc.london.on.ca
Follow this and additional works at: https://scholarworks.wmich.edu/ojot
Part of the Occupational Therapy Commons, Other Mental and Social Health Commons, and the Other
Rehabilitation and Therapy Commons
Recommended Citation
Heard, C. P., Scott, J., & Yeo, S. (2022). Ecospirituality in Forensic Mental Health: A Preliminary Outcome
Study. The Open Journal of Occupational Therapy, 10(1), 1-15. https://doi.org/10.15453/2168-6408.1708
This document has been accepted for inclusion in The Open Journal of Occupational Therapy by the editors. Free,
open access is provided by ScholarWorks at WMU. For more information, please contact wmu-
scholarworks@wmich.edu.
Ecospirituality in Forensic Mental Health: A Preliminary Outcome Study
Abstract
Background: In this study, the personal experience of spirituality in nature (the concept of ecospirituality)
was supported by occupational therapy and spiritual care staff enabling a community-based group for
persons affiliated with a forensic mental health system in Ontario, Canada. Spirituality is a key, though
debated, tenet in occupational therapy practice. At the same time, immersive participation in nature has
been linked to positive health outcomes.
Methods: A qualitative method consistent with Interpretative Phenomenological Analysis was employed.
Data was collected via the completion of semi-structured interviews (n = 9). Collected data was
transcribed verbatim and then coded for themes by multiple coders. Several methods were employed to
support trustworthiness.
Results: Results identified that participation in the ecospirituality group enabled the participants to feel an
enhanced connection with nature and an opportunity for unguarded reflection and relaxation. The
participants described a regenerative and restorative experience, including a sense of peace and
connection with the personally sacred. Enhanced resiliency and meaningful connection with others also
were identified.
Conclusion: Recommendations related to outcomes are identified. These include a focus on enhanced
access to natural environments for individuals involved in mental health systems. Just as importantly, the
opportunity for personal agency and autonomy in those settings appears indicated.
Comments
The authors declare that they have no competing financial, professional, or personal interest that might
have influenced the performance or presentation of the work described in this manuscript.
Keywords
ecotherapy, nature therapy, forensic, mental health, spirituality
Cover Page Footnote
The authors would like to acknowledge the contributions of several individuals who supported this
project. At the Southwest Centre for Forensic Mental Health Care in St. Thomas, ON: Sarah McCallum,
social worker; Allan Tetzlaff, RN/coordinator (Retired); Kent Lewis, occupational therapist/coordinator;
and Janice Vandevooren, occupational therapist/director. At St. Joseph's Health Care London, Spiritual
Care Coordinator Ciaran McKenna (Retired) and Spiritual Care Coordinator Dale Nikkel.
Credentials Display
Clark Patrick Heard, OTD, OT Reg. (Ont.); Jared Scott, MScOT, OT Reg. (Ont.); Rev'd Stephen Yeo, M.Div, RP,
CSCP
Copyright transfer agreements are not obtained by The Open Journal of Occupational Therapy
(OJOT). Reprint permission for this Applied Research should be obtained from the
corresponding author(s). Click here to view our open access statement regarding user rights
and distribution of this Applied Research.
DOI: 10.15453/2168-6408.1708
This applied research is available in The Open Journal of Occupational Therapy: https://scholarworks.wmich.edu/
ojot/vol10/iss1/7

Heard et al.: Ecospirituality in forensic mental health
Nature and participation in natural environments have markedly influenced the health care milieu
for centuries. These influences range broadly from concepts of hospital and care facility design to day-
to-day clinical application in treatment planning (Codinhoto, 2017; Wagenfeld et al., 2013). The impact
of nature as a care informer has been considered over time using various terms, but most commonly in
the modern era the terms nature or eco are used as a prefix related to various therapeutic approaches or
interventions (Hansen et al., 2017; Song et al., 2016; Summers & Vivian, 2018).
Like nature and natural environments, the unique and personal experience of spirituality has also
significantly influenced the provision of health care over time. In the occupational therapy profession,
interest in spirituality as a professional and care informer has particularly enhanced over the past 5
decades (Egan & Delaat, 1994; Newbigging et al., 2017; Townsend & Brintnell, 1990; Wilson, 2010).
Although spirituality is a topic of much professional discourse, the centrality of spirituality in the
profession has compelled its inclusion in occupational therapy practice models defining professional
practice (American Occupational Therapy Association, 2014; Townsend & Polatajko, 2013).
This qualitative study considers the outcomes of participation in a community-based
ecospirituality (the personal experience of spirituality in nature) group for nine (n = 9) individuals
affiliated with the Forensic Mental Health System in Ontario, Canada. Such individuals have come into
contact with the criminal justice system in the Province of Ontario, have been found not criminally
responsible for their offense(s) and, via legal disposition order, have been instructed to reside at the
Southwest Centre for Forensic Mental Health Care. Over a 16-week period and with a +/-120 min
duration, the group enabled the participants to visit local and freely accessible community nature spaces
proximal to the forensic hospital facility.
One factor possibly differentiating the group from more conventional therapist-driven and skill-
building groups was that it did not, specifically, focus on remediating deficits. Rather, the participants
were empowered to have personal agency and self-determination in the varied nature spaces they
attended, pending staff forensic disposition and security accountabilities to the Ontario Review Board
(Hamilton, 2017; Heard et al., 2015; Ontario Review Board, 2011). More importantly, this study
considers the outcomes of a participant experience that the participant both determines and narrates.
Review of the Literature
Conceptualizing Ecospirituality
The concept of ecospirituality as advanced by the authors (two occupational therapists and a
spiritual care professional) speaks to the intersection of the personal experience of spirituality with the
concurrent participation in nature. This is broadly consistent with more modern approaches related to
ecospirituality in health care application. In the nursing context, Lincoln (2000) speaks to an
“interconnection between human beings and the environment” (p. 228) while Delaney and Barrere
(2009) describe ecospirituality as the “spiritual dimension between human beings and the environment”
(p. 365). This study advances an immersive and participatory approach related to the ecospirituality
concept consistent with current occupational therapy and spiritual care theory.
In conceptualizing this group, the authors drew from current occupational therapy and spiritual
care theory to support development. In particular, the authors considered the Canadian Model of
Occupational Performance and Engagement (CMOP-E), noting that this model conceptually places
spirituality at the core or center of each individual. As well, the CMOP-E advocates for the concept of
occupational engagement that, beyond occupational performance, speaks specifically to concepts of
Published by ScholarWorks at WMU, 2022
1

The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
meaning making and self-efficacy that arise from occupational performance, participation, or in
reflection (Townsend & Polatajko, 2013).
The authors also specifically considered Law’s (2002) work on participation in her American
Occupational Therapy Association Distinguished Scholar Lecture, “Participation in the Occupations of
Everyday Life.” In that work, Law specifically linked the institutional environment with limited
participation outcomes for persons with disability. One factor Law noted was “issues of poverty, costs of
programs” (p. 644). In considering the ecospirituality group, one key element in its design was that it
would be practical, generalizable, and cost-efficient, enabling individuals to attend and participate in
community-based nature spaces that would be freely accessible to them during their hospital tenure (if
and when eligible for community pass participation) and also following discharge.
