
International Journal of
Environmental Research
and Public Health
Article
Analysis of Urban Forest Healing Program Expected Values,
Needs, and Preferred Components in Urban Forest Visitors with
Diseases: A Pilot Survey
Kwang-Hi Park
Department of Nursing, College of Nursing, Gachon University, Incheon 21936, Korea; parkkh@gachon.ac.kr;
Tel.: +82-32-820-4204
Citation: Park, K.-H. Analysis of
Urban Forest Healing Program
Expected Values, Needs, and
Preferred Components in Urban
Forest Visitors with Diseases: A Pilot
Survey. Int. J. Environ. Res. Public
Health 2022, 19, 513. https://
doi.org/10.3390/ijerph19010513
Academic Editors: Won Sop Shin and
Bum-Jin Park
Abstract: Although the effectiveness of urban forest therapy has been studied and proven, most
people are not well aware of the positive healing effects of urban forests that are easily accessible in
daily life compared to the known healing effect of forests located outside urban areas. In addition,
there has been a study on the analysis of urban forest healing program needs in the general population,
but there is a lack of evidence on the expected values and needs of urban forest healing for people
with diseases. Therefore, this pilot survey aimed to investigate the expected values, needs, and
preferred components of urban forest healing programs in urban forest visitors with disease via an
online user survey and see if there were any differences in the purpose of the urban forest visits and
expected values of urban forest healing depending on the type of disease. The survey was conducted
on 294 urban forest visitors with diseases. About 79% of respondents agreed with the healing effects
of urban forest, however most respondents expected healing effects on mental health rather than on
physical health (“mood change” was the highest with score of 4.43/5, followed by “reliving stress”
(4.35/5) and “mental and physical stability” (4.31/5)). In addition, more than 82.0% of respondents
agreed to participate in the program if a healing program for disease was developed. The results of
the current pilot survey indicate that the purpose of the urban forest visits and expected values of
urban forest healing were largely not different by the type of disease, and people with disease had
a relatively lower awareness and lower expected values of urban forest healing effects on physical
health, but high demand for the program. Urban forest therapy programs should be developed based
on the specific clinical characteristics of the disease to maximize the effectiveness of the program.
Additionally, policies should be implemented to promote the beneficial effects of urban forest healing
not only for mental health but also for physical health.
Keywords: urban forest; disease; healing effect; survey
Received: 3 December 2021
Accepted: 31 December 2021
Published: 4 January 2022
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2022 by the author.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
1. Introduction
Forest healing, which is a practice comprising of activities utilizing forests to improve
immunity, mental health and physical health has been established as a culture in South
Korea, with annual visits to forests exceeding one million in 2014 [1]. The number of visitors
to forest healing centers has rapidly increased over time to reach 76,000 in 2010, 1.15 million
in 2014, and 2.27 million 2019 in South Korea. Similarly the number of users of forest healing
programs in the country has surged to 1067 in 2009, 1.7 million in 2015, and 1.8 million
in 2019 [1]. In addition, it is predicted that the demand for forest healing will continue to
increase with time due to the escalation in environmental health related risk factors, such
as particulate matter in the air, as well as increased economic development and demand for
leisure [2–4]. However, most of the healing forests are located in the suburbs, making it
difficult to obtain healing benefits of forests in everyday life. In South Korea, most of the
national and public healing forests are located on average 90 min away from metropolitan
cities, by car. Moreover, it is particularly difficult for the mobility disabled, elderly, pregnant
women, and those with diseases affecting movement, to use the healing forests due to the
Int. J. Environ. Res. Public Health 2022, 19, 513. https://doi.org/10.3390/ijerph19010513
https://www.mdpi.com/journal/ijerph

Int. J. Environ. Res. Public Health 2022, 19, 513
2 of 14
lack of accessibility [5]. In addition, the country has become an aging society with an aging
rate of 7.2% in 2000. This rate increased to 14.3% in 2018, and is forecast to rise to 42.5% by
2065, making it the highest in the world [6]. As the national population continues to age,
the interest in benefits of urban forests is also soaring. Therefore, interest in urban forests
with high accessibility is increasing [7].
Urban forests were first defined by Jorgensen in 1974 as “a specialized branch of
forestry, and it has in its objective the cultivation and management of trees for their present
and potential contribution to the physiological, sociological, and economic well-being
of urban society”. Thereafter, Deneke defined urban forestry in 1993 as “the sustained
planning, planting, protection, maintenance, and care of trees, forests, greenspace, and
related resources in and around cities and communities for economic, environmental, social,
and public health benefits for people [7]”. Preserving forest cover as urban populations
grow into surrounding rural areas, as well as trying to restore essential aspects of the urban
environment after construction, are all part of the definition. Continued growth at the
urban front increases environmental and public health concerns, as well as the possibility of
generating educational and environmental links between nature and urban people. Urban
and community forestry is composed of development of citizen engagement coupled with
aid for investment in sustained tree planting, protection, and care programs. A multitude
of definitions have been proposed over the years, but they all acknowledge that urban
forests do not end at the limits of the city.
Nowadays, the main focus of primary health care practices is the identification of
risk factors for preventing diseases and aims to improve the quality of life through this
and the prevention of chronic conditions, which is different from the past that focused
on diagnosing and treating diseases [8]. In particular, it is becoming important for most
people living in cities to establish and implement long-term care plans to promote health
as chronic diseases related to stress from their daily lives increase [9]. As such, the various
therapeutic effects of urban forests have been proven. Especially in South Korea, where
about 89% of the population lives in metropolitan areas, forest recreation and healing in
urban forests that can be easily accessible by the people are needed [10].
Many previous studies have summarized the relationship between the natural envi-
ronment and human health [11–15]. Recent trends indicate a growing interest in urban
forests, as these are seen as a mechanism to encourage physical activity, facilitate social
cohesion, and promote both psychological and physiological restoration [1,14]. Various
studies have shown the benefits of urban forest therapy programs and their effects in a
forest environment [11,12,15–17]. The Korean government is also promoting public health
by designating the living areas and surrounding lands as urban forests for healing effect on
stress caused by urban life [18]. Therefore, it is necessary to continuously develop various
healing programs and related facilities for preventing disease and health in urban forests,
and for this, the need for an evaluation of the multiple functions of urban forests, including
healing benefits, is a prerequisite.
1.1. Operational Definition of “Urban Forest”
Referring to previous studies [19–21], in this study we defined urban forests as “Trees,
forests, and greenspaces that are located within urban living area and play a plethora
of ecological and social roles in the lives of local residents”. These are limited to places
with an infrastructure for hiking trails and fitness facilities. Ecological functions include
particulate matter reduction, noise reduction, furnishing animal and plant habitats, and
providing green spaces, while social functions include exercise, rest, leisure, experience,
and education.
1.2. Healing Effects of Forest
1.2.1. General Benefits of Urban Forest
Urbanization, advancements in technology, crowding, and fast-paced life have dra-
matically decreased the time humans spend in natural surroundings. The lifestyle of people

Int. J. Environ. Res. Public Health 2022, 19, 513
3 of 14
living in cities has been shown to produce negative emotions such as depression, pain
and anxiety [22]. Ulrich, through his stress reduction theory, has described the need for
urban residents to experience nature. This explains that interaction with nature helps in
stress reduction as well as enhancing the physiological functioning of humans [11]. Forest
healing or forest therapy is one of the therapies provided by nature for improving mental
and physical health and includes many environmental factors such as landscape, phyton-
cides, sounds, lights, and negative ions [21]. Then, healing effect of urban green areas may
provide feasible health benefits, as they are easily accessible [11]. Although it is relatively
less than natural forests, the healing effects of urban forest have been proven in many
studies [23–25]. As stated by Han et al., urban forests vary from one region to another, have
several spaces and plantations as well as infrastructure for various forest activities, and
therefore, they can be utilized by urban dwellers as a ‘healing space’ [17]. Social scientists
have also established that urban forests and green spaces improve mental well-being [26].
