

Encountering the Sacred Temenos:
Somatically Integrating Cumulative Trauma and Discovering Wellbeing Within
by
Chelsea Phillips
Submitted in partial fulfillment of the requirements
for the degree of
Master of Arts in Counseling Psychology
Pacifica Graduate Institute
27 February 2017

ProQuest Number: 10259259
All rights reserved
INFORMATION TO ALL USERS
The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscript
and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
ProQuest 10259259
Published by ProQuest LLC (2017). Copyright of the Dissertation is held by the Author.
All rights reserved.
This work is protected against unauthorized copying under Title 17, United States Code
Microform Edition © ProQuest LLC.
ProQuest LLC.
789 East Eisenhower Parkway
P.O. Box 1346
Ann Arbor, MI 48106 - 1346

ii
© 2017 Chelsea Phillips
All rights reserved

iii
I certify that I have read this paper and that in my opinion it conforms to acceptable
standards of scholarly presentation and is fully adequate, in scope and quality, as a
product for the degree of Master of Arts in Counseling Psychology.
____________________________________
Avrom Altman, M.A., L.M.F.T., L.P.C.
Portfolio Thesis Advisor
On behalf of the thesis committee, I accept this paper as partial fulfillment of the
requirements for Master of Arts in Counseling Psychology.
____________________________________
Avrom Altman, M.A., L.M.F.T., L.P.C.
Research Associate
On behalf of the Counseling Psychology program, I accept this paper as partial
fulfillment of the requirements for Master of Arts in Counseling Psychology.
____________________________________
Jemma Elliot, M.A., L.M.F.T., L.P.C.C.
Director of Research

iv
Abstract
Encountering the Sacred Temenos:
Somatically Integrating Cumulative Trauma and Discovering Wellbeing Within
by Chelsea Phillips
This paper explores trauma as a continuum and how various forms of trauma can be
treated with mindfulness and somatic psychotherapy modalities. Ten modalities are
discussed through hermeneutic, heuristic, and intuitive inquiry research methods: mindful
breathing; mindfulness-based stress reduction (MBSR); emotional freedom techniques
(EFT) and energy psychology; eye movement desensitization and reprocessing (EMDR)
and attachment focused EMDR; Hakomi mindfulness-centered psychotherapy;
sensorimotor psychotherapy; somatic experiencing; acupuncture, Soma Neuromuscular
Integration® bodywork, and authentic movement. Unique to this thesis is the approach to
somatically releasing trauma using an acronym framework created by the author,
conceptualized as Safety, Trust, Acceptance, Belonging, Love, Earth, and Ecopsychology
(STABLE©). Adding a depth psychotherapy perspective, the myth of Inanna is offered as
an allegory to enrich the practice of co-regulating patients as they work through their
trauma narratives. Recognizing nature as an essential component to healing the wounds
of the soul adds an ecopsychological and wilderness therapy perspective.

v
Acknowledgments
I would like to offer my gratitude to the people who most profoundly influenced
me in the creation of this thesis. First and foremost, I thank my daughter Lyra Phillips,
who teaches me daily how to deepen my practice of attunement to the needs of another
and who has patiently supported me through the completion of pursuing my life dream to
become a depth and ecopsychology oriented marriage and family therapist and
wilderness therapy facilitator. My gratitude extends deeply to my ancestors and to both of
my parents, MarySue Brooks and Raymond Phillips, who have gifted me with awe
inspiring amounts of acceptance and love, secure attachment, and belief in me in all
ways. You have both taught me how to love more and to welcome adversity with grace.
To my amazing siblings Amy, Heather, and Cameron, and to our entire family—thank
you for your love, support, humor, and the closeness we share. I am blessed to be a part
of an amazing community of friends who continually inspire me, offering warmth and
support from Salt Spring Island, British Columbia to Prescott, Arizona, to Seattle,
Washington to the far reaches of my travels—you know who you are; I thank you with so
much love. To my Pacifica cohort—you have become friends and colleagues for life!
To the educators who have influenced me most throughout my lifetime for gifting
me with an enthusiasm for life and learning, calling out my wisdom, allowing the poetess
within me to be expressed, teaching me about my shortcomings, and expanding my
curiosity: Marcia Larson—you gave me my Montessori, self-directed learning beginning
and celebrated my creative and caring soul. Mary O’Malley—you inspired me to become

vi
a spiritual retreat facilitator and to be a therapist who welcomes my clients back to the
home of their being. Ellen Abell—I instantly wanted to be like you! Your wise clarity,
feminist strength, and confident ease were qualities in myself I grew into as you
mentored and believed in me. Lilla Cabot—you taught me how to question the status quo
from a feminist perspective and encouraged me that in my gentleness there is great
strength. Wayne Regina—you gave me an outstanding education in marriage, family, and
couples therapy from a family systems orientation. Jo Beth Eckerman, Karen Bolesky,
and Marcia Nolte—you gave me the tools and training to facilitate energy and somatic
healing, as well as authentic movement at a core level. To the teachers who nurtured me
as a writer and poet—Carmen Roedell, Carol Erickson, Leanne Lukas, Carmine
Chickadel, and Michael Nipert. To Larry Buell, Dave Craig, Denise Mitten, Erin Lotz,
Julie Munro, Roxane Ronca, Claire Oberst, Fiona Reid, J. Dianne Brederson, Bob Ellis,
Mark Riegner, Tom Fleishner, Laura Sewall, Steve Munsell, David Lovejoy, and Doug
Hulmes—phenomenal experiential and adventure educators who initiated me in
necessary rites of passage to become a wilderness therapy facilitator.
To my mentors at Pacifica Graduate Institute: your depth and caring, combined
with your finesse in the art of therapy fostered the confidence and competence in me to
step into the world as a ecopsychology and depth focused marriage and family
therapist—Marilyn Owen, Avrom Altman, Michelle Villegas, Sukey Fontelieu, Willow
Young, Kathee Miller, Barbara Boyd, Allen Koehn, Nicole Zapata-Williams, Matthew
Bennett, and Christine Downing.
Special thanks to Kim Sather—supervisor, mentor, and friend and to the entire
staff at my counseling internship site. Thank you to the therapists I have worked with
vii
throughout my life journey. To Kathleen Lumiere, Alda Blanes, Kim Hansen, Jared
Kohler, and Wolfgang Brolley—five of the finest somatic healers I have encountered and
benefited from their skills. To my past, present, and future clients I give my utmost
gratitude.
Finally, I give thanks to my intuitive heart and my soul essence, guiding me every
step of the way on the wild, reflective, and wondrous path that is my life.
Nature & Psyche in Bliss
Calf Creek Falls, Utah
Photograph of Chelsea Phillips by Lauren Brule (2013)
Reprinted with permission.

viii
Dedication
This thesis is dedicated to the poetic moments in our lives that thrill our hearts
and warm our souls and it is also dedicated to working with what gets in the way of being
able to feel such moments. To the beauty of the microcosmic and macrocosmic Earth:
with its innumerable and miraculous permutations of life loving life into creation and
ever-unfolding transformation—the ultimate teacher in the cycles of birth and death and
rebirth. May Safety, Trust, Acceptance, Belonging, Love, and connection with Earth
become allies in the process of somatically releasing and integrating cumulative trauma.
And may the qualities of inclusivity, playfulness, empathic attunement, kindness, and
peace be a part of the journey into wellbeing within.
Blooming into Being
Prince Rupert, British Columbia
Photograph by Chelsea Phillips (2015)

ix
Table of Contents
Chapter I Introduction..................................................................................................1
Area of Interest ........................................................................................................1
Guiding Purpose.......................................................................................................3
Rationale ..................................................................................................................4
Methodology ............................................................................................................5
Research Problem ........................................................................................6
Research Question .......................................................................................7
Ethical Concerns ......................................................................................................7
Overview of Thesis ..................................................................................................7
Chapter II Literature Review.........................................................................................9
Introduction ..............................................................................................................9
Trauma Has Many Forms: Differentiations and Definitions .................................10
Trauma Symptoms: How They Show Up Clinically .............................................11
Emotional Regulation, Affect Regulation, and Self-Regulation ...........................12
Polyvagal Theory ...................................................................................................13
Window of Tolerance ............................................................................................14
Highly Sensitive People .........................................................................................15
The Importance of Integration as a Concept and Experience ................................16
Somatic Modalities Utilized in the Treatment of Trauma .....................................16
Mindfulness Breathing: One Belly Breath at a Time.................................17
Mindfulness-Based Stress Reduction ........................................................18
Acupuncture ...............................................................................................19
Energy Psychology and Emotional Freedom Technique ..........................20
Eye Movement Desensitization and Reprocessing ....................................21
Hakomi Mindfulness-Centered Psychotherapy .........................................22
Sensorimotor Psychotherapy .....................................................................24
Somatic Experiencing® .............................................................................25
Soma Neuromuscular Integration® Bodywork .........................................26
Authentic Movement .................................................................................27
Attachment and Bonding: What Love Has to Do With It......................................28
Chapter III Findings and Clinical Applications............................................................30
Encountering the Sacred Temenos.........................................................................30
Trauma as Cumulative and on a Continuum..........................................................33
Co-creating the Sacred Temenos with Patients and Clients ..................................34
STABLE©: Safety, Trust, Acceptance, Belonging, Love, Earth, and
Ecopsychology .......................................................................................................34
Nature’s Influence on the Psyche ..........................................................................37