Theory employed in the provision of spiritual care also informed the group development. In
particular, the spiritual care professional supporting the group approached development though a lens
that first accounted for spiritually integrated psychotherapy concepts in considering how spirituality can
contribute to wholeness and wellness for each individual (Pargament, 2011). As well, Fisher’s (2011)
Four Domains Model of Spiritual Health and Well Being was considered. This model, which describes
spiritual health as a “dynamic state of being,” includes among its four domains: “the
personal…communal…environmental…transcendental” (p. 17). In particular, the authors adopted
Fisher’s position that spirituality is innate and unifies the whole person.
Concepts of ecopsychology, as informing spiritual care, also influenced the group development.
One example of this is work by Jordan (2015) who indicates: “ecopsychology has attempted to position
the psyche as both needing to connect with the environment and suffering from the results of this
disconnection” (p. 14). The articulation and examination of each participant’s experience at the
conclusion of each session enabled dialogue about what Jordan (2015) calls “the reciprocal effects of
human and natural world interaction” (p. 14). Finally, Perriam’s (2015) conceptual work on the concept
of sacred spaces informed the group development, as participation in these enables individuals to have
“active involvement in determining one’s well-being” (p. 29).
Historical Context and Informers
While a focus on “eco” or “nature” concepts may seem more prevalent today, history tells us that
the natural environment has long held a key place in the mental health care milieu. The inclusion of
accessible nature and outdoor spaces have been key tenets informing hospital and care facility design
and care application dating back more than two centuries. Indeed, these concepts came to define care
provision and hospital design for much of the 19th and early 20th century. Psychiatric facility designers
of that era, adherents to the concept of Moral Treatment, sought to create environments (then called
asylums) that enabled wellness with the natural environment as a key component. In York, English
philanthropist and mental health reformer Samuel Tuke (1815) wrote about his design for the York
Retreat:
There is not a shadow of a reason for insane persons, in general, being subjugated to the misery
of gloom as well as confinement; and when it is considered how many hours patients of this
description commonly spend in their bed-rooms, the absence of light must be, to many, a serious
privation. (p. 39)
Charland (2007), in analysis of Tuke’s influential York Retreat, noted: “location and healthy activities
were important ingredients of this healing environment (p. 66).
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
2

Heard et al.: Ecospirituality in forensic mental health
In the United States, psychiatrist and designer Thomas Story Kirkbride was significantly
influenced by Tuke’s work. Kirkbride (1880), in writing about construction and organization of
hospitals for persons with mental illness, supported grounds of “at least one hundred acres of land” and
of those:
from thirty to fifty acres immediately around the buildings, should be appropriated as pleasure
grounds, and should be so arranged and enclosed as to give the patients the full benefit of them,
without being annoyed by the presence of visitors or others. It is desirable that several acres of
this tract should be in groves or woodland, to furnish shade in summer. (p. 7)
In On the Construction, Organization, and General Arrangements of Hospitals for the Insane (1880),
Kirkbride defined mental health facility construction in North America for more than half a century.
In New Zealand in the late 19th century Sir Frederic Truby King followed a similar
philosophical approach. At the Seacliffe Asylum he linked agricultural and outdoor participation with
positive psychiatric outcomes. Stock and Brickell (2013) noted that “King shared a belief in the
importance of fresh air and sunshine—the environment, if you will; if mental instability did set in, these
elements offered the main route to recovery” (p. 109).
Outdoor occupational participation in agricultural tasks and farming has been co-occurring with
mental health facilities and prisons for centuries. Of this, Sempik (2010) noted that “opportunities for
physical labour, rehabilitation and often a pleasant pastime in the company of other people . . . the
gardens and farms satisfied physical, social and productive needs of patients” (p. 16).
Modern Context and Informers
Participation in nature has been a significant historical informer in mental health care; it also has
notable currency in the modern era. Several modern theoretical approaches have markedly influenced
what seems a renewed centrality for nature/eco inputs in health care. First, the emergence of Wilson’s
(1984) Biophilia Hypothesis identified that humans, inherently, have a fundamental and genetically
informed need to affiliate and connect with other living organisms. Another influential approach,
Kaplan’s (1995) Attention Restoration Theory, posited that participation in nature can promote wellness
via restoration of a limited cognitive resource, directed attention. Another currently influential approach
is the concept of Shinrin-Yoku (forest bathing). Originating in the 1980’s, forest bathing “is a traditional
Japanese practice of immersing oneself in nature by mindfully using all five senses” (Hansen et al.,
2017, p. 1). In application, research has identified some benefits for participants in reduction of stress,
anxiety, and depression symptoms (Hansen et al., 2017; Oh et al., 2017). Interest in this approach has
also included some evolution of and modification in mental health care settings to include walking in
nature proximal to care facilities with some reasonable outcomes in symptom mediation for individuals
with affective disorders and psychosis (Bielinis et al., 2019).
Interest and application of these concepts has, much like societal interest in “green” or “eco”
concepts, increased over time. This appears to correlate with reasonable evidence that participation in
green spaces and nature may potentially enable wide-ranging health benefits (Soga et al., 2020; Twohig-
Bennett & Jones, 2018) and has led to the modern conceptualization of green prescription or spending
time in nature to support wellness and mediate illness. Indeed, current generation smart phone apps have
even been developed to support this purpose (McEwan et al., 2019). Despite the centrality of these
concepts, there remain many unexplored questions about potential application and efficacy. Robinson et
al. (2020), perhaps presciently, noted, “It is important to recognize that our complex societies have
Published by ScholarWorks at WMU, 2022
3

The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
evolving views, social behaviours, and health-related needs, and it is unrealistic to view spending ‘time
in nature’ as a panacea” (p. 2).
Given the relative centrality of nature and eco concepts it is perhaps not surprising that clinical
application in mental health care has been notable. For example, research has examined participation in
nature via walking to both mediate stress (Marselle et al., 2019) and reduce rumination (Lopes, 2020).
Other applications have included applied outdoor mindfulness (Djernis et al., 2019) and even using
nature participation as an adjunct to traditional return-to-work rehabilitation (Sahlin et al., 2015).
Occupational therapy has mirrored this enhanced focus on nature and eco inputs. The profession
has a lengthy and diverse history of using nature in assessment and intervention and, in particular, via
gardening and horticulture (Wagenfeld & Atchison, 2014). This has included, but not been limited to,
supporting participant well-being and inclusion (Diamant & Waterhouse, 2010); considering
participation impacts for urban office workers (Schefkind et al., 2019); and accounting for the unique
influence and impact of spirituality (Unruh, 1997; Unruh & Hutchinson, 2011). Interdisciplinary work,
involving occupational therapy inputs, has also been published in application of gardening and
horticulture in supporting incarcerated females (Toews et al., 2018) and in several design applications in
correctional settings (Toews et al., 2020; Wagenfeld & Winterbottom, 2021).
The use of nature, and horticulture in particular, in supporting care for varied conditions has also
informed the occupational therapy literature. Among such work are studies that consider the impact of
therapy involving nature application and sensory garden design for individuals with autism spectrum
disorders (Singley et al., 2016; Wagenfeld et al., 2019). Design of outdoor spaces for individuals with
PTSD has also been specifically considered (Wagenfeld et al., 2013).