Previous studies observed that forest healing programs in urban forests enhance
mental health such as resilience, stress reduction [17,27]. Lee et al. concluded that the
therapeutic effect of urban forest therapy on the psychological healing of middle-aged
women thought focus group interview [11]. Furthermore, another study found that urban
green space improved children’s emotional happiness and behavior resilience [28]. Urban
forests have been found to be effective not only for mental health but also for physical health
such as decreasing pulse rate, blood pressure, variability of heart rate, nervousness, tension,
depression in middle-aged and elderly subjects [12,13,15,29]. A study on the association
between urban tress and various health benefits revealed that more urban tree canopy were
mainly associated with lower incidence of obesity, high blood pressure, asthma, and type
2 diabetes [30].
1.2.2. Healing Effects of Forest Therapy for Chronic Diseases
Forest healing is not considered as a remedy for diseases, rather it’s a healing activity
that aids in the maintenance of patients’ health and the enhancement of both physiological
and psychological functions [1]. As such, many studies have been conducted that says
that the healing effects of forest has a positive effect on various types of chronic diseases.
Recent study have shown that forest therapy improves depression and anxiety in addition
to reducing blood pressure by stabilizing the autonomic nervous system in elderly subjects
with dementia [20]. Lee et al. examined the biophysical and psychosocial effects of different
types of forest on middle-aged women with metabolic syndrome and found that wild
forest had a positive effect on insulin responses, pulse rate, oxidative stress markers, and
stress hormone level [31]. Chun et al. also demonstrated that forest therapy was beneficial
for treating depression and anxiety symptom in patients with chronic stroke; therefore,
forest therapy can be specifically used for chronic patients who cannot receive standard
treatment [32]. In addition, many studies have shown that forest healing is effective in
cardiopulmonary disease patients [33–35]. Direct evidence was provided by Mao et al.
in favor of forest therapy being beneficial for patients with chronic heart failure and
therefore it was considered that it has the potential to be used as an adjuvant therapy
for cardiovascular disorders [34]. With regard to cancer patients, previous studies have
stated that forest healing therapy not only increased physiological factors such as natural
killer cell activity [36–39], but also psychological status such as depression, anxiety, and
sleep quality [36,40–42].
1.3. Aim of the Study
Despite the studied and proven effectiveness of urban forest therapy, most people
are not completely aware of the positive healing effects of urban forests compared to the
healing effects of forests located outside urban areas.
Employing an Evidence-based practice (EBP) which is a problem-solving strategy
that incorporates the best evidence of well-designed studies, experts’ opinion and patients’
value or preference is important to be established as a healthcare program which can lead

Int. J. Environ. Res. Public Health 2022, 19, 513
4 of 14
to better patient outcome for individuals with diseases [43]. A lot of evidence already
supports that forest healing program has a positive effect on improving physiological and
psychological functions and many experts assured that the importance of forest healing
program should be highlighted. However, although there has been a study on the analysis
of urban forest healing program needs in the general population [44] there is still a lack
of evidences to infer the needs and expected value of urban forest healing programs for
individuals with diseases. Therefore, the purpose of this pilot survey was to investigate
the purpose of the urban forest visits, expected values, and preferred components of urban
forest healing programs based on developed questionnaires by expertise for urban forest
visitors with known diseases in South Korea. The secondary purpose of the study was to
see if there were any significant differences in the purpose of the urban forest visits and
expected values of urban forest healing depending on the type of disease.
2. Materials and Methods
2.1. Ethical Approval
The study was conducted in accordance with the guidelines of the Declaration of
Helsinki and approved by the Gachon University Institutional Review Board (1044396-
202106-HR-136-01). The purpose of this study was fully explained before the survey was
conducted. All participants who agreed to participate in the survey were required to sign
an informed consent form before beginning the survey.
2.2. Participants
A total of 294 urban forest visitors who had visited urban forests within the last two
years with disease (aged between 15 and 69 years), residing in two metropolitan cities
in South Korea participated in an online survey conducted by a research institution with
a panel composed of the same distribution as the Korean population sensor and secure
representation. A non-probability sample extraction was used to select 294 subjects with
diseases classified in the Korea National Health and Nutrition Examination Survey in
2019. Three thousand seven hundred thirty-five emails were distributed to the panel,
1239 checked their emails and 407 participated in the survey. Among them, 15 respondents
who did not meet the inclusion criterion and 98 respondents who did not complete the
survey were excluded, then, a total of 294 were included as a valid sample for this pilot
survey. The respond rate was 32.8%.
2.3. Questionnaire
A questionnaire was created for this study in order to investigate the awareness of
urban forest visitors with regard to the effects of urban forest healing. A survey titled
“Questionnaire on expected values and needs of urban forest healing effects” was developed
through systematic literature reviews of previous studies [19,44,45] and consultation with a
panel of experts. A draft questionnaire was prepared after several meetings with reference
to the literature review. Next, the validity of the draft questionnaire was investigated by a
panel of experts to determine whether it included appropriate components for the purpose
of the study and was suitable for the patients. The questionnaire consisted of four sections:
(1) general characteristics of the respondents, (2) purpose of urban forest visit, (3) expected
values of the urban forest healing effect, (4) needs of urban forest healing programs,
and (5) preferred components of urban forest healing programs. General population
characteristics included age, sex, education level, marital status, income, occupation, and
presence of disease. The purpose of the urban forest visits, expectation values of the urban
forest, and needs of the urban forest healing program were rated on a 5-point Likert scale.
2.4. Data Collection
An online survey was conducted between 21 to 29 July 2021. The questionnaire was
distributed to residents of two metropolitan cities with urban forests in South Korea via
email with an online survey link. The purpose of the study was described in the first part

Int. J. Environ. Res. Public Health 2022, 19, 513
5 of 14
of the questionnaire, and all valid questionnaires collected during the survey period were
used for the analysis.
2.5. Statistical Analysis
The data were analyzed using the statistical software IBM SPSS Statistics for Windows,
version 26.0 (IBM Corp., Armonk, NY, USA). Frequency analysis was performed according
to the characteristics of each item. Quantitative variables were calculated as mean and
standard deviation (SD), while categorical variables were presented as frequency and
percentage. The Kolmogorov-Smirnov test was used to test for the normality of the data.
A chi-squared test was used to compare the distribution of preferred components of
urban forest healing program in the age and disease categories. One-way repeated analysis
of variance (ANOVA) was used to compare the expected values among type of disease.
Additionally, one-way analysis of covariance (ANOCA) test with Bonferroni-adjusted post
hoc test was used to explore the influences of any variables over the dependent variables.
The level of significant was set at α = 0.05.
3. Results
Demographic characteristics of the respondents are described in Table 1. Among the
respondents, 50.5% were women, and the average age was 50.3 ± 14.5 years. The most
common primary diseases reported were circulatory system diseases (55.4%), followed by
respiratory system diseases (11.6%), and musculoskeletal system diseases (9.5%). Multiple
responses were available if there were more disease other than the primary disease, and
83 respondents had more than two diseases. Including multiple responses, a total of 294 re-
spondents had 398 diseases. The most common diseases were circulatory system disease
(43.7%), followed by endocrine system and metabolic diseases (17.1%), respiratory sys-
tem diseases (12.6%), musculoskeletal system diseases (10.8%), depression (8.8%), cancers
(5.0%), and others (2.5%). Other diseases included atopic dermatitis, Parkinson’s disease,
and prostate disease.