x
Exploring the Application of Somatic Modalities .................................................39
Affect Regulation and the Introduction of Conscious Co-Regulation...................41
Shadow Integration ................................................................................................42
The Myth of Inanna as an Allegory for Processing Trauma..................................44
Discovering and Cultivating Wellbeing.................................................................47
Clinical Applications .............................................................................................49
Chapter IV Summary and Conclusions ........................................................................51
Summary ................................................................................................................51
Suggestions for Further Research ..........................................................................52
Conclusions ............................................................................................................53
Appendix A STABLE© Rainbow Drawing Used Clinically .........................................55
Appendix B Using STABLE© to Address Client Dysregulation: A Clinical Example 56
References ..........................................................................................................................59
xi
List of Illustrations
Figure 1
Nature & Psyche in Bliss .......................................................................... vii
Photograph of Chelsea Phillips by Lauren Brule, 2013
Reprinted with permission
Figure 2
Blooming into Being ................................................................................ viii
Photograph by Author, 2015
Figure 3
Gentleness Embodied ................................................................................. xi
Photograph by Author, 2015
Figure 4
STABLE© ...................................................................................................36
Drawing by Author, 2017
Figure 5
Rainbow Drawing of STABLE© ................................................................54
Drawing by Author, 2017
Gentleness Embodied
Carpinteria, California
Photograph by Chelsea Phillips (2015)

Chapter I
Introduction
Area of Interest
My fascination with the subject of the release and integration of somatically
stored cumulative trauma comes from both professional and lived experience. This thesis
is based on the conjecture that all people experience various forms of trauma from micro
to macro. In order to orient the reader to the perspectives on trauma presented in this
thesis, sharing some of my history with discovering trauma work is relevant. Twenty
years ago, I was walking along a low bank waterfront trail on Salt Spring Island, British
Columbia when I had a vision of me sitting there in a circle of stones with a group of
people, cofacilitating a workshop blending bodywork, therapy, and attunement with
nature. In my vision, the circle of stones was a sacred demarcation, a safe container, a
temenos. There was some numinous connection between addressing healing the body and
healing psyche in nature that I intuitively felt was how I wanted to dedicate my life’s
work with others. I also desperately needed what this triune had to offer; I felt it in my
bones.
To pursue this dream, I discovered the field of ecopsychology and was also
introduced to the bodywork modality of Soma Neuromuscular Integration® (Bolesky,
2017). I set out to train as an ecotherapist and bodywork practitioner. As a bodywork
practitioner, I learned that tension and trauma are stored in the connective tissue and that
often my clients experienced eruptions of tears and memories, and released not just
present time tightness but years of stored trauma.

2
Before I understood the concept of the window of tolerance for emotional arousal,
I experienced being outside the window of my tolerance due to the intensity of new skill
acquisition backpacking in the wilderness of Arizona, river rafting in the Canyonlands,
and sea kayaking in the Sea of Cortez (Siegel, 2012; discussed in Chapter II). Years of
cumulatively accrued trauma came up for me during my adventure education training at
Prescott College in the form of overwhelm, overstimulation, fear, panic, a lack of
confidence, clumsiness, and at times being more dysregulated. My threshold for
disequilibrium seemed to be lower than for other students, although some students also
experienced disequilibrium. What made some of us more vulnerable to overwhelm than
others? I self-identify as a highly sensitive person (HSP) and this correlates to having a
nervous system that is more hypervigilant at times and more easily aroused by stimulus,
especially when there is a perceived threat to survival (Aron 1996, 2010; discussed in
Chapter II). Having experienced past trauma increases the sense of perceived threats
(Levine, 2010; van der Kolk, 2014).
A part of me was calling out for help in the only language it had—through the
body and psyche rather than the articulate mind. As I was studying to become a therapist,
I felt that there was a way to facilitate exhilarating backcountry trips that would be more
responsive to sensitively wired participants like me. My soul was calling for a pace that
would support my nervous system to experience cortical calm and integration in the
wilderness adventures being led. In reflecting on my experiences, I recognized that I
needed the pace of skill acquisition to slow down to make room for my internal process
to reveal itself. This realization influenced how I intend to facilitate therapeutic
experiences in nature.

3
When I encountered psychologist Pat Ogden’s (Ogden, Kekuni, & Pain, 2006;
Ogden & Fisher, 2015) sensorimotor psychotherapy something clicked. Ogden and her
colleagues were keenly aware of the need to slow experiences in therapy when a place of
trauma or dysregulation was touched. I could see that in adventure education slowing
down processes and offering choices when it comes to tasks involving physical risks may
help to bring equilibrium to the sympathetic and parasympathetic nervous system, which
may lead, as discussed in Chapter II, to increased skill acquisition, integration, ease, and
enjoyment of experiences. The more I work with clients from young children to adults,
the more I see the need to slow the pace of experience and allow empathic attunement to
take place, as this is where transformation from stored trauma into resilient wellbeing
occurs.
Guiding Purpose
When I set out to explore the topic of how to release and resolve trauma
emotionally, mentally, and somatically, I approached each topic individually, unaware of
the vast amount of research being done on the interrelatedness of attachment processes,
mind, body, and emotion in healing trauma. It was gratifying to me that the research
literature was supporting my intuition that these elements are crucially connected in
trauma, its release, and the creation of wellbeing—including issues of emotional
deregulation and unresolved trauma (Epstein, 2013; Johnson, 2013; Kabat-Zinn, 2013;
Kurtz, 1990; Ogden & Fisher, 2015; Parnell, 2013; Siegel, 2012; Shapiro & Forrest,
2016; van der Kolk, 2014; Weiss, Johanson, & Monda, 2015). This discovery spurred me
on to write this thesis. I set out to explore what somatic modalities seem most effective
for what kinds of trauma and what core needs long to be met beneath the defensive scabs

4
of trauma wounds. This research serves the underlying goals of therapy to help clients
release cumulative trauma, integrate past experiences to create cohesive narratives out of
their life histories, foster more effective emotional self-regulation, and increase their
sense of wellbeing and resilience in the present moment. It is my hope that readers from
professional fields that serve people’s psychological and physical wellbeing and those
with a curious mind will gain useful insights and be motivated to further explore the
approaches to treating cumulative trauma I reference in this thesis.
My hope in crafting this thesis was to envelop this synthesis of research in a depth
psychology approach with the use of language as a healing balm—to craft my thesis in
such a way that the reader has an experience of cortical calm, while reading my work. I
hoped to allow the experience of writing my thesis to be personally healing and grow me
into a better, more informed therapist. My hope is that the same kind of process happens
for my readers—where they feel acknowledged in their micro and cumulative trauma
experiences. I hope to convey to readers the uplifting idea that wellbeing is a state one
can return to again and again throughout life and within a single day.
Rationale
Trauma does not affect some people; it impacts all people (Epstein, 2013). Thus,
seeing trauma on a continuum may be helpful—from micro to macro. All people begin as
infants—vulnerable and without adequate defenses against innumerable forms of
stimulus. Some stimuli are pleasant and welcome, opening the infant further to seek more
of what feels good. Other forms of stimuli create micro trauma responses of contraction,
retraction, fear, and uncertainty. Macro trauma is inclusive of singular or repeated
incidents such as war, domestic violence, sexual abuse, rape, severe car accidents, and