Several studies have specifically noted the impact of horticulture therapy in mental illness.
Sempik et al. (2014) identified positive changes in social interaction scoring following such
participation. Kam and Siu (2010) reported significantly decreased anxiety, depression, and stress
following a short (2 week) participation in a structured horticultural activity program. Cipriani et al.
(2018) reported positive outcomes from participation in a greenhouse program, including feelings of
accomplishment for participants. Summary analysis via systemic review shows participation in nature
via horticulture therapy to “improve client factors and performance skills” (Cipriani et al., 2017, p. 47).
The Forensic Mental Health Context
The built forensic mental health environment is secure and supports a somewhat externally
structured social and participatory environment (Manual of Operating Guidelines, 2019). Security
measures, both active and passive, further define the space and each individual’s ability to navigate in it
(Eggert et al., 2014). Often, in such designs there are purposefully constructed nature spaces or “therapy
courtyards” and interior spaces offering enhanced natural light exposure (Behavioral Healthcare, 2015).
Immersive and self-determined participation outdoors and in nature, as may be common for non-
hospitalized individuals, is not typically viable or available in those settings (Heard et al., 2015).
While modern facility design compassionately prioritizes purpose-built nature courtyards, access
to natural light, and enhanced views of nature, these offer neither an immersive nor a community-
consistent opportunity for normative personal interaction with nature (Karlin & Zeiss, 2006; Sine &
Hunt, 2009). Helsel (2018), in the context of providing spiritual care, has indicated that “land and person
are tied up in an inextricable relationship” (p. 23). It is that relationship that inspired the ecospirituality
group and this study.
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
4

Heard et al.: Ecospirituality in forensic mental health
This qualitative study considers the research question: What is the meaning and experience
associated with participating in the ecospirituality group for persons with serious and persistent mental
illness who reside in a forensic mental health setting
Method
This study employed a qualitative research method that is consistent with Interpretative
Phenomenological Analysis (IPA) in supporting data analysis and related coding (Smith, et al., 2009).
This approach seemed the most reasonable as the purpose of this study was to enable some
understanding of the experience and meaning of immersive and autonomous participation in nature
spaces for individuals affiliated with a forensic mental health facility (Creswell, 2007; Smith et al.,
2009). Smith (2011) has identified that “IPA is concerned with the detailed examination of personal
lived experience, the meaning of experience to participants and how participants make sense of that
experience” (p. 9). Prior to implementation of the study, institutional approval was obtained from the
Research Ethics Board at the University of Western Ontario.
Participants
IPA is “an idiographic approach, concerned with understanding particular phenomena in
particular contexts, IPA studies are conducted on small sample sizes” (Smith et al., 2009, p. 49). In this
study, a process was put in place to obtain a sample consistent with an IPA approach. First, potential
participants were identified by the group facilitators (occupational therapist and spiritual care
professional). Following identification, the actual recruitment, consent, and interview process was
facilitated by a third member of the research team, occupational therapist Jared Scott. Scott was a
member of the community mental health team affiliated with the hospital. It is notable that this clinician
and research team member did not have any role in the actual facilitation of the ecospirituality group.
Scott also did not have any clinical contact with any of the participants prior to initiation of the
recruitment, consent, and interview processes. Application of a recruitment and consent process of this
nature mediated potential for coercion and enhanced the potential credibility of the data set. Given this
context and approach, nine (n = 9) individuals residing at a large forensic mental health facility in
Ontario, Canada, were recruited for participation.
In effecting of the above plan, individuals who indicated potential interest in participation were
initially met by the co-investigator responsible for recruitment, consent, and interview. At that time, a
letter of information was provided and follow-up arranged regarding study related questions. Following
this process, informed consent could be obtained. It is notable that no payment, benefits, or other
incentives were provided to any participant. While this approach to recruitment did, potentially, enable a
convenience sample, it is important to note that research consistent with IPA requires both purposive
and homogeneous sampling (Smith et al., 2009).
In working with the sample, an inclusion and exclusion criteria consisting of several parts was
applied. The first component of the inclusion criteria required that all participants be persons with a
diagnosis of serious and persistent mental illness and reside at the Southwest Centre for Forensic Mental
Health Care under the jurisdiction of the Ontario Review Board secondary to their being found not
criminally responsible because of commission of a serious criminal offense. Second, all participants
included in the research must have participated in the Occupational Therapy/Spiritual Care
Ecospirituality group program. In terms of exclusion criteria, any participant could be excluded from the
study if the assessment of their clinical treatment team and/or the study investigators determined they
could not safely participate.
Published by ScholarWorks at WMU, 2022
5

The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
The participants in this study were representative of the demographic characteristics of patients
at the hospital. The sample (n = 9) was comprised of seven males and two females, and this was broadly
consistent with gender ratios in the facility at the time of study completion. In terms of age, the sample
ranged between 32 and 67 years with a mean age of 51.6 years and a median age of 54 years. Tenure in
the forensic mental health system ranged between 2.5 and 16 years with a mean of 8.0 years. The sample
was diagnostically diverse with schizophrenia, schizoaffective disorder, bipolar disorder, and delusional
disorder representing the majority of the primary diagnoses.
Procedures
The participants in the study took part in a group called the ecospirituality group. This group was
supported once per week over a 16-week period with a +/- 120 min duration. The group was facilitated
by occupational therapy and/or spiritual care staff at each session with support from hospital nursing
staff, as clinically indicated, in considering forensic mental health responsibilities to the Ontario Review
Board. This approach enabled forensic client attendance at various nature and green spaces in the
community accessible to the Southwest Centre for Forensic Mental Health Care. While forensic
responsibilities were taken into account, the participants were maximally enabled to experience the
nature setting as autonomously as possible (i.e., group facilitators maintained observation of participants
over lines of sight enabling, typically, several thousand square meters, or more, for individuals to
independently access). In application, this enabled the participants to experience the nature settings via
their own preferences. This meant that individual participants could choose to access the nature space
independently and to sit quietly and reflectively on their own. It also meant that individuals might
choose to sit with peers or to walk some distance with them apart from other group members. Each
individual participant was granted the agency to choose how they wished to participate and, accordingly,
to define and narrate their own unique experience. At the conclusion of each group session spiritual care
or occupational therapy staff supported a short group reflection exercise of +/- 15 min. Participation in
the reflection was voluntary, not recorded, and included three questions:
• How was this experience for you?
• What did you notice (both internally, thoughts and feelings, and around you, externally)?
• What will you take away from this experience?
Data Collection
After consent was obtained and documented, a brief interview with each participant was
undertaken. This interview occurred in the secure hospital setting at a time and location of the
participant’s choosing and was facilitated by co-investigator Scott. The interview consisted of the
collection of limited demographic information and several standardized questions. Responses were
documented, verbatim, onto the interview form. The interview form did not contain any data that could
specifically identify the research participant.
Standardized questions on the interview form related specifically to participation in the
Occupational Therapy/Spiritual Care Ecospirituality group. They read as follows:
• How would you describe the experience of participating in the Occupational Therapy/Spiritual
Care Ecospirituality group?
• How did you feel while participating in the Occupational Therapy/Spiritual Care Ecospirituality
group?