Table 1. Demographic characteristics of the respondents (n = 294).
Characteristics
Age (year), mean ± SD
Gender (women), n (%)
Education level, n (%)
No education or elementary school or middle school
High school
Undergraduate
Graduate school
Marital status, n (%)
Single
Married
Divorced
Economic status, n (%)
Low (below KRW 3,000,000)
Middle (KRW 3,000,000–7,000,000)
High (above 7,000,000)
Missing
Type of primary disease, n (%)
Circulatory system diseases
Musculoskeletal system diseases
Respiratory system diseases
Endocrine system and Metabolic diseases
Cancers
Depression
Others
Total (n = 294)
n (%) or Mean ± SD
50.3 ± 14.5
134 (45.6)
5 (1.7)
82 (27.9)
167 (56.8)
40 (13.6)
78 (26.5)
206 (70.1)
10 (3.4)
79 (26.9)
156 (53.1)
45 (15.3)
14 (4.8)
163 (55.4)
28 (9.5)
34 (11.6)
27 (9.2)
14 (4.8)
24 (8.2)
4 (1.4)
Int. J. Environ. Res. Public Health 2022, 19, 513
6 of 14
3.1. Purpose of Urban Forest Visit
“Purpose of the urban forest visit” section of the questionnaire contained 18 sub-
objectives under four major categories, all of which could be scored between 1 and 5 points
(1 point: least, 5 points: best). Among the four major categories, “rest/healing” was the
highest scored with 3.97 out of 5, followed by “nature-friendly” (3.70). “risk aversion” was
the least common purpose of the urban forest visit (3.52). Among the sub-objectives, “taking
a walk” under “healthcare” section had the highest score of 4.40 and “maintaining health”
followed closely at 4.09. However, the overall score of “healthcare” was low because of
the low scores of “healing a disease” (2.80) and “participating in healing program” (3.06)
sub-objectives (Table 2).
The purpose of the urban forest visit was significantly different among type of disease
in “healthcare” in the major category, as well as “healing program participation” and “main-
taining health” under “healthcare” section (p < 0.05). However, there was no significant
difference in the purpose of the urban forest visit after controlling for the effect of age
(p > 0.05).
3.2. Expected Values of the Urban Forest Healing Effect
Table 3 shows expected values of the healing effect of urban forest. Before, asking
the expected values of the urban forest healing, the respondents were asked whether they
agreed with the fact that urban forests have healing effects. Two hundred thirty-four (79.6%)
respondents agreed with the healing effects of urban forest. The agreement of the urban
forest healing effect was significantly different depending on the type of disease (p < 0.001).
Only those who agreed were given the follow-up questionnaire. Among the healing
effects provided by urban forest, “mood change” scored the highest with 4.43 out of 5,
followed by “relieving stress” (4.35) and “mental and physical stability” (4.31). “Prevention
of diseases” scored the lowest with 3.73 points followed by “Improving immunity” (3.93).
Expected value of the urban forest healing effect was significantly different among
type of disease in “healthcare”, “improving immunity”, “prevention of diseases”, and
“rejuvenation” (p < 0.05). However, only the expected values of “improving immunity”
differed significantly on types of disease after controlling for the effect of age (F(5227) = 2.208,
p = 0.047). Bonferroni-adjusted post hoc test showed that respondents with circulatory
system diseases had significantly higher expected value of the urban forest healing effect
than those with endocrine system and metabolic diseases in terms of “improving immunity”
(p = 0.035).
3.3. Needs of Urban Forest Healing Programs
Before proceeding with this part of the survey, the respondents were asked whether
they needed an urban forest healing program. Of the total respondents, 81.3% agreed on
the need for an urban forest healing program, and only 3.7% disagreed (Table 4).
When asked the question, “Would you like to participate in the program if healing
program is established in an urban forest for diseases?” 82.0% respondents “agreed” to
participate, while 5.4% did not want to participate in the program.
The necessity and the intention to participate in the urban forest healing program
participation were not significantly different depending on the type of disease (p > 0.05).
The most appropriate time duration of the healing program was 60 min for 121 respon-
dents (50.2%), followed by 120 min for 51 patients (21.2%), and 90 min for 38 respondents
(15.8%). Among the respondents, 106 (44.0%) thought that the appropriate cost of the heal-
ing program in urban forest per visit was “less than KRW 5000 (USD 4.2)” and 78 (32.4%)
thought it should be within “KRW 10,000 (USD 8.4)” (Table 4).
Int. J. Environ. Res. Public Health 2022, 19, 513
7 of 14
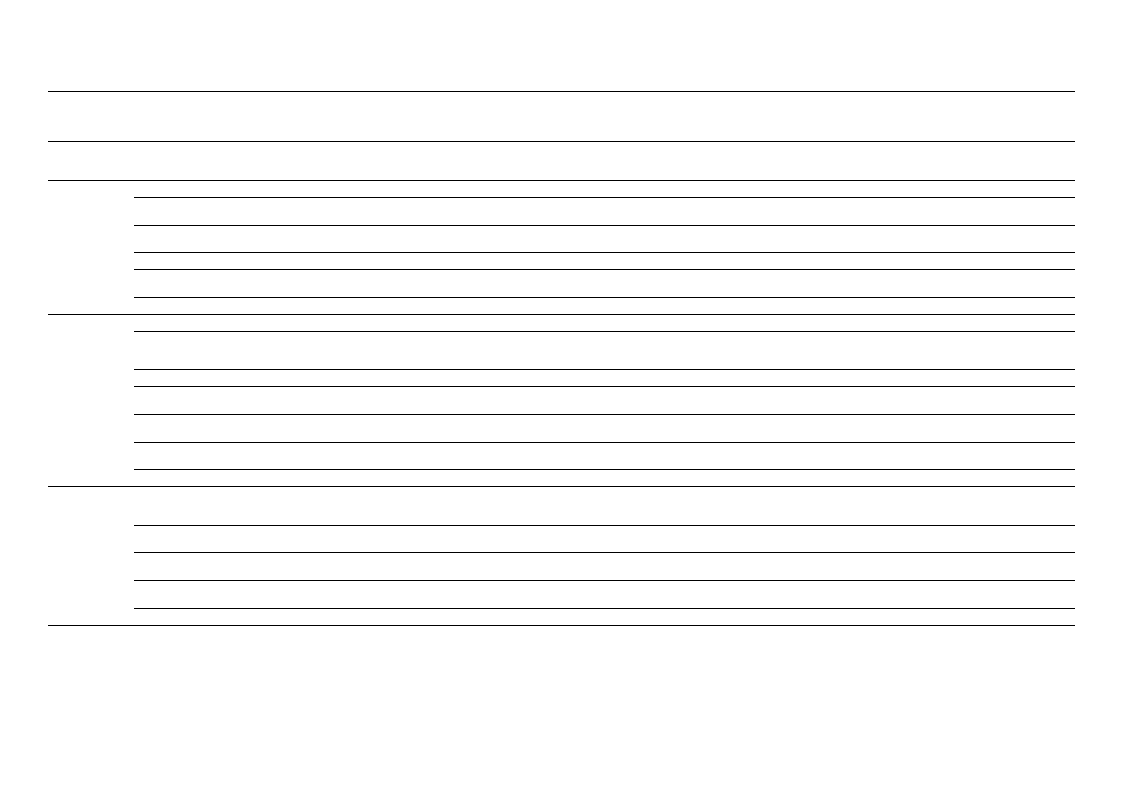
Table 2. Questionnaire derived data on the purpose of visit to urban forest in urban forest visitors (n = 294).