5
other threats to one’s existence (Herman, 1997; van der Kolk, 2014). Developmental
trauma—that which negatively effects psychological growth during childhood—can
impact a person for the duration of his or her life. Cumulative trauma describes the
accrual of unprocessed experiences of traumatizing events. The extent to which stimuli is
trauma inducing depends on the individual’s unique set of genetic, in-utero, postnatal,
and developmental nurturance and circumstances that contribute to both cumulative
trauma and resilience. Given that every person encounters negative experiences, some of
which result in trauma responses, exploring how to release trauma from psyche and body
to move forward in life in a balanced and emotionally regulated way seems important to
practitioners, patients, and family members worldwide.
Methodology
The research and writing process in this thesis became a blend of hermeneutic,
heuristic, and intuitive inquiry approaches (Coppin & Nelson, 2005, pp. 28-33, 133).
“Hermeneutic analysis is required in order to derive a correct understanding of a text. . .
Interrelationship of science, art, and history is at the heart of hermeneutic design and
methodology” (Moustakas, 1994, p. 9). Having experienced various forms of trauma in
my life, the healing process I have undergone has become a guide in service to my
research. However, my personal journey is not the central focus of this thesis. In this
way, the heuristic aura informed how I went about writing this thesis from lived events
blended with research supporting my conjectures (Dane, 2011, pp. 44-45).
Throughout this writing process, I have released trauma from my tissues through
various forms of bodywork in conjunction with therapy, meditation, and time in nature.
In this way, I underwent an experience of intuitive inquiry: The health practitioners who

6
assisted me in healing served as a panel to reflect what they observed in me during my
process with them (Coppin & Nelson, 2005, pp. 32-33). Phenomenologically, I
somatically released trauma in conjunction with psychotherapy, and thus I became a
living example of my thesis research, as my therapy clients also did (Creswell, 2009, p.
13). The documentation of this process may be helpful for others to explore their personal
and professional encounters with releasing and integrating trauma.
Research problem. I believe that greater exploration of the relationships between
highly sensitive individuals, trauma somatization in the body, attachment and bonding,
self-regulation, and the holistic treatment of cumulative trauma from a depth perspective
would be beneficial to a large populous. It seems that as a result of the existing research
into this subject trauma and attachment have become buzz words, but this only highlights
the importance of continuing to add a depth psychotherapy voice to the dialogue.
The very pace of life can cause cumulative micro traumas: speeding down the
freeway; being inundated by electronic media; lacking time to go outside and be breathed
by the trees; global warming; increasing economic stress, debt, and homelessness; and
feeling isolated in a world where its human population is growing while other species are
racing toward extinction all contribute to cumulative trauma (Wilson, 2016). All these
micro traumas tend to be somatized in the body as it continually seeks homeostasis.
Highly sensitive individuals are most likely to have and be aware of a traumatogenic
psychological and somatic reaction to these life experiences. Creating strong
interpersonal bonds and secure attachments can be a healing balm to the growing
epidemic of isolation and support resilience and the healing of trauma. I aimed to explore
and synthesize research on trauma as a continuum inclusive of micro traumas and its

7
treatment through 10 different modalities, weaving the research into a depth psychology
approach.
Research question. Acknowledging the postulation that every person has somatic
experiences of trauma, this thesis asks: What methods are effective in the relief of trauma
symptoms, and in what ways does creating a sacred temenos, a safe container, in
therapeutic settings help to release and integrate trauma and then lead to greater
wellbeing?
Ethical Concerns
The primary ethical concern of this thesis is the potential for the author or a reader
to reexperience traumatic memories or to become activated by the material focusing on
somatized trauma. It is important that both the author and the reader be aware of personal
limitations and consult with a therapist or other natural supports if activation or
retraumatization occurs while writing or reading this material. In discussing work with
clients or patients, I used generalities of experience, amalgamating various clients’
experiences. To protect the privacy of my patients I did not use names or specific details
which could lead to any form of personal identification.
Overview of Thesis
The title of this thesis is a primer to the entire work in that each key word has at
least one interrelated section that explores its relevance. Chapter II deepens the
discussion with an overview of the key topics to understand when exploring somatically
stored trauma: differences between forms of trauma, the clinical appearance of trauma
symptoms, emotional regulation, polyvagal theory, the window of tolerance, highly
sensitive people (HSPs), and the integration of somatic content. The second portion of the

8
literature review adds perspectives from essential founders and practitioners of 10
somatic modalities that treat trauma: mindful breathing, mindfulness-based stress
Reduction (MBSR), acupuncture, Emotional Freedom Technique (EFT) and energy
psychology, eye movement desensitization and reprocessing (EMDR) and attachment
focused EMDR (AF-EMDR), Hakomi Mindfulness-Centered Psychotherapy,
Sensorimotor Psychotherapy, Somatic Experiencing®, Soma Neuromuscular
Integration® bodywork, and Authentic Movement. The final section of Chapter II
discusses the essential aspects of attachment theory and bonding that highlight the
importance to wellbeing of the affiliative nature of humanness.
Chapter III opens the reader into the lens from which I do trauma work, inclusive
of Safety, Trust, Acceptance, Belonging, Love, Earth, and Ecopsychology (STABLE©),
an acronym and method conceptualized by the author. This way of working with clients
leads into a discussion of the process of making trauma work effective and how I have
observed integration and release of cumulative trauma to unfold. A depth psychological
view of integrating unconscious memories and affect is presented that draws on the myth
of Inanna (Perera, 1981) as an allegory for movement from the dysregulation of trauma to
a state of a greater wholeness. Chapter III also discusses the clinical applicability of
working with somatic modalities in the treatment of trauma symptoms. Chapter IV
provides a summary of thesis topics and suggestions for further research. The conclusion
offers final reflections and a synthesis of how therapists, facilitators, and health
professionals can incorporate the concepts offered in this thesis into their professional
practices.

Chapter II
Literature Review
Introduction
There are already multitudes of modalities and techniques to somatically address
trauma symptoms. Founder and director of the Trauma Center in Brookline,
Massachusetts, Bessel van der Kolk (2014) made the bold statement, “We are on the
verge of becoming a trauma-conscious society” (p. 349). What is exciting about van der
Kolk’s assertion is that although trauma is not considered something to look forward to
encountering, when the global populous can recognize trauma affects everyone, then the
impact trauma has on individuals and society at large can begin to transform at every
level.
There is an opportunity to recognize that physical and emotional pain affect
everyone and can show up invisibly or dramatically, and it does not make people who
name their experiences weaker or less effective. This is true unless they become
categorized as such by some internal or external source. Being categorized as weaker of
body or mind and as less than others occurred for soldiers after coming home from World
War I, World War II, The Korean War, and the Vietnam War when they experienced
symptoms of trauma from war (Levine, 2010, pp. 32-33). This history is where the
diagnosis for posttraumatic stress disorder (PTSD) originated (American Psychiatric
Association [APA], 2013; Levine, 2010). Changing the perspective that someone is less
valuable when they need time to heal and reintegrate from stressful or traumatic

10
experiences seems to be unfolding. In this way a new paradigm of greater empathic
attunement and compassion may be on the horizon globally.
Trauma Has Many Forms: Differentiations and Definitions
Most people from adolescence into adulthood in Western culture have been
introduced to the concept of PTSD. The American Psychiatric Association (2013)
described PTSD to include directly experiencing, witnessing, or learning about traumatic
events occurring with close family members resulting in the expression of intrusive
symptoms and avoidance behaviors (p. 271). Van der Kolk (2011) recognized,
When post-traumatic stress disorder (PTSD) first made it into the diagnostic
manuals, we only focused on dramatic incidents like rapes, assaults, or accidents
to explain the origins of the emotional breakdowns in our patients. Gradually, we
came to understand that the most severe dysregulation occurred in people, who, as
children, lacked a consistent caregiver. Emotional abuse, loss of caregivers,
inconsistency, and chronic misattunement showed up as principal contributors to
a large variety of psychiatric problems. (pp. xi-xii)
The topic of trauma as a focus in medicine, therapy, and somatic healing
modalities is not new, yet there seem to be pervasive misconceptions around what is
considered traumatic or what can be legitimately called trauma (van der Kolk, 2016). Van
der Kolk (2011) acknowledged the shift in medicine, psychiatry, and psychology to
broaden trauma to include inherited family trauma and developmental trauma.
Developmental trauma has its own designated category and the methods to treat it can
involve more time, as often the wounding occurs over an extended phase in one’s life
(Stolorow, 2008). Founding faculty member and training and supervising analyst at the
Institute of Contemporary Psychoanalysis Robert Stolorow (2008) wrote,
Developmental trauma originates within a formative intersubjective context
whose central feature is malattunement of painful affect—a breakdown of the
child-care-giver system of mutual regulation. This leads to the child’s loss of
affect-integrating capacity and thereby to an unbearable, overwhelmed,