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
6

Heard et al.: Ecospirituality in forensic mental health
• How did participation in the Occupational Therapy/Spiritual Care Ecospirituality group impact
or affect your stay in the hospital?
Interview participation time ranged from +/- 25 min on the low end to +/- 60 min in total. The
transcribed data from each interview ranged between 2 and 4 pages.
Data Analysis
The collected data was immediately transcribed following the completion of all nine interviews.
A coding process was then initiated. The coding team included the principal investigator, a spiritual care
co-investigator, and a staff social worker. The first step of the coding process was completed using an
editing style of analysis whereby each coder independently analyzed the transcribed interview data and
emergent themes were identified (Jongbloed, 2000; Smith & Osborn, 2008). The three members of the
coding team then met to collaboratively determine overarching or superordinate themes. After reaching
agreement on definitions for each of the superordinate or overarching themes, these were tested for
consistency. Accordingly, coding team members independently coded one transcript using the final
coding scheme and definitions. Final coding agreement was found to be 87.1%.
Trustworthiness
Rodham, Fox, and Doran (2015) have published specifically on the concept of analytical
trustworthiness in IPA. They note that, “typically authors explain how they conduct interpretative
phenomenological analysis (IPA), but fail to explain how they ensured that their analytical process was
trustworthy” (p. 59). Aware of Rodham et al.’s (2015) work, our team has prioritized the same concepts
highlighted in their article, including a sensitivity to context, a focus on rigor, evident transparency, and
documentation of impact.
Rodham’s team focuses on a process that advocates data coding at a team level (consistent with
our own). Rodham’s team advocates that all analysts participate in listening to the recordings (our team
transcribed the data and our analysts reviewed all of that content). Second, they advise sharing of any
fieldwork notes made from each interview (our team included this content, as indicated). Third, they
advise some inclusion of reflexive content in transcripts (our team specifically named our approaches to
trustworthiness, provided a rationale for the same, and maintained a field journal). Finally, Rodham’s
team “emphasize the importance of establishing a supportive environment where colleagues engaged in
a shared analysis of the data can question and critically engage in one another’s interpretations” (p. 69).
Our research team takes these processes seriously. Using multiple coders on our teams from
different professions and backgrounds enabled the shared analysis Rodham et al. (2015) advocate. Our
team, using three professionally diverse coders, identified that this approach supports triangulation by
theory and perspective (Hammell & Carpenter, 2000). We also used peer review as “this enables a
further instance of triangulation” (Hammell & Carpenter, 2000, p. 111). Perhaps most importantly, our
team employed member checking, as this supports “enhancing credibility and the ability for participants
to meaningfully contribute to the research process” (Doyle, 2007, p. 894). Finally, we will securely store
our records for 15 years enabling our team the ability to revisit the content, if indicated.
Results
The data analysis supported the identification of several unique themes for each interview
question. These themes described the meaning and experience associated with participating in the
ecospirituality group program for persons residing at a forensic mental health care facility.
Published by ScholarWorks at WMU, 2022
7
The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
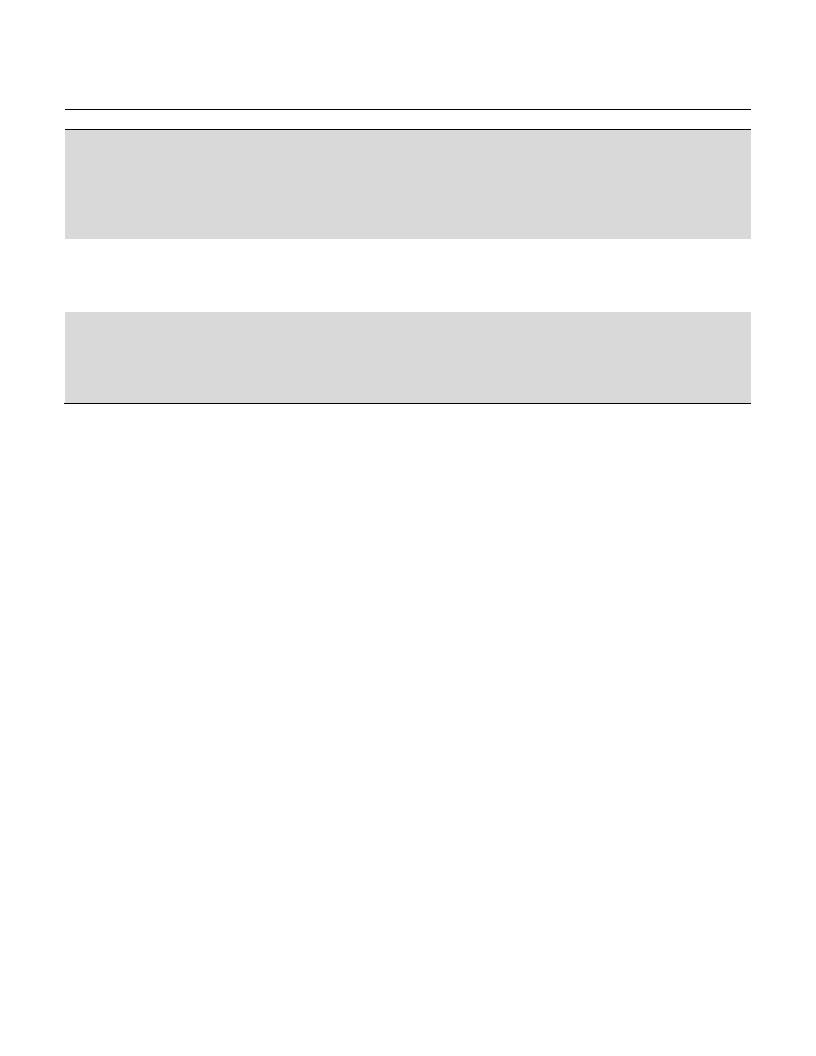
Table 1
Superordinate and Overarching Themes
Question
How would you describe the experience
of participating in the Occupational
Therapy and Spiritual Care
Ecospirituality group?
Superordinate/Overarching Themes
• A sense of communion and connection with nature
• An opportunity for open and unguarded reflection and
relaxation
• A strengthened human connection and a sense of
camaraderie though shared experience in nature
How did you feel while participating in • A sense of peace, comfort, serenity, and accomplishment
the Occupational Therapy and Spiritual • A feeling of freedom, autonomy, and personal agency
Care Ecospirituality group?
• A connection to the personally sacred
How did participation in the
Occupational Therapy and Spiritual
Care Ecospirituality group impact or
affect your stay in the hospital?
• Regenerative and restorative participation
• Easy and accessible stress relief
• Supported resiliency and meaningful connection with
others
The Experience of Ecospirituality
The participants described several outcomes related to their participation in the Occupational
Therapy/Spiritual Care Ecospirituality group. An overarching theme described the experience as
enabling a sense of communion and connection with nature. One participant, in positing this view,
stated: “I describe it as being surrounded by nature. It’s always interesting to get fresh air and to observe
the animals and trees and everything to do with nature” (Participant 3). Several other participants
similarly reflected this type of immersive and personal connection with nature: “the entire time I was out
in nature and things were balanced at the time. It was a very precious moment for me. I was out
observing nature being one with nature” (Participant 9). Another noted, succinctly: “some people need it
more than others; you feel like you’re at home” (Participant 1).