Purpose of Visit to Urban Forest
Rest
/Healing
Healthcare
Risk
Aversion
Rest/healing
Spending time
in nature
Escaping from
daily routine
Relieving stress
Physical/mental
rejuvenation
Overall
Taking a walk
Healing
program
participation
Simple exercise
Maintaining
health
Prevention of
disease
Healing a
disease
Overall
Avoiding
particulate
matter
Breathing in
fresh air
Avoiding noise
in the city
Avoiding heat
island phenom
Overall
Circulatory
Diseases
(n = 163)
4.16 ± 0.63
4.02 ± 0.75
3.84 ± 0.82
3.99 ± 0.75
4.15 ± 0.70
4.03 ± 0.56
4.42 ± 0.62
3.24 ± 1.14
3.87 ± 0.90
4.20 ± 0.75
3.55 ± 0.96
2.87 ± 1.04
3.69 ± 0.65
3.02 ± 1.01
3.86 ± 0.88
3.53 ± 0.94
3.80 ± 0.86
3.55 ± 0.78
Musculo-Skeletal
Diseases
(n = 28)
3.94 ± 0.96
4.16 ± 0.88
3.70 ± 1.09
3.66 ± 0.76
3.94 ± 0.71
3.88 ± 0.77
4.53 ± 0.51
3.35 ± 1.25
3.94 ± 0.74
4.29 ± 0.61
3.63 ± 0.91
2.89 ± 0.85
3.77 ± 0.57
3.14 ± 0.93
4.01 ± 0.88
3.57 ± 0.94
4.01 ± 0.85
3.68 ± 0.80
Respiratory
Diseases
(n = 34)
4.19 ± 0.55
3.83 ± 0.89
3.64 ± 1.00
3.79 ± 0.96
4.02 ± 0.83
3.90 ± 0.65
4.45 ± 0.52
2.38 ± 1.15
3.83 ± 0.69
3.90 ± 0.77
3.00 ± 1.08
2.40 ± 0.91
3.33 ± 0.56
2.69 ± 1.04
3.69 ± 1.11
3.07 ± 1.27
3.64 ± 0.98
3.27 ± 0.94
Endocrine &
Metabolic Diseases
(n = 27)
3.91 ± 0.88
4.07 ± 0.66
3.82 ± 0.93
3.79 ± 1.00
3.94 ± 0.96
3.91 ± 0.71
4.53 ± 0.63
2.92 ± 1.05
3.70 ± 0.90
4.10 ± 0.58
3.54 ± 0.87
2.95 ± 1.02
3.62 ± 0.60
3.01 ± 0.78
3.79 ± 0.82
3.70 ± 0.80
3.91 ± 0.83
3.60 ± 0.69
Cancers
(n = 14)
3.90 ± 1.04
3.79 ± 1.22
3.74 ± 1.28
4.01 ± 0.75
3.96 ± 0.80
3.88 ± 0.70
4.12 ± 0.97
3.13 ± 1.19
3.30 ± 1.15
3.90 ± 1.22
3.30 ± 1.22
2.91 ± 1.07
3.44 ± 0.69
2.86 ± 0.93
3.85 ± 1.07
3.35 ± 1.03
3.74 ± 0.93
3.45 ± 0.89
Depression
(n = 24)
4.04 ± 0.81
3.89 ± 0.41
3.93 ± 0.88
3.89 ± 0.88
4.04 ± 0.84
3.96 ± 0.77
4.07 ± 0.70
2.50 ± 1.32
3.46 ± 1.04
3.61 ± 1.05
3.21 ± 1.02
2.75 ± 1.07
3.27 ± 0.84
2.82 ± 0.91
3.68 ± 1.07
3.61 ± 1.10
3.93 ± 0.91
3.51 ± 0.85
Others
(n = 4)
3.39 ± 0.68
3.93 ± 0.41
2.86 ± 1.17
3.57 ± 0.58
3.75 ± 0.90
3.50 ± 0.59
4.46 ± 0.68
3.39 ± 0.68
3.75 ± 0.90
3.39 ± 0.68
2.86 ± 1.17
2.14 ± 0.58
3.33 ± 0.51
2.14 ± 1.01
2.68 ± 1.58
3.39 ± 1.22
3.39 ± 0.36
2.90 ± 0.40
Overall
4.09 ± 0.72
3.99 ± 0.81
3.79 ± 0.91
3.91 ± 0.81
4.07 ± 0.76
3.97 ± 0.63
4.40 ± 1.27
3.06 ± 0.64
3.80 ± 1.19
4.09 ± 0.80
3.45 ± 0.99
2.81 ± 1.01
3.60 ± 0.66
2.96 ± 0.98
3.81 ± 0.94
3.49 ± 0.99
3.81 ± 0.87
3.52 ± 0.81
F(p)
1.549 (0.163)
0.598 (0.732)
1.034 (0.404)
0.944 (0.464)
0.671 (0.673)
0.845 (0.536)
1.725 (0.115)
3.463 (0.003)
1.496 (0.180)
2.915 (0.009)
1.971(0.070)
1.332 (0.243)
2.781 (0.012)
1.159 (0.329)
F(p) †
-
0.215 (0.972)
-
-
-
-
1.379 (0.223)
1.300 (0.257)
-
1.152 (0.333)
0.607 (0.724)
-
0.701 (0.649)
0.330 (0.921)
1.353 (0.234)
1.217 (0.298)
0.659 (0.683)
1.116 (0.353)
0.842 (0.538)
-
-
0.478 (0.824)
Int. J. Environ. Res. Public Health 2022, 19, 513
8 of 14
Table 2. Cont.
Purpose of Visit to Urban Forest
Nature
Friendly
Enjoying the
natural scenery
Using nature
and green space
Communicating
with nature
Overall
Circulatory
Diseases
(n = 163)
3.75 ± 0.87
Musculo-Skeletal
Diseases
(n = 28)
3.73 ± 0.78
Respiratory
Diseases
(n = 34)
3.71 ± 1.03
Endocrine &
Metabolic Diseases
(n = 27)
3.70 ± 0.74
Cancers
(n = 14)
3.79 ± 0.68
3.89 ± 0.79
3.91 ± 0.77
3.95 ± 0.89
3.98 ± 0.64
3.96 ± 0.55
3.51 ± 0.96
3.42 ± 0.91
3.36 ± 1.03
3.42 ± 0.99
3.02 ± 1.34
3.70 ± 0.77
3.69 ± 0.71
3.67 ± 0.84
3.70 ± 0.62
3.59 ± 0.74
† After controlling the covariate (age) which was significantly related to the dependent variables.
Depression
(n = 24)
3.89 ± 0.91
3.79 ± 0.77
3.61 ± 1.07
3.76 ± 0.76
Others
(n = 4)
3.39 ± 0.68
3.93 ± 0.41
2.86 ± 1.54
3.39 ± 0.63
Overall
3.74 ± 0.86
3.90 ± 0.76
3.45 ± 1.01
3.70 ± 0.75
F(p)
F(p) †
0.235 (0.965)
0.151 (0.989)
0.859 (0.526)
0.197 (0.977)
-
-
0.859 (0.526)
0.308 (0.933)
Table 3. Expected values of urban forest healing effect in urban forest visitors who agreed with the urban forest healing effect (n = 234).