11
disorganized state. Painful or frightening affect becomes enduringly traumatic
when the attunement that the child needs to assist in its tolerance and integration
is profoundly absent. (p. 114)
Trauma is cumulative throughout one’s life and can be seen on a continuum.
Traumatic experiences from micro to macro occur in all realms of life—in every nation,
at every age, and at every socioeconomic level. Traumatic events occur at home, at
school, at work, while watching or reading the media, and in every setting one can
imagine.
Trauma Symptoms: How They Show Up Clinically
Observing how trauma symptoms display themselves can be obvious or more
mercurial depending on how defended a person becomes or how willing, consciously or
unconsciously, the person is to reveal their inner world to themselves and others
(McWilliams, 2011). Symptoms of depression, anxiety, shame, sleep disturbances,
holding one’s breath inadvertently, the inability to make eye contact, postural aberrations,
physical pain, dissociation or moments of vacancy, the use of substances to cope with
life’s stressors, weight loss or weight gain, fatigue, aversion to certain activities,
hypervigilance, greater tendency toward verbal conflicts, a lack of engagement with
previously enjoyed activities, difficulty maintaining relationships and friendships,
difficulty maintaining emotional equilibrium and responses when parenting, and greater
overwhelm when triggered in any number of ways can all be outer signs that someone is
experiencing overwhelm from accumulated trauma (Aron, 2010; Odgen & Fischer, 2015;
Parnell, 2013; van der Kolk, 2014). Archetypal psychotherapist and mythology scholar
Thomas Moore (1992) asserted, “Observing what the soul is doing and hearing what it is
saying is a way of going with the symptom” (p. 7).
12
Thus, seeing triggering and difficult life experiences as forms of micro, macro,
and cumulative trauma can become a lens through which to understand the potentially
incongruous or ineffective ways in which one goes about living one’s life. In this regard,
child psychologist Ross Greene (2014) shifted the common misconception from “kids do
well if they want to” to “kids do well if they can” (p. 10). The same applies to adults;
they do well if they can. From this place compassion for how others show up in the world
can grow.
Emotional Regulation, Affect Regulation, and Self-Regulation
The terms emotional regulation, affect regulation, and self-regulation seem to
point to much the same concept—the idea of being adaptive, flexible, and balanced
emotionally and using clear and effective communication when interacting with others is
the goal of all three similar terms (Levine, 2010; Siegel, 2012). Siegel (2012) addressed
the question of why self-regulation is essentially considered emotional regulation by
recognizing that emotion links all layers of functioning in the mind through an integrative
process (p. 306). The term affect, Siegel added, refers to tone of voice, facial expressions,
and bodily motions—all of which are considered social signals. Psychologist Peter
Levine (2010) highlighted, “The capacity to switch between different emotional states . . .
known as affect regulation . . . is the basis for the core sense of self. . . . Emotional
regulation, our rudder through life, comes about through embodiment” (p. 354).
Psychiatrist Michael Kerr and psychiatrist and Bowen family systems founder
Murray Bowen (1988), in their conceptualization of a family system, defined an
emotional system as that which governs human behavior by “processes that predate the
development of [a] complex cerebral cortex” (p. 28). In addition to the anatomical and

13
physiological aspects of emotional response, they found the emotional system to include
the relational system: “Much of the emotional functioning of the organism is geared to its
relationship with other organisms and with the environment” (pp. 28-29). This definition
of an emotional system alleviates the need to dichotomize and compartmentalize psychic
versus somatic causes of disease. Siegel (2012) discussed emotion as being a method the
body and mind use to organize and integrate, “attuning the whole organism to current
situational demands on the basis of past experience” (p. 267). Thus, emotions inform and
link mental, social, and biological systems that involve meaning making and memory
processes of human experience.
Polyvagal Theory
This way of understanding the emotional system seems to be a precursor to
understanding human emotional reactions as presented in the polyvagal theory of Stephen
Porges (2011,), professor of psychiatry and bioengineering and Director of the Brain
Body Center at the University of Chicago, Illinois. Polyvagal theory refers to the three
possible responses of the autonomic nervous system when presented with a perceived
threat to survival: fight, flight, or freeze. Van der Kolk (2011) summarized Porges’ theory
when he wrote “the social, myelinated vagus as the fine-tuning regulatory system that
opens up a role for the environment to foster or ameliorate stress-related physiological
states” (p. xiii). Polyvagal theory offers a model for understanding how the human
nervous system is designed to respond to and regulate with other humans, animals, and
all forms of life. Porges (2011) further explained the nervous system’s regulatory
response as being
a hierarchical regulatory stress-response system emerged in mammals that not
only relies on the well-known sympathetic-adrenal activating system and the

14
parasympathetic inhibitory vagal system, but that these systems are modified by
myelinated vagus and cranial nerves that regulate facial expression which
constitute the social engagement system. (p. xiii).
Polyvagal Theory points toward the subtlety of tone of voice and facial
expressions as giving very real cues as to how one behaves in stressful as well as ordinary
life circumstances (Porges, 2011, p. xiii). This recognition is exciting, because it
scientifically proves that by external influences such as nature, therapists, doctors, and
health practitioners can help co-regulate patients. The concepts presented in this theory
also offer the opportunity to acknowledge and apply the recognition that family members,
friends, colleagues, and any member of a person’s community contribute to positive or
negative co-regulation. This is interesting in light of family systems and group dynamics,
where a group mind can influence a person’s beliefs and subsequent actions.
Window of Tolerance
The window of tolerance, a term coined by psychiatrist Dan Siegel (2012), is
interrelated with polyvagal theory. Siegel wrote extensively on the window of tolerance
as present within everyone: “Each of us has a ‘window of tolerance’ in which various
intensities of emotional arousal can be processed without disrupting the functioning of
the system” (p. 281). The window of tolerance “is a zone of optimal arousal, not too high
and not too low, within which we can adaptively and flexibly process stimuli, including
thoughts, emotions, and physical reactions, without becoming overwhelmed or numb”
(Odgen & Fisher, 2015, p. 777). An expression of trauma symptoms often disrupts
emotional regulation—thus the zone of optimal arousal is often disturbed when trauma
occurs or when repressed trauma is triggered.

15
Highly Sensitive People
The designation of being a highly sensitive person (HSP) is a way to categorize
individuals who, as the name suggests, have heightened sensitivities to various stimuli as
compared to the global populous (Aron, 1996, 2010). This term was conceptualized by
Aron (1996, 2010) based on her observations of herself, those around her, and her
patients. When exploring one’s personal level of sensitivity or assessing the level of a
patient’s tolerance to stimulation from life events, the concept that roughly 15 to 20% of
the world’s population is thought to be made up of highly sensitive persons might be
illuminating (Aron, 1996, p. ix). This percentage is too large to list HSP as a diagnosis in
the DSM-5 but it deserves to be noted that one-fifth of the world’s population experience
stimuli more acutely than is typical (APA, 2013; Aron, 1996, p. ix). It is important to
recognize that there are introverted HSPs and extroverted HSPs. Through her research,
Aron (1996) recognized approximately 70% of HSPs lean toward social introversion,
preferring interactions with fewer people and experiencing overwhelm from crowds,
large parties, or at times strangers (p. 97). Aron noted that extroverted HSPs make up
roughly 30% of the HSP population and are less overwhelmed socially by larger numbers
of people (p. 97). However, extroverted HSPs do find other sources of arousal
overwhelming such as “a long work day or being in the city too much. When over-
aroused [extroverted HSPs] avoid socializing” (p. 98).
Often there is a misconception that only introverted people who have a low
window of tolerance for overstimulation are HSPs. That is not the case. People with
attention-deficit disorder (ADD) or attention hyperactive-deficit disorder (ADHD) whose
symptoms show up more externally can also be HSPs. Each client will have their own set

16
of needs in reframing their experience to come back to a place of equilibrium after
experiencing overstimulation and thus leaving their window of tolerance (Aron, 1996).
Siegel (2012) spoke to self-regulation and levels of sensitivity within the window of
tolerance when he wrote, “Each of us has a ‘threshold of response’ or the minimum
amount of stimulation needed in order to activate our appraisal systems” (p. 275). In
addition to acknowledging one’s level of sensitivity to stimuli, the presence of trauma
and attachment or relational wounds further contributes to understanding one’s threshold
of response.
The Importance of Integration as a Concept and Experience
When exploring the nature of how trauma is released from the body, integration is
an essential concept to grasp. Siegel (2013) pointed to the importance of the integration
of aspects of the self and interpersonally with others when he wrote, “Integration is the
fundamental mechanism beneath the adaptive and healthy regulation of affect, attention,
memory, and social interactions” (p. xiii). Somatic integration is a form of integration
that refers to the body assimilating change through stimuli inclusive of breath, touch, and
movement (Levine, 2010; Ogden & Fisher, 2015). Bodywork, walking, exercise in
general, stretching, and sleep can be particularly effective forms of physical integration
that stimulate positive somatic change and rebalancing. The effect of participating in
integrative activities can be improved cognition, greater creativity, and more flexibility
when new stimuli influence the body and mind (Bolesky, 2017).
Somatic Modalities Utilized in the Treatment of Trauma
What Jungian analyst Clarissa Pinkola Estés (1992) recognized has relevance for
all aspects of trauma work and somatic release: “The body remembers, the bones