While connection with nature was identified as important, the participants in the group also
identified the opportunity for unguarded reflection and relaxation. One participant noted that the group
enabled them, stating: “You can think about you. It’s time for that and it’s nice because it’s peaceful”
(Participant 8). A second followed this line of thinking, noting: “I was absorbing all the positive energy
given to me by the surroundings I was in, by the people I was with. Everything was very organized and
put together so I could just be and think and not worry” (Participant 9). Several of the participants
reported on the opportunity to be in nature: “it was relaxing” (Participant 7) and “I love the outdoors, I
like to be outdoors, it helps me think” (Participant 5).
Being in nature and sharing an experience with a group of peers enabled the participants to
identify feelings of an enhanced human connection and a sense of camaraderie. A participant spoke to
this shared experience: “Overall, very good. It was relaxing. I think there was a bonding between
individuals who went, to take a look at nature and reflect on it. To discuss it as a group with other people
in a group setting” (Participant 4). Others reflected positively on the supportive facilitation: “I also find
it a very friendly atmosphere with your fellow patients and the staff. It’s very relaxing and I enjoy the
camaraderie we have together” (Participant 3). Another similarly noted: “it was very serene and the
spiritual care staff was inspiring in their discussions about nature. It was an enjoyable experience”
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
8

Heard et al.: Ecospirituality in forensic mental health
(Participant 6). A participant summarized their feelings of the group influence, noting: “it is different
than just going for a walk because you are with the group. You can be with other people and think about
things. You can share with others and talk to them about your thoughts” (Participant 8).
The Effect of Ecospirituality
A key question in this study looked at how the participants considered the effect of participation
or how they felt while immersed in nature via a supported group context. The participants identified
themes that spoke to important personal outcomes. The first of these related to feeling a sense of peace,
comfort, serenity, and accomplishment. These findings were reflected in various personal narratives: “I
was going through a pretty rough time in my life at the time so it felt pretty good. Just the staff and
being in the environment, and being around people who care about you. It was really good” (Participant
2). Another spoke to the relevance of being outside: “when I’m outside I am comforted. I feel good
when I’m outside or in nature. Both in a group or own my own. It’s about being outside – it makes me
feel better” (Participant 6). The peaceful nature of the outdoors spoke to some participants: “it was a lot
more therapeutic being outside. Being somewhere special” (Participant 2). Finally, a participant spoke
specifically to the personal value of participation: “you learn stuff and I feel like you have accomplished
something. It’s a good feeling” (Participant 1).
Each participant narrative was unique but spoke to their connection with nature and with the
group:
When you walk along with other people you have to carry on a conversation or you can walk
along in silence, too. They say silence is golden. I like the company of walking with others and I
feel like that’s assistance, too. But I also want to do things on my own and be independent.
(Participant 3)
The opportunity to participate independently, with peers or staff, informed some of the participants: “we
all shared our ideas and thoughts about nature and the spirituality of nature and the balance of the
universe and I learned a lot” (Participant 9). Another indicated: “when I walk by myself I say a few
poems to myself or pray a little bit” (Participant 3). One participant summarized their experience:
“Peaceful. The different venues, for example, we saw turtles and saw a crane and different animals and
insects and it was a great experience to share that with people. I really enjoyed it” (Participant 4).
The Impact of Ecospirituality
The participants in the Occupational Therapy/Spiritual Care Ecospirituality group discussed the
impacts of the group and how it affected their stay in the hospital. These impacts, it seems, were multi-
faceted and spoke to three fairly discrete themes. The first of these spoke to the concept that
participation in the group was both regenerative and restorative. One participant noted:
I do look forward to the group being in nature but sometimes I have to be persuaded to go.
Sometimes I feel aches and pains through my body and I have to be careful so sometimes I’m not
sure if I want to go. But when I go, I always feel better inside. (Participant 3)
Another participant reflected: “well, it was good to get out of the hospital. To go for a ride in the van
and I felt good after we got back. The walks made me feel good” (Participant 7). Finally, a participant
spoke to a more personal impact: “it created memories for me because I didn’t know the forensic
Published by ScholarWorks at WMU, 2022
9

The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
hospital offered groups like that. I was very happy to get out and get to the outside world, in nature,
more” (Participant 9).
Beyond supporting regenerative and restorative outcomes, the participants’ experiences also
spoke to an overarching theme of easy and accessible stress relief. The participants described this
content in varied ways with some quite explicitly identifying this feature of the group:
I feel less stressed out. The time is helpful to break my daytime down. I feel more rested.
Overall, it was a good experience. Everyone in the hospital could do it and it would help them. It
is nice to be outside the hospital. (Participant 8)
Others were less explicit but noted a similar sentiment: “it made me a lot happier. It brought me back to
myself a little bit and I was able to focus on myself more” (Participant 2). Some participants spoke to
more of a long-term applicability in terms of stress relief and application of eco concepts in their own
day-to-day living: “I can go outside and find a quiet place or park or trees and walk on my own to help
me calm down, to just be out in the open” (Participant 7). Other participants spoke to more immediate
application, noting: “You get rid of pressure. In your body and in your head. You get rid of all the stress,
all your pressures. You feel good about yourself. You relieve the stress” (Participant 5).
The final overarching theme in terms of impact related to how participation supported resiliency
and connection to others. Several of the participants spoke to a more practical view of connection and
related resiliency development: “It’s good programs. It helps people connect with each other in new and
different ways” (Participant 1). Another participant reflected this same concept: “In the group you are
not by yourself, you have other people with you who experience the same thing, nature, and they can
share that experience with you” (Participant 7). Other participants took a broader view of the group and
related connection and resiliency outcomes:
It changed my memories of the hospital. It built up my emotions and trust with the hospital. It
showed me there was some sort of care and connection to nature and the world. To make people
feel valued and connected. To have hope and faith, to recognize how we celebrate that – our
connection to nature as people, as humans. (Participant 9)
Perhaps most importantly, the group supported a real connection between peers: “it was something that I
talked to and with my peers about. I would tell other people where we went and what we saw and the
different questions that were asked of us and my reflections” (Participant 4).
Discussion
Ecospirituality Group Participation in Context
The results of this study identify a number of compelling narratives. Among these, the
participants in the Occupational Therapy/Spiritual Care Ecospirituality group described an experience
that enabled both personal autonomy and self-determinism. They described this participation experience
as enabling success and feelings of achievement. This would be consistent with those elements of
empowerment that are a core concept of the World Health Organization’s (WHO) vision of health
promotion. Indeed, the WHO (2010) note that:
For the individual, the empowerment process means overcoming a state of powerlessness and
gaining control of one’s life. The process starts with individually defined needs and ambitions
and focuses on the development of capacities and resources that support it. The empowerment of
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
10

Heard et al.: Ecospirituality in forensic mental health
individuals is intended to help them adopt self-determination and autonomy, exert more
influence on social and political decision-making processes and gain increased self-esteem. (p. 1)
The participants spoke plainly to these concepts when describing the participation experience of the
ecospirituality group. This concept of empowerment appears particularly relevant in the forensic mental
health milieu where opportunities for autonomy and self-determination in occupational participation
cannot always be part of the recovery journey secondary to those legal aspects that inform care (Ontario
Review Board, 2011).