Expected Values of Urban
Forest Healing Effect
Healthcare
Increasing exercise effects
Maintaining vitality
Relieving stress
Mental and physical stability
Mood change
Improving immunity
Prevention of diseases
Rejuvenation
Circulatory
Diseases
(n = 133)
Musculo-Skeletal
Diseases
(n = 26)
Respiratory
Diseases
(n = 31)
Endocrine & Metabolic
Diseases
(n = 22)
Cancers
(n = 9)
Depression
(n = 13)
Overall
F(p)
F(p) †
4.38 ± 0.55
4.15 ± 0.54
4.03 ± 0.70
4.32 ± 0.60
4.44 ± 0.60
4.34 ± 0.62
4.30 ± 0.59
2.343 (0.042) 1.293 (0.268)
4.35 ± 0.57
4.18 ± 0.63
4.06 ± 0.62
4.16 ± 0.61
4.05 ± 0.80
4.29 ± 0.71
4.26 ± 0.61
1.771 (0.120)
-
4.38 ± 0.53
4.09 ± 0.62
4.15 ± 0.54
4.29 ± 0.54
4.37 ± 0.56
4.23 ± 0.46
4.30 ± 0.55
1.932 (0.090) 1.318 (0.257)
4.40 ± 0.50
4.37 ± 0.68
4.24 ± 0.52
4.32 ± 0.60
4.13 ± 0.69
4.34 ± 0.62
4.35 ± 0.55
0.770 (0.573)
-
4.34 ± 0.55
4.23 ± 0.60
4.12 ± 0.66
4.38 ± 0.60
4.44 ± 0.48
4.45 ± 0.31
4.31 ± 0.56
1.192(.314)
-
4.47 ± 0.50
4.23 ± 0.64
4.33 ± 0.58
4.48 ± 0.50
4.52 ± 0.51
4.40 ± 0.49
4.43 ± 0.53
1.253 (0.285)
-
4.40 ± 0.63
3.90 ± 0.65
3.73 ± 0.84
3.60 ± 0.52 *
4.21 ± 0.56
4.07 ± 0.84
3.93 ± 0.68
2.328 (0.044) 2.208 (0.047)
3.84 ± 0.74
3.63 ± 0.57
3.36 ± 0.96
3.57 ± 0.73
3.97 ± 0.81
3.79 ± 0.94
3.73 ± 0.79
2.399 (0.038) 1.359 (0.241)
4.31 ± 0.57
3.93 ± 0.84
3.96 ± 0.66
4.12 ± 0.73
4.29 ± 0.51
4.29 ± 0.51
4.20 ± 0.64
2.844 (0.016) 2.029 (0.062)
* Significant difference from those who with circulatory system diseases after controlling the covariate (age). † After controlling the covariate (age) which was significantly related to the
dependent variables.
Int. J. Environ. Res. Public Health 2022, 19, 513
9 of 14
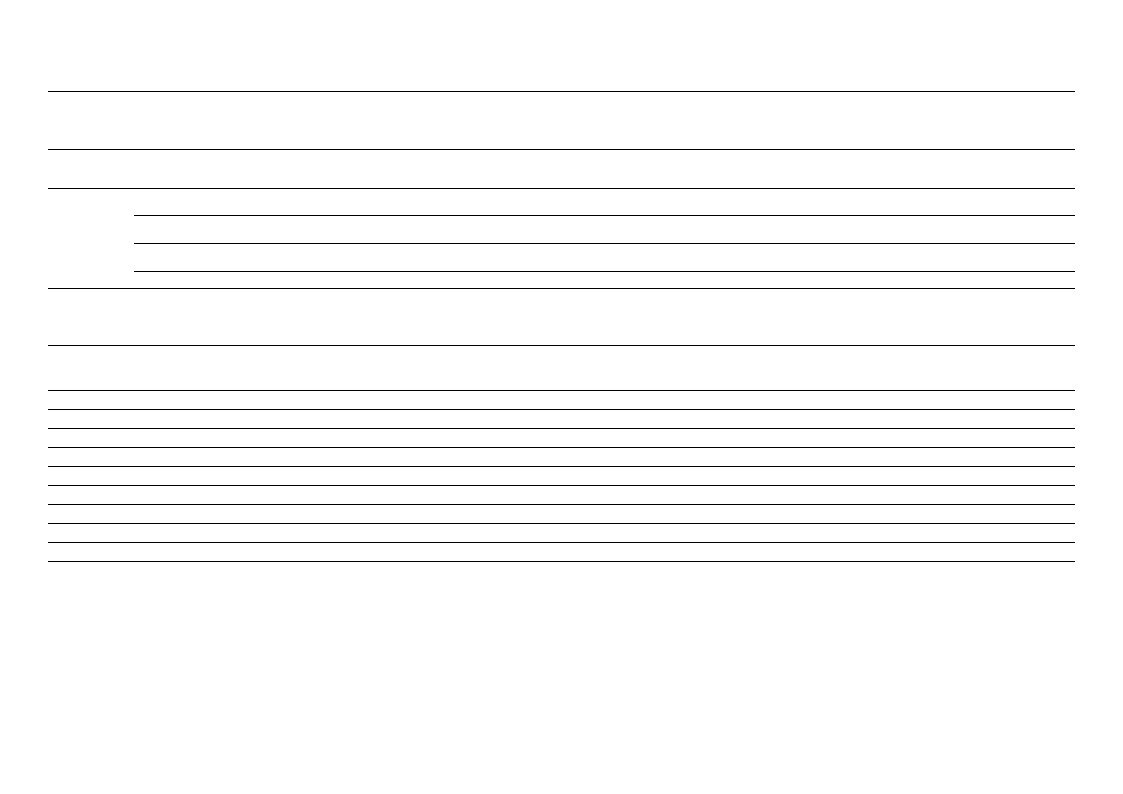
Table 4. Needs of urban forest healing programs with preferred duration and cost.
Items
Total (n = 294)
n (%)
Necessity of urban forest healing program
Strongly agree and agree
Strongly disagree and disagree
Neither agree nor disagree
Will you participate in urban forest healing program?
Strongly agree, agree, somewhat agree
Strongly disagree, disagree, somewhat disagree
Neither agree nor disagree
Preferred duration of urban forest healing program *
30-min
60-min
90-min
120-min
More than 120-min
Preferred cost of urban forest healing program *
Free
Below KRW 5000 (USD 4.2)
KRW 10,000 (USD 8.4)
KRW 10,001—20,000 (USD 8.4—16.8)
Above KRW 20,000 (USD 16.8)
239 (81.3)
11 (3.7)
44 (15.0)
241 (82.0)
16 (5.4)
37 (12.6)
25 (10.4)
121 (50.2)
38 (15.8)
51 (21.2)
6 (2.5)
1 (0.4)
106 (44.0)
78 (32.4)
50 (20.7)
6 (2.5)
* Duration and cost of urban forest healing program were asked from only those respondents who were willing to
participate in the urban forest healing program (n = 241).
3.4. Preferred Components of Urban Forest Healing Program
Table 5 shows the preferred components of the urban forest healing program for
urban forest visitors with disease. This part of questionnaire was required to be completed
by the respondents who were willing to participate in the program. Multiple responses
were provided. The most preferred component of the urban forest healing program as
reported by the respondents was, “taking a walk” (73.8%). “meditation” (57.7%) and “wind
bath” (50.2%), were also selected as components of high preference by 57.7% and 50.2% of
the respondents, respectively. On the other hand, only 23.1% agreed to inclusion of “art
therapy” in the program; “forest recreation” (24.9%) and “tea ceremony” (31.1%), were
selected as components that were less preferred.