17
remember, the joints remember, even the little finger remembers. Memory is lodged in
pictures and feelings in the cells themselves” (p. 200). What follows is an exploration of
a series of modalities that address somatically stored trauma rooted in physical,
developmental, psychological, emotional, and relational origins. This investigation into
each of these modalities is by no means exhaustive. There are literally hundreds of
modalities that address the release of somatic trauma (Shapiro & Forrest, 2016). Each of
the following sections offers a glimpse into a modality that informs this research.
Mindfulness breathing: One belly breath at a time. The breath bathes and
nourishes each cell of the body. Ecologist and philosopher David Abram (1996)
acknowledged the essential poetic nature of breath to human life:
The air is the most pervasive presence I can name, enveloping, embracing, and
caressing me both inside and out, moving in ripples along my skin, flowing
between my fingers, swirling around my arms and thighs, rolling in eddies along
the roof of my mouth, slipping ceaselessly through throat and trachea to fill the
lungs, to feed my blood, my heart, myself. I cannot act, cannot speak, cannot
think a single thought without the participation of this fluid element. (p. 225)
Spiritual teacher and counselor Mary O’Malley (2011) recognized the breath as a
doorway to be present for life, and to align the heart, mind, and body (p. 58). O’Malley
utilized many methods to strengthen awareness including mindfulness breathing. She
worked with clients individually and in weekly mindfulness meditation groups and has
led week-long retreats. O’Malley fostered an environment where hugs are welcome, eye
contact is encouraged, and breath becomes a gentle invitation into self-love. Silence is
still maintained for much of the time, but bonding between participants is encouraged.
Her mindfulness and breath work is full of heart.
Breath is part of the foundation of many somatic modalities aimed at releasing
trauma symptoms (Chodorow, 1991; Kabat-Zinn, 2013; Levine, 2010; Odgen & Fisher,

18
2015; Weiss et al., 2015). It opens tightness in the tissue when people focus on their
bellies rising and falling. Through their studies, psychiatrists Richard Brown and Patricia
Gerbarg (2012) have worked to legitimize the power of breath in U.S. medical and
psychiatric circles,
Breathing practice (pranayama) is one of the classical limbs of yoga. . . . Studies
are revealing that by changing the patterns of breathing it is possible to restore
balance to stress response systems, calm an agitated mind, relieve symptoms of
anxiety and post-traumatic stress disorder (PTSD), improve physical health and
endurance, elevate performance, and enhance relationships (p. 2)
Buddhist psychologist and Vipassana meditation teacher Jack Kornfield (1993) has
taught mindful breathing as essential for living a life of balance and awareness—as a
steadying force amidst the chaos of ever-changing life. It seems simple to work with
something as fundamental as breathing to help relax and open the body. It costs nothing,
it is always available to patients and practitioners alike, it is portable, and without the
ability to rely on consistent breath, very little else matters. Mindful breathing grounds
patients in somatic awareness they can touch and feel.
Mindfulness-Based stress reduction. Mindfulness-based stress reduction
(MBSR) is a somatic modality adapted from Vipassana and Buddhist meditation
techniques that fosters an 8-week series of daily breathing and awareness exercises
(Kabat-Zinn, 2013). MBSR programs began in hospitals as a way to reduce suffering and
stress and to increase wellbeing in hospital inpatients and outpatients. Molecular biologist
and founder of MBSR Jon Kabat-Zinn (2013) recognized the power of breath and its
ability to regulate emotion:
In focusing on the breath when we meditate, we are learning right from the start to
get comfortable with change. We see that we will have to be flexible. We will
have to train ourselves to attend to a process that not only cycles and flows but

19
also responds to our emotional state by changing its rhythm, sometimes quite
dramatically. (p. 41)
Research has been conducted on the use of MBSR in treating patients with
anxiety, stress, loneliness, chronic pain, PTSD, and depression, and has been found to
produce positive change in these patients (Kabat-Zinn, 2013). “This ‘work’ involves
above all the regular, disciplined cultivation of moment-to-moment awareness, or
mindfulness—the complete ‘owning’ and ‘inhabiting’ of each moment of your
experience, good, bad, or ugly. This is the essence of full catastrophe living” (p. ix).
Kabat-Zinn effectively brought mindfulness practices into mainstream medicine
internationally, offering great promise to reduce stress and trauma symptoms.
Acupuncture. Acupuncture can have profound and lasting effects on the body,
trauma patterns, and balancing emotional states to regulate affect (van der Kolk, 2014).
Its interconnections through the energetic meridian system in the body correlate to every
muscle, joint, bone, nerve, and organ in the body. It also affects qualities in human
experience such as mood, affect, and memory. Acupuncturist Kathleen Lumiere stated
that she treats cumulative physical and emotional trauma in her practice regularly, noting
that “the acupuncture points to treat anxiety are also many of the acupuncture points to
treat trauma” (personal communication, November 21, 2016). Describing acupuncture’s
efficacy in treating trauma, scholar and doctor of pulse diagnosis William Morris (2015)
described, “All traumatic events affect the heart and circulation. . . . Healing moves from
the inside to the outside, top to bottom, most important organ to least important organ,
and from most recent to the most past” (p. 30). In support of acupuncture and other
somatic modalities in treating trauma van der Kolk (2014) recounted

20
Dr. Spencer Eth . . . conducted a survey of 225 people who had escaped from the
Twin Towers [On September 11, 2001]. Asked what had been most helpful in
overcoming the effects of their experience, the survivors credited acupuncture,
massage, yoga, and EMDR, in that order. Among rescue workers, massages were
particularly popular. (p. 233)
In the study referenced above, van der Kolk noted acupuncture was the number one
modality New York residents chose to effectively treat trauma after the terrorist attack.
Energy psychology and the emotional freedom technique. The emotional
freedom technique (EFT) works by stimulating acupoints through gentle tapping,
referencing the same meridian system used in acupuncture and acupressure (Feinstein,
Eden, & Craig, 2005). The general EFT recipe begins with tapping the top of the head,
points on the face, the trunk of the body, and the sides of the hands. EFT falls within the
overall category of energy psychology (EP). “EP has been used to treat traumatic stress in
various groups, and is establishing itself as an evidence-based treatment for post-
traumatic stress disorder (PTSD), depression, anxiety, phobias, and other psychological
disorders” (Church, Piña, Reategui, & Brooks, 2012, p. 73; Feinstein, 2008). By
legitimizing energy psychology techniques as having profound results in one’s overall
health and wellbeing, the discussion of what constitutes effective psychotherapy is
broadened. Psychologist David Feinstein, energy healer Donna Eden, and EFT expert
Gary Craig (2005) explained that EP
approaches traumatic memories by sending electromagnetic impulses to the brain
that interrupt the intense emotional response the memory has been causing.
Unlike many other therapies, the emphasis is not on analyzing the memory and its
meaning. Rather, you work with acupoints. (p. 76)
EFT has been shown to affect neural responses including emission of a fear-
dampening signal to the amygdala and reduction of pain and fear in the limbic system of
the brain (Church et al., 2012, p. 74). To clarify the universality of energy work, all

21
human hands have “an electromagnetic field extending beyond the fingers, so simply
holding one’s hand over an affected part of the body can have a therapeutic effect, as can
massaging, tapping, or holding specific energy points on the skin” (Feinstein et al., 2005,
p. 5). Van der Kolk (2014) has had effective results utilizing EFT with his patients. He
has used EFT “to help patients stay within the window of tolerance and [this method]
often has positive effects on PTSD symptoms” (p. 267).
Eye movement desensitization and reprocessing. The modality of eye
movement desensitization and reprocessing (EMDR) was developed by psychologist
Francine Shapiro. Clinical psychologist Laurel Parnell (2013) trained under Shapiro and
described EMDR as “a powerful tool for catalyzing integration in an individual across
several domains, including memory, narrative, state, and vertical and bilateral
integration” (p. xii), and it “can work on reprocessing the traumas so that they lose their
emotional charge” (p. 139). Shapiro and Forrest (2016) explained that in EMDR therapy,
“rather than trying to talk through the problem, the processing occurs on a physiological
level and allows new associations, insights and emotions to emerge spontaneously” (p.
2).
EMDR therapy helps to reunite traumatic memories with the more resourced
aspects of memory and self-regulation. Shapiro and Forrest (2016) illuminated that
traumas and other experiences perceived as distressing can be held “in the wrong form of
memory. Instead of being stored in memory where they can be remembered without pain,
they are stored in memory where they hold the emotions and body sensations that were
part of the initial event” (p. 2).