In reviewing the outcomes of this study in consideration of current literature related to mental
health care, it appears that many existing approaches do not tend toward privileging the autonomy and
personal agency of each individual. Rather, it appears that much of this work is targeted toward enabling
the client to meet some externally defined wellness or discharge related criteria. Hamilton (2017)
describes this situation as secondary to “deficit-centric discourses” defining care interactions (p. 2). As
an example of this concept, the high volume of literature supporting group interventions related to social
skill development, anger management, and assertiveness speak directly to this narrative. This is not to
minimize the potential clinical relevance, perhaps, of such groups, but it is compelling to consider the
influence of externally defined, deficit informed care.
For individuals residing in secure mental health facilities, or secure settings more generally,
concepts of autonomy, determinism, and success experience may not always be common informers in
care participation (Heard et al., 2015). As such, participation in the ecospirituality group, as described in
this study, does mark a fairly significant departure from the existing deficit informed hegemony. For
health care providers considering this type of group it may feel like there is some tension in supporting a
more open-ended participant-defined experience versus supporting an outcome driven group answerable
to some type of deficit. If such tensions can be accepted, then the ecospirituality group offers a
particularly practical and cost-effective approach to care that speaks to real-world applicability in terms
of leisure participation, relaxation, stress relief, and connection with the personally sacred.
Ultimately, health care providers have at their disposal a domain, nature, in which spirituality
and spiritual health can be nurtured and promoted. This domain, according to Fisher (2011), moves
“beyond care and nurture for the physical and biological, to a sense of awe and wonder…[and]…for
some…the notion of unity with the environment” (p. 22). Fisher argues that spiritual health is the
“fundamental dimension of people’s overall health and well-being, permeating and integrating all the
other dimensions of health,” describing spiritual health as a “dynamic state of being, reflected in the
quality of relationships that people have in up to four domains of spiritual well-being: personal
domain…communal domain…environmental domain… transcendental domain” (p. 17). To assist in
explaining the interrelationship between the four domains, Fisher refers to the notion of progressive
synergism, stating it “implies that the more embracing domains of spiritual well-being not only build on,
but also build up, the ones they include” (p. 23). The authors of this study did observe multiple
occurrences where a participant’s sense of self, connection to others, and to the personally sacred were
maximized because of their accessing local nature spaces and their capacity to self-author these
experiences.
Implications for Practice
This study describes the significant impacts that access to natural environments, and the ability
to self-author those experiences, can have in the lives of individuals residing in a forensic mental health
Published by ScholarWorks at WMU, 2022
11

The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
system. While the sample was comprised of individuals affiliated with a forensic mental health hospital,
it may be reasonable to posit that the most powerful impacts of participation would be optimal in any
care setting or context. Indeed, the potential to support feelings of freedom, autonomy, personal agency,
stress relief, and relaxation is a compelling driver for any clinical work. Given that narrative, the results
of this study identify several important implications for mental health practice and, perhaps, clinical
practice more generally:
• Enabling immersive experiences in nature supports participants to access, learn, and potentially
replicate cost-efficient opportunities for stress relief.
• Unlike deficit informed approaches, these experiences (where individuals have the autonomy to
determine the scope of their participation in the nature space) privilege the personal agency,
experience, and wisdom of each participant.
• The results of this study speak to the centrality of nature as an informer in care. At a practical
level it appears that enhancing access to such spaces may have a significant and positive impact
on occupational performance, wellness, and the personal experience of spirituality. Accordingly,
it may be relevant to consider how accessible nature and immersive nature spaces might play an
enhanced role in the care paradigm via building and facility design, supported community
access, or programmatic focus.
• Participation in ecospirituality group creates space or allows for theological and spiritual
reflection and enables the development of personal wisdom.
Limitations and Directions for Future Research
It is important to note that this study does have limitations. First, while the sample correlates
fairly reasonably with the demographic norms for the facility, the study did occur at a single forensic
hospital in Ontario, Canada. This sample size, at n = 9, is relatively small and, at some level, this may
limit potential generalizability. That said, it should be noted that in employing a design consistent with
IPA, it is required that the sample is more or less homogeneous and purposefully selected (Smith et al.,
2009). In considering future research, further study may be compelling in considering the varied
potential benefits that self-authored and autonomous participation in nature might enable for different
clinical populations. It is not difficult to forecast that this type of easily accessible and inexpensive
spirituality-focused intervention may well have clinical applicability with a wide array of clinical
populations.
Conclusion
The outcomes of this study speak to the centrality of personal interaction with nature and its
implication for health, wellness, and connection to the personally sacred. The opportunity to narrate this
interaction via personal agency in those nature spaces, and to allow what Kirkbride (1880) might refer to
as “the full benefit of them,” also appears relevant (p. 7). In a practical way, supporting and enabling
immersive personal interaction with nature for those who are mentally ill, incarcerated, or otherwise
vulnerable may offer an important pathway to wellness. Compellingly, it appears that this pathway was,
historically, quite explicitly acknowledged and accounted for in the works of Tuke (1815) and Kirkbride
(1880) and in the practice of Truby King (Stock & Brickell, 2013). Perhaps the wisdom of past
generations regarding the value of immersive participation and personal autonomy in natural
environments may hold a key to future healing, wellness, occupational performance, and experience of
the personally sacred.
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
12
Heard et al.: Ecospirituality in forensic mental health
References
American Occupational Therapy Association. (2014).
Occupational therapy practice framework
domain and process. American Journal of
Occupational Therapy, 68 (Suppl. 1), S1–S48.
https://doi.org/10.5014/ajot.2014.682006
Behavioral Healthcare. (2015). Design showcase:
Southwest centre for forensic mental health care.
http://cdn.coverstand.com/36947/263804/7d4c19
e46171f890787e0fc92513bac962d80975.1.pdf
Bielinis, E., Jaroszewska, A., Lukowski, A., & Takayama,
N. (2019). The effects of a forest therapy
programme on mental hospital patients with
affective and psychotic disorders. International
Journal of Environmental Research and Public
Health, 17(1), 118.
https://doi.org/10.3390/ijerph17010118
Charland, L. C. (2007). Benevolent theory: Moral
treatment at the York retreat. History of
Psychiatry, 18(1), 61–80.
https://doi.org/10.1177/0957154X07070320
Cipriani, J., Benz, A., Holmgren, A., Kinter, D.,
McGarry, J., & Rufino, G. (2017). A systematic
review of the effects of horticultural therapy on
persons with mental health conditions.
Occupational Therapy in Mental Health, 33(1),
47–69.
https://doi.org/10.1080/0164212X.2016.1231602
Cipriani, J., Georgia, J., McChesney, M., Swanson, J.,
Zigon, J., & Stabler, M. (2018). Uncovering the
value and meaning of a horticulture therapy
program for clients at a long-term adult inpatient
psychiatric facility. Occupational Therapy in
Mental Health, 34(3), 242–257.
https://doi.org/10.1080/0164212X.2017.1416323
Codinhoto, R. (2017). Healing architecture. In R. Cooper
& E. Tsekleves (Eds.), Design for health (p.