Table 5. Preferred components of urban forest healing program.
Items
Meditation
Taking a walk
Mental and physical reinforcement
Forest gymnastics
Forest recreation
Ecological experience
Wind bath
Performance in the forest
Tea ceremony
Art therapy
Aroma therapy
Multiple answers were available.
Total (n = 241)
n (%)
139 (57.7)
178 (73.8)
117 (48.5)
109 (45.2)
60 (24.9)
88 (36.5)
121 (50.2)
95 (39.4)
75 (31.1)
65 (22.1)
84 (34.9)
4. Discussion
This pilot survey aimed to investigate the expected values, needs, and preferred
components of urban forest healing programs in urban forest visitors with disease and see
if there were any significant differences depending on the type of disease through a user

Int. J. Environ. Res. Public Health 2022, 19, 513
10 of 14
survey. Respondents were classified on the basis of disease types, and circulatory system
disease was reported by 55.4%, respiratory system diseases by 11.6%, and musculoskeletal
system diseases by 9.5% of the respondents in our study. About 70% of the participants had
diseases that demanded lifestyle improvements, including exercise and diet modifications.
This is confluent with the recent observations that people with various types of disease
are visiting urban forests and indicates that the need as well as demand for urban forest
healing programs is expected to rise in the future.
In the present study the most common purpose of visit to the urban forest was reported
as “resting and healing” followed by “nature-friendly” and “healthcare”. The “taking a
walk” sub-objective of the “healthcare” section scored high but “prevention of disease”
and “healing a disease” scored relatively low. These results are similar with the findings
of the previous study on the use of urban forests by visitors with or without diseases,
showing “change of mood” and “mental health promotion” as the highest stated purposes
of urban forest visits with “healthcare” being the least common reported purpose [44]. The
purposes of visit to the urban forest were not significantly different by type of disease after
controlling ‘age’. This shows that urban forest visitors with the purpose of “healthcare” are
more affected by age than type of diseases.
Many studies on forest healing effects have consistently shown psychological benefits
such as reduction in depression and anxiety, as well as physical effects such as decreased
blood pressure and increased NK cell activity [1,11,13,40,46]. However, people without
disease and even with disease were only aware of the psychological effects of forest healing
and were relatively unaware of the effects of forest healing on physical aspects of diseases.
In the current study 79.6% of the respondents agreed on the healing effect of urban
forest, which is similar to the results of a survey in Germany where 77.2% of respondents
were positive of the healing effect of urban forests, of which 45.5% were very confident
about the healing effect [10].
However, it was seen that the agreement with regard to physical healing effects such
as “improving immunity”, and “prevention of disease” was relatively low compared to
psychological healing effects such as ‘mood change’ and “reliving stress”. This shows that
the expectation of physical healing related to urban forest visits is low among people, which
is also reflected in the purpose of urban forest visits. This is in a similar to the previous
study, which reported that the artificial landscape beauty of urban forests is relatively less
evaluated for the healing function of forests than ecologically well-cultivated forests [9]. In
the result of the present survey, the expected values of “improving immunity” significantly
higher in patients with cardiovascular system disease after controlling for the effect of age.
This is believed to be due to the fact that urban forest visitors with cardiovascular disease
expect more to promote immunity because the immune system plays an essential role in
the development and progression of cardiovascular diseases [47].
About 81% of respondents agreed on the necessity of urban forest healing programs,
and 82% of them were willing to participate in the program and it did not differ by the
types of disease. The intention to participate in the programs was much higher in the
current study than in previous surveys showing that 47.2% of the national population [48]
and 58.3% of urban forest visitors [44] were willing to participate in the forest healing
programs. However, as Park et al. [44] did not analyze the intention to participate in the
urban forest healing program based on the presence or absence of disease, this study cannot
be directly compared with our study. It can be assumed that the respondents included in
the current study had a higher intention to participate in these programs because they had
diseases. Applying the program in combination with the conventional treatment in people
with diseases who are understood to have higher needs for forest healing programs could
have the effect of reducing social and economic costs of diseases or other health related
conditions on the healthcare system.
The preferred activities for urban forest healing programs in the decreasing order were
walking, meditation, wind bathing, and forest gymnastics. These results are somewhat
different from the previous studies on forest healing program preferences, where forest
Int. J. Environ. Res. Public Health 2022, 19, 513
11 of 14
gymnastics, wind bathing, and meditation were the highest rated activities [49,50]. ‘Walk-
ing’ was the highest preferred activity as part of the healing program in the present study
and the biggest purpose of urban forest visits, but the expected effect on physical health
was relatively low. This might be due to a relatively lack of understanding of the fact that
walking in the forest has a positive impact on physical health. In general, people are well
aware of the physical benefits of ‘walking’, but the connection to physical fitness seems
to be relatively insignificant because they think that ‘walking’ in the forest has greater
impact on psychological aspect than ‘walking’ in the concrete. This is supported by a
previous study analyzing big data on forest walking showed that walking in the forest
tends to be perceived as leisure activities that taking a walk in the forest [51]. In addition,
our results indicated that visitors with diseases had higher demands for physical activities
such as ‘walking’ and ‘gymnastics’ than people without diseases, as part of urban forest
healing programs, and this should be considered when developing suitable urban forest
healing programs for people with diseases. Moreover, since it is important to constantly
participate in these healing programs at places which are easily accessible in daily life,
urban forests may be more suitable in terms of use for people with diseases than forests
located outside urban areas. Furthermore, it was noted that except ‘walking’, the preference
for physical health-related activities was low, and further studies should be conducted in
order to promote the physical health benefits of urban forests, such as ’health promotion’
and ‘improving immunity’ in addition to the mental health benefits.
According to a Delphi survey conducted on forest healing by 19 experts in medicine,
psychology, and forestry, to predict the preferred targets and diseases that can be applied to
forest healing programs [52], the suitability was reported in the following order: moderate
respiratory, endocrine, nutritional and metabolic, cardiovascular, and digestive diseases.
Specifically, asthma, diabetes, obesity, high blood pressure, hyperlipidemia, myocardial
infarction, and indigestion were identified as the target diseases. Expectations for forest
healing effects and urban forest utilization can be promoted in daily life through efforts to
clearly distinguish whether it is a competitive or complementary approach to the existing
treatment methods.
In our study, about 81.6% participants responded that they would participate in the
urban forest healing program for disease and considering the cost that these respondents
were willing to pay for the program as per the results of the survey, it would be quite
valuable to develop and publicize these healing programs. Correspondingly, the Korean
government is actively making efforts to provide forest healing effects within living areas.
At this point, it is very encouraging that awareness of the healing effect of urban forests is
positive. Therefore, efforts will be needed to clearly present the effectiveness of forest heal-
ing programs by developing individualized healing programs for patients and expanding
these to urban forests that are easily accessible in daily life.
To the best of our knowledge, this is the first study to investigate the expected values,
needs, and preferred components of urban forest healing programs in urban forest visitors
with diseases. However, the limitations of this study must also be acknowledged. First,
the study was at risk of selection bias, as only those interested in the topic would have
participated in the survey. Further research should use probability sampling methods to
reduce this selection bias. Second, this pilot survey included only urban forest visitors with
diseases; therefore, it is difficult to confirm whether our results were due to the presence
or absence of diseases. Therefore, further studies are warranted to compare urban forest
visitors with and without diseases to obtain meticulous results. In addition, the sample size
of each disease was unequal so that type I error levels may not be guaranteed. Therefore,
further research should include equal sample sizes considering age distribution for each
disease to find out the difference depending on the type of disease and see their relationship
to the degree of awareness or preference of urban forest healing effects, due to various
clinical and pathological characteristics of these diseases. Future studies should focus on
the detailed clinical characteristics of visitors to improve or develop customized urban
forest healing programs for people with various types of diseases.