22
Parnell (2013) created attachment-focused EMDR (AF-EMDR), a specific
relational trauma subcategory of EMDR that focuses on healing the wounds stemming
from insecure attachments, especially those in childhood with primary caregivers. Both
the original practice of EMDR and AF-EMDR utilize alternating stimulation with
physical tapping of the client’s limbs, subtle electrical impulses with paddles the client
holds, or eye movement stimulation conducted by an EMDR trained therapist to reduce
the heightened affect surrounding a memory or relationship.
Developmental and relational trauma have an impact on genetic expression and
brain processes can have long-term effects on how a person relates to and interacts with
life and with others (Siegel, 2013, pp. xiv-xv). AF-EMDR assists in catalyzing greater
levels of integration and flexibility for those who experience insecure attachment and
developmental trauma (Parnell, 2013). Siegel (2013) summarized AF-EMDR as a way to
treat “suboptimal regulation, such as difficulty balancing emotion, experiencing joy, and
ease or focusing attention in a flexible and adaptive manner; challenges with painful
traumatic memories; and unhelpful patterns of interaction with others that result in
troubled relationships” (p. xiv). As a somatic and energy-based rather than talk-based
modality, AF-EMDR may be helpful for those who find verbal exploration of their
trauma a threatening endeavor (Parnell, 2013).
Hakomi mindfulness-centered somatic psychotherapy. Hakomi mindfulness-
centered somatic psychotherapy was founded by the late therapist Ron Kurtz (1990) in
the 1970s. The word Hakomi comes from the Hopi Indian word, the current usage of
which means, “who are you?” The older meaning is, “How do you stand in relation to
these many realms?” The word Hakomi came to one of the Hakomi originators, David

23
Winters, in a dream (Kurtz, 1990, p. i; Weiss et al., 2015, p. v). Hakomi therapists assist
their clients in observing the consciousness that arises within them through practicing
mindful awareness, thus serving clients as a gentle witness. Hakomi therapists embody
what they call loving presence with the intention of attuning to clients in such a way that
they feel safe and held. Kurtz summarized key components of Hakomi:
The basic method is: create a relationship which allows the client to establish
mindfulness, evoke experiences in that mindful state, and process the experience
evoked. Experience mirrors internal organization. It reflects memories and beliefs
and those images of self and world which organize all experience. With mindful
evocation we move close. Just a step or two, a gesture, staying a little longer with
the experience, and we are at the core. Core material goes deep; organizing beliefs
are held firmly and defended strongly. . . . Core material is not accessible through
the intellect. But it is through mindfulness. (p. 4)
Psychotherapist Richard Schwartz (2008, 2015) founded internal family systems
therapy (IFS), a modality for interacting with unconscious parts of one’s self, or inner
figures, to create greater psychological integration and wholeness. Schwartz (2015)
validated Hakomi as facilitating a state of mindful observation that supports clients to
“release core, often unconscious, beliefs,” noting that “through this process, they were
helping clients access what I call the exiled parts of themselves—vulnerable, young, hurt
parts that I was trying to get to in a different way” (p. xi).
Psychotherapist and international Hakomi trainer Manuela Mischke Reeds (2015)
observed, “Clients categorize their lives in terms of before and after the trauma
experience” (p. 274; Herman, 1997; van der Kolk, 2014).
Many traumatized clients are not able to mobilize intellectual and physical
requirements for addressing . . . their trauma. They cannot operate within the
window of tolerance where the ventral vagal nerve facilitates our capacity for
social engagement, with ourselves or others. (Reeds, 2015, p. 273)).

24
For therapy to be effective, clients need to be able to make coherent sense out of
their trauma narratives. Facilitating states of mindfulness as a part of Hakomi can be an
effective way to encourage this growth (Reeds, 2015, p. 273). Reeds (2015) articulated,
All somatic psychotherapy that aims to negotiate the arousal of the nervous
system in elegant ways seeks to track and address activations and dissociations
beyond the client’s window of tolerance, so clients can actually be present with
their experience and find new ways of relating to triggers. (p. 276)
Hakomi therapists bring attunement, limbic resonance, compassion, and love to
their clients in an atmosphere of calm and quiet, paying attention to the present moment
and the client’s direct experience (Reeds, 2015). This above all is what trauma clients
seek in therapy—to feel safe, loved, and recognized with understanding (pp. 276-277).
Sensorimotor Psychotherapy.
In the instinctive psyche, the body is considered a sensor, an informational
network, a messenger with myriad communication systems—cardiovascular,
respiratory, skeletal, autonomic, as well as emotive and intuitive.
C. P. Estés, 1992, p. 200
Ogden, Sensorimotor Psychotherapy founder and educational director of the
Sensorimotor Psychotherapy Institute, and assistant educational director Janina Fisher
(2015) made the distinction, “The body’s intelligence is largely an untapped resource in
psychotherapy. . . . The story told by the ‘somatic narrative’—gesture, posture, prosody,
facial expressions, eye gaze, and movement—is arguably more significant than the story
told by the words” (p. 13). Sensorimotor psychotherapy is “a body-oriented talking
psychotherapy that specifically addresses trauma and attachment wounds, emphasizing
the body as an avenue for exploration and vehicle for change” (Ogden & Fisher, 2015,
p. 776). This modality was specifically designed to work with trauma and attachment
misattunements. “Resolving past trauma is not an act of will. It is the felt sense that the

25
trauma or threat is over. To experience a sense of having survived rather than a sense of
anticipatory threat requires autonomic and physical recalibration” (p. 537). Ogden and
Fisher (2015) explained,
A relational, attachment-focused therapy is a healing process not because
therapists are treating trauma and attachment; but because they are helping to
restore belief in the existence of human relatedness. The process of enactment
accomplishes this especially powerfully because it generates a here-and-now
reality that is created by both people in which the endangered attachment becomes
repairable right in the room. (p. 51)
Much of what sensorimotor psychotherapy does for clients is to slow down
processes and bring attention to breathing, posture, movement, and ways of relating, and
assess whether they are still valid or whether a change might increase wellbeing (Odgen
& Fisher, 2015). This form of therapy works with the edge of a client’s window of
tolerance to expand the window itself. This modality emphasizes the wisdom of both the
body of the therapist and the client as self-awareness is tracked and explored.
Somatic Experiencing®. Levine (2010) created Somatic Experiencing® as a
trauma treatment modality from his recognition that trauma resides not only the brain or
mind, but also in the body. This modality addresses the held patterns of tightness, tension,
and what the body somatized as real or imagined threat. Levine (2010) synthesized
multiple techniques inclusive of eye movements, vocal toning, postural changes, talk
therapy, and verbal cues. In a video recording of a portion of a session, Levine guided a
former Marine with PTSD through vocally toning while tracking Levine’s finger back
and forth, and up and down; at the end of the exercise, Levine gave the verbal cue: “And
rest” (Brooks & Walkenhorst, 2014). Levine (Brooks & Walkenhorst, 2014) summarized
that Somatic Experiencing® “…helps individuals have new experiences in their bodies,
where they feel more powerful, more centered, more grounded, then they’re able to deal

26
with those traumatic memories in a much better way—in a way that is embodying and
empowering” (3:01).
Nine key principles form the framework of Somatic Experiencing®: establishing
safety; exploring sensation; establishing pendulation and containment; titrating small
drops of trauma experience; providing a corrective and empowering experience;
separating conditioned associations of fear from biological immobility responses;
supporting self-regulation and dynamic equilibrium; and orienting to the present moment
(Levine, 2010, p. 75). Levine highlighted the essential importance of kindness and
noninvasive support when practicing this modality.
Soma Neuromuscular Integration® Bodywork. Soma Neuromuscular
Integration® is a structural integration modality created in 1977 by psychologist and
Rolfer® Bill Williams and his wife Ellen Gregory Williams (Bolesky, 2017). In Greek,
soma means “the body as distinct from the soul, or psyche,” but in the ancient Greek
language soma included mind and spirit (“Soma,” 2017, def. 2). Director of the Soma
Institute Karen Bolesky (2004) explained “The added layer of acknowledging body,
mind, and spirit as an inseparable whole system supports the multidimensional human
being” (p. 1). She recognized,
Our bodies want to heal, to feel great. But sometimes with accidents, stress,
abuse, trauma, and self-criticism, we forget to allow our body to listen to itself.
We forget, literally. If the body can return to being a listening mechanism, it will
heal. All touch therapy whether structural integration or massage, has the goal of
supporting the client’s body to heal—to feel great. Perhaps what we are doing as
somatic educators is pointing the client’s attention (which has often wandered)
back to their own precious body. (p. 1)
Soma is a method that takes place in 10 sessions to align the connective tissue of
the body to function as it was biomechanically designed to function, with an optional