111–156). Routledge.
Creswell, J. W. (2007). Qualitative inquiry and research
design: Choosing among five approaches (2nd
ed.). Sage.
Delaney, C., & Barrere, C. (2009). Ecospirituality: The
experience of environmental meditation in
patients with cardiovascular disease. Holistic
Nursing Practice, 23(6), 361–369.
https://doi.org/10.1097/HNP.0b013e3181bf381c
Diamant, E., & Waterhouse, A. (2010). Gardening and
belonging: Reflections on how social and
therapeutic horticulture may facilitate health,
wellbeing and inclusion. The British Journal of
Occupational Therapy, 73(2), 84–88.
https://doi.org/10.4276/030802210X1265806279
3924
Djernis, D., Lerstrup, I., Poulsen, D., Stigsdotter, U.,
Dahlgaard, J., & O’Toole, M. (2019). A
systematic review and meta-analysis of nature-
based mindfulness: Effects of moving
mindfulness training into an outdoor natural
setting. International Journal of Environmental
Research and Public Health, 16(17), 1–19.
https://doi.org/10.3390/ijerph16173202
Doyle, S. (2007). Member checking with older women: A
framework for negotiating meaning. Health Care
for Women International, 28(10), 888–908.
https://doi.org/10.1080/07399330701615325
Egan, M., & Delaat, M. (1994). Considering spirituality in
occupational therapy practice. Canadian Journal
of Occupational Therapy, 61(2), 95–101.
https://doi.org/10.1177/000841749406100205
Eggert, J. E., Kelly, S. P., Margiotta, D. T., Hegvik, D.
K., Vaher, K. A., & Kaya, R. T. (2014). Person–
Environment interaction in a new secure forensic
state psychiatric hospital. Behavioral Sciences &
The Law, 32(4), 527–538.
https://doi.org/10.1002/bsl.2127
Fisher, J. (2011). The four domains model: Connecting
spirituality, health and well-being. Religions, 2,
17–28. https://doi.org/10.3390/rel2010017
Hamilton, S. A. (2017). Clients’ experiences of recovery-
oriented care for schizophrenia: A qualitative
research study [Unpublished doctoral
dissertation]. Duquesne University.
Hammell, K. W., & Carpenter, C. (2000). Evaluating
qualitative research. In K. W. Hammell, C.
Carpenter, & I. Dyck (Eds.), Using qualitative
research: A practical introduction for
occupational and physical therapists (pp. 107–
119). Churchill Livingstone.
Hansen, M. M., Jones, R., & Tocchini, K. (2017).
Shinrin-yoku (forest bathing) and nature therapy:
A state-of-the-art review. International Journal
of Environmental Research and Public Health,
14(8), 851.
https://doi.org/10.3390/ijerph14080851
Heard, C. P., Scott, J., & Yeo, R. S. (2015). Walking the
labyrinth: Considering mental health consumer
experience, meaning making, and the
illumination of the sacred in a forensic mental
health setting. Journal of Pastoral Care &
Counseling, 69(4), 240–250.
https://doi.org/10.1177/1542305015616102
Helsel, P. B. (2018). Loving the world: Place attachment
and environment in pastoral theology. Journal of
Pastoral Theology, 28(1), 22–33.
https://doi.org/10.1080/10649867.2018.1475977
Jongbloed, L. (2000). Choosing the methodology to
explore the research. In K. W. Hammell, C.
Carpenterm & I. Dyck (Eds.), Using qualitative
research: A practical introduction for
occupational and physical therapists (pp. 13–
21). Churchill Livingstone.
Jordan, M. (2015). Nature and therapy: Understanding
counselling and psychotherapy in outdoor
spaces. Routledge.
Kam, M., & Siu, A. (2010). Evaluation of a horticultural
activity programme for persons with psychiatric
illness. Hong Kong Journal of Occupational
Therapy, 20(2), 80–86.
https://doi.org/10.1016/S1569-1861(11)70007-9
Kaplan, S. (1995). The restorative benefits of nature:
Toward an integrative framework. Journal of
Environmental Psychology, 15(3), 169–182.
https://doi.org/10.1016/0272-4944(95)90001-2
Karlin, B. E., & Zeiss, R. A. (2006). Environmental and
therapeutic issues in psychiatric hospital design:
Toward best practices. Psychiatric Services,
57(10), 1376–1378.
https://doi.org/10.1176/appi.ps.57.10.1376
Kirkbride, T. S. (1880). On the construction, organization
and general arrangements of hospitals for the
insane with some remarks on insanity and its
treatment. (2nd ed.). J.B. Lippincott.
Law, M. (2002). Participation in the occupations of
everyday life. The American Journal of
Published by ScholarWorks at WMU, 2022
13
The Open Journal of Occupational Therapy, Vol. 10, Iss. 1 [2022], Art. 7
Occupational Therapy, 56(6), 640–649.
https://doi.org/10.5014/ajot.56.6.640
Lincoln, V. (2000). Ecospirituality: A pattern that
connects. Journal of Holistic Nursing, 18(3),
227–244.
https://doi.org/10.1177/089801010001800305
Lopes, L. (2020). Nature can get it out of your mind: The
rumination reducing effects of contact with
nature and the mediating role of awe and mood.
Journal of Environmental Psychology, 71,
101489.
https://doi.org/10.1016/j.jenvp.2020.101489
Manual of Operating Guidelines – Provincial Psychiatric
Hospitals. (1995). Wording of custodial
disposition orders.
http://www.orb.on.ca/scripts/en/legal/psych-
hosp-guidelines.pdf
Marselle, M., Warber, S., & Irvine, K. (2019). Growing
resilience through interaction with nature: Can
group walks in nature buffer the effects of
stressful life events on mental health?
International Journal of Environmental
Research and Public Health, 16(6), 986.
https://doi.org/10.3390/ijerph16060986
McEwan, K., Richardson, M., Sheffield, D., Ferguson, F.,
& Brindley, P. (2019). A smartphone app for
improving mental health through connecting
with urban nature. International Journal of
Environmental Research and Public
Health, 16(18), 3373.
https://doi.org/10.3390/ijerph16183373
Newbigging, C., Stewart, D., & Baptiste, S. (2017).
Spirituality in occupational therapy: Enhancing
our practice through the use of the four domains
model. Occupational Therapy Now, 19(1), 13–15.
Oh, B., Lee, K. J., Zaslawski, C., Yeung, A., Rosenthal,
D., Larkey, L., & Back, M. (2017). Health and
well-being benefits of spending time in forests:
Systematic review. Environmental Health and
Preventive Medicine, 22(1), 1–11.
https://doi.org/10.1186/s12199-017-0677-9
Ontario Review Board. (2011). About us.
http://www.orb.on.ca/scripts/en/about.asp#infor
mation
Pargament, K. I. (2011). Spiritually integrated
psychotherapy: Understanding and addressing
the sacred. The Guilford Press.
Perriam, G. (2015). Sacred spaces, healing places:
Therapeutic landscapes of spiritual significance.
Journal of Medical Humanities, 36(1), 19–33.
https://doi.org/10.1007/s10912-014-9318-0
Robinson, J., Jorgensen, A., Cameron, R., & Brindley, P.