Int. J. Environ. Res. Public Health 2022, 19, 513
12 of 14
5. Conclusions
About 82% of urban forest visitors with disease agreed on the need for urban forest
healing programs and wanted to participate in these programs. The results of the present
survey showed that the purpose of the urban forest visits and expected values of urban
forest healing were mostly not different for each disease and although people with diseases
had relatively lower awareness and expected values of urban forest healing effects on
physical health, the demand for these programs was still high.
Urban forest therapy programs should be developed based on the medical characteris-
tics of the individual disease to maximize the effectiveness of the program. Additionally,
policies should be made to inform general population that urban forest healing is beneficial
not only for mental health but also for physical health. Moreover, our results can be used
as basic data for the development of such programs for people with diseases.
Funding: This research was supported by ‘R&D’ program for Forest Science Technology (Project No.
2021393A00-2123-0103) provided by Korea Forest Service (Korea Forestry Promotion Institute).
Institutional Review Board Statement: The study was conducted according to the guidelines of
the Declaration of Helsinki and approved by the Gachon University Institutional Review Board
(1044396-202106-HR-136-01).
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: The datasets generated during this study are available from the corre-
sponding author upon reasonable request.
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Park, S.; Kim, S.; Kim, G.; Choi, Y.; Kim, E.; Paek, D. Evidence-Based Status of Forest Healing Program in South Korea. Int. J.
Environ. Res. Public Health 2021, 18, 10368. [CrossRef]
2. Jeong, D.-Y.; Choi, Y.-E.; Chon, J.-H. Analysis of Importance in Available Space for Creating Urban Forests to Reduce Particulate
Matter—Using the Analytic Hierarchy Process. J. Korean Inst. Landsc. Archit. 2019, 47, 103–114. [CrossRef]
3. Oku, H.; Fukamachi, K. The differences in scenic perception of forest visitors through their attributes and recreational activity.
Landsc. Urban Plan. 2006, 75, 34–42. [CrossRef]
4. Blazevska, A.; Miceva, K.; Stojanova, B.; Stojanovska, M. Perception of the Local Population toward Urban Forests in Municipality
of Aerodrom. South-East Eur. For. 2012, 3, 87–96. [CrossRef]
5. Nam, E.K.; Lee, S.K.; Research, H. The influences of the tourism motivation on the perceived value and satisfaction of healing
forest visitor. Int. J. Tour. Hosp. Res. 2015, 29, 79–93.
6. Lee, Y. An Outlook for Social Changes in an Aged Korea: Implications from the Japanese Case Health and welfare policy forum.
Health Welf. Policy Forum 2017, 254, 9–17.
7. Deneke, F. Urban Forestry in North America: Towards a Global Ecosystem Perspective. In Proceedings of the First Canadian
Urban Forests Conference, Winnipeg, MB, Canada, 30 May–2 June 1993.
8. Levine, S.; Malone, E.; Lekiachvili, A.; Briss, P. Health Care Industry Insights: Why the Use of Preventive Services Is Still Low.
Prev. Chronic Dis. 2019, 16, E30. [CrossRef]
9. Chae, Y.-R.; Kang, S.-Y.; Jo, Y.-M.; Lee, S.-H.; Park, S.-Y.; Cheon, I.-S. An Analysis of Needs and Preferences of Forest Healing
Programs in patients with Chronic Diseases. J. Korean Soc. Rural. Plan. 2021, 27, 29–41.
10. Lee, J.-H.; Burger-Arndt, R.J. Understanding the healing function of urban forests in German cities. J. Korean Inst. For. Recreat.
2011, 15, 81–89.
11. Lee, H.J.; Son, Y.-H.; Kim, S.; Lee, D.K. Healing experiences of middle-aged women through an urban forest therapy program.
Urban For. Urban Green. 2019, 38, 383–391. [CrossRef]
12. Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological
and Psychological Effects of Forest Therapy on Middle-Aged Males with High-Normal Blood Pressure. Int. J. Environ. Res. Public
Health 2015, 12, 2532–2542. [CrossRef] [PubMed]
13. Mao, G.-X.; Cao, Y.-B.; Lan, X.-G.; He, Z.-H.; Chen, Z.-M.; Wang, Y.-Z.; Hu, X.-L.; Lv, Y.-D.; Wang, G.-F.; Yan, J. Therapeutic effect
of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [CrossRef] [PubMed]
14. Vujcic, M.; Tomicevic-Dubljevic, J. Urban forest benefits to the younger population: The case study of the city of Belgrade, Serbia.
For. Policy Econ. 2018, 96, 54–62. [CrossRef]
15. Yu, C.-P.; Lin, C.-M.; Tsai, M.-J.; Tsai, Y.-C.; Chen, C.-Y. Effects of Short Forest Bathing Program on Autonomic Nervous System
Activity and Mood States in Middle-Aged and Elderly Individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [CrossRef]

Int. J. Environ. Res. Public Health 2022, 19, 513
13 of 14
16. Lanki, T.; Siponen, T.; Ojala, A.; Korpela, K.; Pennanen, A.; Tiittanen, P.; Tsunetsugu, Y.; Kagawa, T.; Tyrväinen, L. Acute effects of
visits to urban green environments on cardiovascular physiology in women: A field experiment. Environ. Res. 2017, 159, 176–185.
[CrossRef]
17. Han, I.D.; Koo, C.-D. The Effect of Forest Healing Program on the Resilience of Elderly People in Urban Forest. J. People Plants
Environ. 2018, 21, 293–303. [CrossRef]
18. Service, K.F. Urban Forest Policy Report; Korea Forest Service: Daejeon, Korean, 2007.
19. Kim, D.-S.; Lee, B.-C.; Park, K.-H. Determination of Motivating Factors of Urban Forest Visitors through Latent Dirichlet Allocation
Topic Modeling. Int. J. Environ. Res. Public Health 2021, 18, 9649. [CrossRef]
20. Kim, S.Y.; Kim, B.H.S. The Effect of Urban Green Infrastructure on Disaster Mitigation in Korea. Sustainability 2017, 9, 1026.
[CrossRef]
21. Lee, H.J.; Son, S. Qualitative assessment of experience on urban forest therapy program for preventing dementia of the elderly
living alone in low-income class. J. People Plants Environ. 2018, 21, 565–574. [CrossRef]
22. Yu, C.-P.S.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban For. Urban Green.
2020, 51, 126670. [CrossRef]
23. Byun, H.-J.; Lee, B.-C.; Kim, D.; Park, K.-H. Market Segmentation by Motivations of Urban Forest Users and Differences in
Perceived Effects. Int. J. Environ. Res. Public Health 2021, 19, 114. [CrossRef]
24. Kim, S.-Y. The effect of choice attribute of forest healing culture affects user expectation value and satisfaction. Cult. Exch.
Multicult. Educ. 2016, 5, 5–29.
25. Deng, J.; Arano, K.G.; Pierskalla, C.; McNeel, J. Linking Urban Forests and Urban Tourism: A Case of Savannah, Georgia. Tour.