27
11th session for further integration, known as Somassage®. Clients experience body
reading; fascial manipulation on a massage table; are guided to practice integrative
movement exercises; draw their bodies before and after sessions; and have the ability to
utilize a client notebook throughout the 10-11 sessions. Soma Neuromuscular
Integration® deep tissue massage encapsulates processes that address mind, body, and
emotions by accessing the fascial web that wraps every organ and links every muscle
(Bolesky, 2004). Thus, working one part of the fascial web influences associated parts
elsewhere in the body. The deep tissue massage releases trauma from the fascia and
connective tissue that hold body memories and associations.
Authentic Movement. Authentic movement opens the body into a state of free
association in which the contents of the psyche translate into spontaneous movement,
vocalizations, and emotions, and are witnessed by an observer (Konopatsch & Payne,
2012). Founder of authentic movement and dance therapist Mary Whitehouse (2007)
initially conceptualized this method of work through her own journey as an analysand in
Jungian therapy where she was inspired by the relationship between active imagination
and free association of movement (Konopatsch & Payne, 2012). Psychiatrist Carl Jung
(1956/1970) developed the process of active imagination in which one focuses on a
dream or fantasy as reflective of “psychic processes in the unconscious background,
which appear in the form of images consisting of conscious memory material. In this way
conscious and unconscious are united, just as a waterfall connects above and below” (pp.
495-496).
In this way of connecting above and below, conscious and unconscious, implicit
memory with explicit memory, practicing authentic movement in individual or group

28
settings offers a new way to communicate within oneself and with the therapist
facilitating the session (Konopatsch & Payne, 2012). Often there is music playing that
helps to evoke kinesthetic and emotional experiences across a range from sorrow to
ecstasy. “Authentic movement, as an approach to self-exploration, intends to create a
space for hidden, unconscious and sensitive personal themes to be explored. The ground
form of Authentic Movement involves two people, termed ‘mover’ and ‘witness’”
(Konopatsch & Payne, 2012, p. 342). Authentic Movement can evoke the release of
many forms of trauma as the mover is silently received by the witness. If there are body
issues, shame might arise, followed by tears, or sighs—small movements or sweeping
gestures. The witness acts as a source of loving presence and affirmation, which in
redressing issues of traumatized attachment, is cathartic in and of itself.
Attachment and Bonding: What Love Has to Do With It
Clinical psychologist and founder of emotionally focused therapy (EFT) Sue
Johnson (2013) wrote, “We need emotional connection to survive. Neuroscience is
highlighting what we have perhaps always known in our hearts—loving human
connection is more powerful than our basic survival mechanism: fear. We also need
connection to thrive” (p. 23). There are many components to self-regulation that dovetail
with attachment and bonding. There seems to be a correlation between affect regulation
and the ability to experience self-love and self-worth (Bram & Peebles, 2014, p. 255).
“These states of mind can be based on secure attachment experiences in which we feel
seen, safe, soothed, and secure—the ‘four S’s of attachment’ that serve as the foundation
for a healthy mind” (Siegel, 2013, p. xiii). For those who did not grow up with
relationships that facilitated feeling securely attached, indeed there is hope. There is

29
recognition among many experts in the fields of psychology and neuroscience that secure
attachment can be cultivated at every phase of development throughout one’s lifespan
(Crain, 2011; Johnson, 2013; Siegel, 2012). Chapter III builds on the research discussed
above in presenting an analysis of the creation of a sacred space that provides for the four
S’s of attachment.

Chapter III
Findings and Clinical Applications
Encountering the Sacred Temenos
The body is a multilingual being. It speaks through its color and its temperature,
the flush of recognition, the glow of love, the ash of pain, the heat of arousal, the
coldness of non-conviction. It speaks through its constant tiny dance, sometimes
swaying, sometimes a-jitter, sometimes trembling. It speaks through the leaping
of the heart, the falling of the spirit, the pit at the center and rising hope.
C. P. Estés, 1992, p. 200
To approach the human body with a sense of its dynamic, awe-inspiring, and
wondrous nature allows for the sacred to enter back into the practice of psychotherapy
and somatic psychology. I think the word sacred has become loaded with religious
connotations—whether favorable or unfavorable. But I would like to resurrect the word
sacred to mean a deep sense of honoring soul essence. Moore (1992) wrote, “Soul has to
do with genuineness and depth, as when we say certain music has soul or a remarkable
person is soulful. Soul is revealed in attachment, love, and community” (p. xii). When I
conceptualized the title of this thesis as Encountering the Sacred Temenos: Somatically
Integrating Cumulative Trauma and Discovering Wellbeing Within, I very consciously
added the word sacred. To me being invited to witness the inner and confidential
processes of a client or a friend or family member is an honor and in that way sacred. The
word sacred comes from the antiquated verb sacren “to make holy” and from the “Latin
sacrare, to make sacred, consecrate; hold sacred; immortalize; set apart; dedicate”
(Harper, 2017, para. 1). It is my belief that life and all of nature is miraculous and I

31
intentionally chose to elevate the safe container and the members held within it to honor
the presence of soul and spirituality.
Levine (2010) concurred about spirituality as an essential focus in trauma work
when he wrote, “In a lifetime of working with traumatized individuals, I have been struck
by the intrinsic and wedded relationship between trauma and spirituality” (p. 147). What
he meant by this was that the process of catharsis from wounding to releasing trauma to
reintegrating into wellbeing has brought profound and spontaneous expressions of
ecstatic joy, tears of gratitude, and “an all-embracing sense of oneness” (p. 147). This can
occur for clients, health professionals, wilderness therapy guides, and therapists who
witness and help to facilitate such a metamorphosis. I have experienced this in my own
practice as a body and energy work practitioner as well as in my training to become a
psychotherapist.
Somewhere along the way, in modern society, government, and the insurance
industry, the broad recognition of sacredness and soul in therapy got lost as an overall
tenet to treating emotional balance and wellbeing. This is true of the healing that occurs
in the myriad of modalities that tend to the body and mind. In ancient Greece there were
references to healing temples, places of great beauty and architecture with fountains and
interior courtyards—a temenos-like space in honor of the healing gods and goddesses in
the polytheistic pantheon such as Hygiea and Asclepius (Campbell, 2013, pp. 120-121).
The word temenos originates from the ancient Greek notion of a sacred healing temple
and, according to Jungian analyst Daryl Sharp (1991), when defined in a Jungian sense it
means “a sacred, protected space; psychologically, descriptive of both a personal
container and the sense of privacy that surrounds an analytical relationship” (p. 133).

32
Jungian analyst and somatic therapist Jean Chodorow (1991) defined working with the
concept of a temenos as “a safe and secure space within which unconscious fantasies and
conscious dilemmas can be safely dealt with. The nature of this dialectic between patient
and therapist is fostered by an empathic mirroring on the part of the therapist” (p. 7).
The term temenos as I use it is a place of safety and wholeness where the sacred
work of depth psychotherapy can occur—honoring the ancient tradition of creating an
exalted space. This creation of a temenos can happen in a windowless office on the
corner of a busy street in a community mental health clinic. I make use of soft lighting,
images of peace in nature on the walls, comfortable seating, plants that detoxify and
oxygenate the air in the room, and work with a steady and calm tone of voice as subtle
influences in the creation of a temenos. Yet above all, creating a temenos is about the
energetic held by the therapist, facilitator, or health professional. Being surrounded by the
beauty of nature or in an architecturally uplifting space certainly adds to the creation of
such energy, but it is not essential. The sacred temenos is largely about intentionality.
Historian and archeologist Asia Shepsut (1993) acknowledged the universe and Earth as
macrocosmic representations of the sacred temenos and spaces created to reflect the sense
of being held as microcosms of that greater, cosmic container. Shepsut furthered this
concept when she explained,
Wherever it is, however you do it, create some spot which ritualizes The Centre of
the World. . . . You will notice that creating this sacred space will have an
immediate, regulating effect on activities of a more practical nature that go on
outside it. (p. 29)
One of the primary clinical or facilitative functions of the creation of a temenos is
to create a sense of emotional safety where deeper and more vulnerable layers of human