(2020). Let nature be thy medicine: A
socioecological exploration of green prescribing
in the UK. International Journal of
Environmental Research and Public Health,
17(10), 1–24.
https://doi.org/10.3390/ijerph17103460
Rodham, K., Fox, F., & Doran, N. (2015). Exploring
analytical trustworthiness and the process of
reaching consensus in interpretative
phenomenological analysis: lost in transcription.
International Journal of Social Research
Methodology, 18(1), 59–71.
https://doi.org/10.1080/13645579.2013.85236
Schefkind, S., Hock, N., & Wagenfeld, A. (2019).
Measuring emotional response to a planting
activity for staff at an urban office setting: A
https://scholarworks.wmich.edu/ojot/vol10/iss1/7
DOI: 10.15453/2168-6408.1708
pilot study. The Open Journal of Occupational
Therapy, 7(2), 1–11.
https://doi.org/10.15453/2168-6408.1532
Sahlin, E., Ahlborg, J., Tenenbaum, A., & Grahn, P.
(2015). Using nature-based rehabilitation to
restart a stalled process of rehabilitation in
individuals with stress-related mental illness.
International Journal of Environmental
Research and Public Health, 12(2), 1928–1951.
https://doi.org/10.3390/ijerph120201928
Sempik, J. (2010). Green care and mental health:
Gardening and farming as health and social
care. Mental Health and Social Inclusion, 14(3),
15–22. https://doi.org/10.5042/mhsi.2010.0440
Sempik, J., Rickhuss, C., & Beeston, A. (2014). The
effects of social and therapeutic horticulture on
aspects of social behaviour. The British Journal
of Occupational Therapy, 77(6), 313–319.
https://doi.org/10.4276/030802214x1401872313
8110
Sine, D. M., & Hunt, J. M. (2009). Following the
evidence toward better design. Behavioral
Healthcare, 29(7), 45.
Singley, K., Griner, C., DeDominic, T., & Wagenfeld, A.
(2016). Therapy in the natural environment:
Growing solutions for autism spectrum
disorder. OT Practice, 21(11), 21–24.
Smith, J. A., Flowers, P., & Larkin, M. (2009).
Interpretative phenomenological analysis:
Theory, method and research. Sage.
Smith, J. A. (2011). Evaluating the contribution of
interpretative phenomenological analysis. Health
Psychology Review, 5(1), 9–27.
https://doi.org/10.1080/17437199.2010.510659
Smith, J. A., & Osborn, M. (2008). Interpretative
phenomenological analysis. In J. Smith (Ed.),
Qualitative psychology: A practical guide to
research methods (pp. 53–80). Sage.
Soga, M., Evans, M., Tsuchiya, K., & Fukano, Y. (2020).
A room with a green view: The importance of
nearby nature for mental health during the
COVID-19 pandemic. Ecological Applications,
e2248–e2248. https://doi.org/10.1002/eap.2248
Song, C., Ikei, H., & Miyazaki, Y. (2016). Physiological
effects of nature therapy: A review of the
research in japan. International Journal of
Environmental Research and Public Health,
13(8), 781.
https://doi.org/10.3390/ijerph13080781
Stock, P. V., & Brickell, C. (2013). Nature's good for you:
Sir Truby King, Seacliff Asylum, and the
greening of health care in New Zealand, 1889–
1922. Health and Place, 22, 107–114.
https://doi.org/10.1016/j.healthplace.2013.03.002
Summers, J. K., & Vivian, D. N. (2018). Ecotherapy – A
forgotten ecosystem service: A review. Frontiers
in Psychology, 9, 1389.
https://doi.org/10.3389/fpsyg.2018.01389
Toews, B., Wagenfeld, A., & Stevens, J. (2018). Impact
of a nature based intervention on incarcerated
women. International Journal of Prisoner
Health, 14(4), 232–243.
https://doi.org/10.1108/IJPH-12-2017-0065
Toews, B., Wagenfeld, A., Stevens, J., & Shoemaker, C.
(2020). Feeling at home in nature: A mixed
method study of the impact of visitor activities
and preferences in a prison visiting room
garden. Journal of Offender Rehabilitation,
14
Heard et al.: Ecospirituality in forensic mental health
59(4), 223–246.
https://doi.org/10.1080/10509674.2020.1733165
Townsend, E., & Brintnell, S. (1990). Developing
guidelines for client-centred occupational
therapy practice. Canadian Journal of
Occupational Therapy, 57(2), 69–76.
https://doi.org/10.1177/000841749005700205
Townsend, E., & Polatajko, H. (2013). Enabling
occupation II: Advancing an occupational
therapy vision for health, well-being & justice
through occupation. CAOT.
Tuke, S. (1815). Description of the Retreat, an institution
near York, for insane persons of the Society of
Friends: Containing an account of its origin and
progress, the modes of treatment, and a
statement of cases. Pierce, Isaac.
Twohig-Bennett, C., & Jones, A. (2018). The health
benefits of the great outdoors: A systematic
review and meta-analysis of greenspace exposure
and health outcomes. Environmental Research,
166, 628–637.
https://doi.org/10.1016/j.envres.2018.06.030
Unruh, A. (1997). Spirituality and occupation: Garden
musings and the Himalayan blue poppy.
Canadian Journal of Occupational Therapy,
64(1), 156–160.
https://doi.org/10.1177/000841749706400112
Unruh, A., & Hutchinson, S. (2011). Embedded
spirituality: Gardening in daily life and stressful
life experiences: Embedded spirituality.
Scandinavian Journal of Caring Sciences, 25(3),
567–574. https://doi.org/10.1111/j.1471-
6712.2010.00865.x
Wagenfeld, A., & Atchison, B. (2014). ‘Putting the
occupation back in occupational therapy’: A
survey of occupational therapy practitioners’ use
of gardening as an intervention. The Open
Journal of Occupational Therapy, 2(4), 1–19.
https://doi.org/10.15453/2168-6408.1128
Wagenfeld, A., Roy-Fisher, C., & Mitchell, C. (2013).
Collaborative design: Outdoor environments for
veterans with PTSD. Facilities, 31(9/10), 391–
406.
https://doi.org/10.1108/02632771311324954
Wagenfeld, A., Sotelo, M., & Kamp, D. (2019).
Designing an impactful sensory garden for
children and youth with autism spectrum
disorder. Children, Youth and Environments,
29(1), 137–152.
https://doi.org/10.7721/chilyoutenvi.29.1.0137
Wagenfeld, A., & Winterbottom, D. (2021). Coping on
the inside: Design for therapeutic incarceration
interventions - A case study. Work, 68(1), 97–
106. https://doi.org/10.3233/WOR-203360
Wilson, E. (1984). Biophilia. Harvard University Press.
Wilson, L. (2010). Spirituality, occupation and
occupational therapy revisited: Ongoing
consideration of the issues for occupational
therapists. British Journal of Occupational
Therapy, 73(9), 437–440.
https://doi.org/10.4276/030802210X1283936752
6219
WHO Regional Office for Europe, European
Commission. (2010). User empowerment in
mental health. World Health Organization.
http://www.euro.who.int/__data/assets/pdf_file/0
020/113834/E93430.pdf
Published by ScholarWorks at WMU, 2022
15