Anal. 2010, 15, 167–181. [CrossRef]
26. Poe, M.R.; McLain, R.J.; Emery, M.; Hurley, P.T. Urban Forest Justice and the Rights to Wild Foods, Medicines, and Materials in
the City. Hum. Ecol. 2013, 41, 409–422. [CrossRef]
27. Kim, J.Y.; Shin, C.S.; Lee, J.K. The effects of forest healing program on mental health and melatonin of the elderly in the urban
forest. J. People Plants Environ. 2017, 20, 95–106. [CrossRef]
28. Flouri, E.; Midouhas, E.; Joshi, H. The role of urban neighbourhood green space in children’s emotional and behavioural resilience.
J. Environ. Psychol. 2014, 40, 179–186. [CrossRef]
29. Kardan, O.; Gozdyra, P.; Misic, B.; Moola, F.; Palmer, L.; Paus, T.; Berman, M.G. Neighborhood greenspace and health in a large
urban center. Sci. Rep. 2015, 5, 11610. [CrossRef]
30. Ulmer, J.M.; Wolf, K.L.; Backman, D.R.; Tretheway, R.L.; Blain, C.J.; O’Neil-Dunne, J.P.; Frank, L.D. Multiple health benefits of
urban tree canopy: The mounting evidence for a green prescription. Health Place 2016, 42, 54–62. [CrossRef]
31. Lee, K.J.; Hur, J.; Yang, K.-S.; Lee, M.-K.; Lee, S.-J. Acute Biophysical Responses and Psychological Effects of Different Types of
Forests in Patients with Metabolic Syndrome. Environ. Behav. 2018, 50, 298–323. [CrossRef]
32. Chun, M.H.; Chang, M.C.; Lee, S.-J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J.
Neurosci. 2017, 127, 199–203. [CrossRef]
33. Jia, B.B.; Yang, Z.X.; Mao, G.X.; Lyu, Y.D.; Wen, X.L.; Xu, W.H.; Lyu, X.L.; Cao, Y.B.; Wang, G.F. Health Effect of Forest Bathing Trip
on Elderly Patients with Chronic Obstructive Pulmonary Diseas. Biomed. Environ. Sci. 2016, 29, 212–218. [CrossRef]
34. Mao, G.; Cao, Y.; Wang, B.; Wang, S.; Chen, Z.; Wang, J.; Xing, W.; Ren, X.; Lv, X.; Dong, J.; et al. The Salutary Influence of Forest
Bathing on Elderly Patients with Chronic Heart Failure. Int. J. Environ. Res. Public Health 2017, 14, 368. [CrossRef] [PubMed]
35. Kang, H.; Chae, Y.; Health, P. Effects of Integrated Indirect Forest Experience on Emotion, Fatigue, Stress and Immune Function
in Hemodialysis Patients. Environ. Res. Public Health 2021, 18, 1701. [CrossRef] [PubMed]
36. Nakau, M.; Imanishi, J.; Imanishi, J.; Watanabe, S.; Imanishi, A.; Baba, T.; Hirai, K.; Ito, T.; Chiba, W.; Morimoto, Y. Spiritual Care
of Cancer Patients by Integrated Medicine in Urban Green Space: A Pilot Study. Explore 2013, 9, 87–90. [CrossRef] [PubMed]
37. Li, Q.; Morimoto, K.; Nakadai, A.; Inagaki, H.; Katsumata, M.; Shimizu, T.; Hirata, Y.; Hirata, K.; Suzuki, H.; Miyazaki, Y.; et al.
Forest Bathing Enhances Human Natural Killer Activity and Expression of Anti-Cancer Proteins. Int. J. Immunopathol. Pharmacol.
2007, 20, 3–8. [CrossRef]
38. Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.; Wakayama, Y.; et al.
Visiting a Forest, but Not a City, Increases Human Natural Killer Activity and Expression of Anti-Cancer Proteins. Int. J.
Immunopathol. Pharmacol. 2008, 21, 117–127. [CrossRef]
39. Kim, B.J.; Jeong, H.; Park, S.; Lee, S. Forest adjuvant anti-cancer therapy to enhance natural cytotoxicity in urban women with
breast cancer: A preliminary prospective interventional study. Eur. J. Integr. Med. 2015, 7, 474–478. [CrossRef]
40. Kim, H.; Lee, Y.W.; Ju, H.J.; Jang, B.J.; Kim, Y.I. An Exploratory Study on the Effects of Forest Therapy on Sleep Quality in Patients
with Gastrointestinal Tract Cancers. Int. J. Environ. Res. Public Health 2019, 16, 2449. [CrossRef]
41. Chang, Y.-C.; Tseng, T.A.; Chiu, S.-C. The effect of nature therapy for stress, anxiety, depression and demoralization on breast
cancer patients. GSTF J. Nurs. Health Care 2018, 5.
42. Lee, I.; Choi, H.; Bang, K.-S.; Kim, S.; Song, M.; Lee, B. Effects of Forest Therapy on Depressive Symptoms among Adults: A
Systematic Review. Int. J. Environ. Res. Public Health 2017, 14, 321. [CrossRef]
43. Melnyk, B.M.; Gallagher-Ford, L.; Long, L.E.; Fineout-Overholt, E. The Establishment of Evidence-Based Practice Competencies
for Practicing Registered Nurses and Advanced Practice Nurses in Real-World Clinical Settings: Proficiencies to Improve
Healthcare Quality, Reliability, Patient Outcomes, and Costs. Worldviews Evid.-Based Nurs. 2014, 11, 5–15. [CrossRef]

Int. J. Environ. Res. Public Health 2022, 19, 513
14 of 14
44. Suk-Hyeon Park, C.-D.K. Needs Analysis for the Development of Forest Therapy Program Utilizing the Urban Forest-Focused on
the Visitors of Incheon Grand Park. J. Korean Inst. For. Recreat. 2018, 22, 11–24.
45. Kim, Y.-H.J.; Joung, D.; Park, B.J. A Study on Analyze Contents of Forest based Therapeutic Programs in Korea. Korean Inst. For.
Recreat. Welf. 2019, 23, 43–58.
46. Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The Psychological and Physical Effects of Forests
on Human Health: A Systematic Review of Systematic Reviews and Meta-Analyses. Int. J. Environ. Res. Public Health 2021,
18, 1770. [CrossRef] [PubMed]
47. Ruiz, I.F. Immune system and cardiovascular disease. Nat. Rev. Cardiol. 2016, 13, 503. [CrossRef] [PubMed]
48. Report on ‘Three National Parks in the City, Including Bukhansan Mountain, Have Increased the Number of Visitors; Korea National Park
Service: Wonju, Korea, 2020.
49. Kim, Y.-H.; Kim, E.-J.; Kim, D.-J.; Yeoun, P.-S.; Choi, B.-J. The preference analysis of adults on the forest therapy program with
regard to demographic characteristics. J. Korean Soc. For. Sci. 2015, 104, 150–161. [CrossRef]
50. Kim, Y.-H.; Kim, D.; Yeoun, P.; Choi, B.J. The analysis of interests and needs for the development of forest therapy program in
adults. J. Korean Inst. For. Recreat. 2014, 18, 45–59.
51. Kim, G.-H.; Lee, S.-G. An analysis of user perception regarding trail related cafes and blogs using big data collected over 10 years.
J. Hosp. Tour. Stud. 2021, 23, 34–52. [CrossRef]
52. Park, S.; Woo, J.; Kim, W.; Lee, Y.J. Sub-populations and disorders that can be applied to forest therapy. J. Korean Inst. For. Recreat.
2012, 16, 35–42.