33
experience, inclusive of cumulative trauma, can be revealed while being securely
contained by the loving presence of the therapist or other health professional.
Trauma as Cumulative and on a Continuum
Both PTSD and developmental trauma are considered macro levels of trauma,
but if trauma is seen on a continuum, varying degrees of micro traumas may occur in
which an event causes subtle neurophysiological fear reactions. There are professionals
and individuals in all walks of life who have encountered various forms of trauma or
traumatic stress and these instances can occur at any time in one’s lifespan (Parnell,
2013; van der Kolk, 2014). An employer, spouse, professor, or other person in power can
be an influential figure in relational micro or macro trauma for an adult, just as a parent
can be a tremendous source of wounding for a child (Parnell, 2013). After years of
accumulated micro traumas, peoples’ ways of relating to others and to themselves can
become in a sense clogged or distorted and in need of relief from the struggle to maintain
emotional equilibrium and defend against further trauma.
Psychotherapy and somatic modalities that address trauma are ways to work with
transforming cumulative trauma. Aron (2010) further clarified and broadened the
definition of the forms of trauma people experience:
When we say someone has had a traumatic physical injury, it means the body has
lost its wholeness in some way: the skin has been deeply cut, a bone has been
broken, or an organ has been injured. Trauma happens to the mind as well, either
with or without physical trauma. It occurs when emotions are not just
overwhelming but in some real sense unbearable. With enough stress and a sense
of powerlessness to prevent more stress, the mind loses its wholeness and “falls
apart,” “breaks down,” or “goes to pieces.” The brain goes through changes that,
although often reversible, are equivalent of an injury. Trauma can be acute, an
abrupt experience, or chronic, something that grinds you down over time. (p. 77)

34
Aron’s (2010) description hints that trauma can be seen on a spectrum from
physical to emotional, or psychological. Psychologist and faculty member of the Seattle
Psychoanalytic Society and Institute Margaret Crastnopol (2015) defined micro-trauma
as way to differentiate repeated, built-up, minor hurts . . . less obvious or direct in
destructive quality. . . . The hurtful quality may reside only in the tonal
undercurrents or peripheral implications of the act rather than in its main message.
(p. 5)
Crastnopol (2015) further discussed her observations about micro-trauma when she
wrote, “In the area of micro-trauma at least, telescoping betrays itself when the reaction
to the event seems truly disproportionate; under these circumstances, we often discover
on further inquiry that the particular blow was only the latest in a series” (p. 10). A
therapeutic temenos needs to invite and hold as sacred the process of deepening, paying
the depth of attention to a client that does not overlook, but rather looks within, micro as
well as macro traumas.
Cocreating the Sacred Temenos with Patients and Clients
It was the fall of 2010 and I was at a crossroads in my life. I was desperately
ready for a change, pondering what was calling me from within. Nature is a healing balm
for me, so I hiked to sit perched on a rock outcropping atop Mount Erskine on Salt Spring
Island, British Columbia. As I gazed out over the labyrinth of calm, sun-sparkling waters,
an insight came illuminating what I believe to be the core emotional needs of humanity.
The words safety, trust, acceptance, belonging, and love came forth. I realized then that
emotional wounds stem from a lack of these qualities.
STABLE©: Safety, Trust, Acceptance, Belonging, Love, Earth, and Ecopsychology
As I worked with these needs, one additional need came forward, and that was the
human need to connect with Earth as a living being. To further honor and clarify the vital

35
synergy of nature and psyche, I added the term ecopsychology. From these foundational
needs the acronym STABLE© formed, which stands for Safety, Trust, Acceptance,
Belonging, Love, and connection with the vibrancy of Earth and Ecopsychology as a
source of nourishment. Ecopsychology can be thought of as the connection between
one’s psychological and emotional state being inextricably interrelated with the energy
and physical health of Earth (Roszak, 1992; Roszak, Gomes, & Kanner, 1995).
During my clinical practicum I found that many of my clients were seeking
stability within themselves and in their outer life circumstances that were often
dominated by financial strain and, for some, homelessness. I wanted to offer something
that could add hope and be a reminder of the qualities of life that are available to
everyone. STABLE© evolved to align with the seven colors of the rainbow to help my
clients visually connect with the concepts, especially the children and teenagers. During
my final sessions with several of my clients ranging in age from six into adulthood, I
drew the image of a vibrant rainbow with the acronym and the words that comprise it.
The drawing was meant to be a transitional object that my patients could keep to
remember the important work we did together and the bond we shared. It seemed from
their responses that the simple gift of the drawing added meaning and closure to our
therapeutic relationship. The rainbow STABLE© drawing (Appendix A, Figure 5)
offered clients a way to remember some of the emotionally supportive core values that
were addressed during sessions.
The drawing below (Figure 1) is a result of my continued and deepening work
with the acronym I conceptualized to represent the key elements of mind, body, and
emotional nourishment that lead to resilient and effective functioning. I noted its
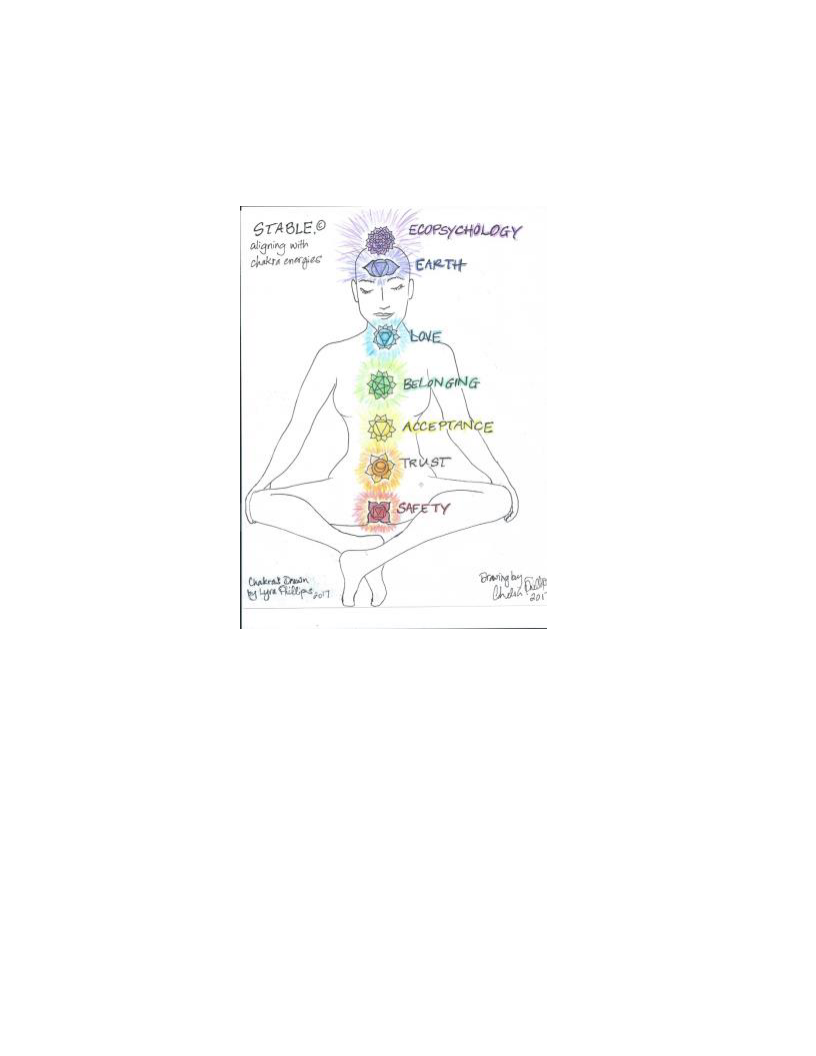
36
relevance in accord with the seven chakras, which are Ayurvedic energy centers that
correlate with the spine of the body from the perineum to the top of the head, root to
crown (Judith, 2004).
Figure 1. STABLE©. Illustration of relationship between the human needs and the
chakras. Drawing by author, 2017.
Chakras align with rainbows, as they share the same color spectrum and they are
often represented as lotus flowers with specific geometric shapes, as shown above
(Judith, 2004). Working with the framework of STABLE©, one can conceptualize the
image to begin from the root chakra whose color is represented as red and is located at
the perineum, or base of the spine, which is Safety. The second chakra is located just
below the navel and is considered the sex chakra or center of creativity. Its color is
orange, which aligns with the word Trust. The third chakra is yellow and is considered

37
the will chakra; its word is Acceptance. The fourth chakra is green, is located in the
center of the sternum, and is known as the heart chakra; its word is Belonging. The fifth
chakra is associated with the color blue, is located at the throat, and its word is Love. The
sixth chakra resides just above and between the eyebrows. Its color is indigo and it
connects with Earth. Ecopsychology, the study of psyche and Earth as interrelated, is
represented with the color violet. It resides at the top and center of the head (Judith,
2004).
I imagined that physical and emotional safety and grounding in the root chakra
was the foundation upon which all other energies are built. I saw this leading to a greater
sense of trust in the second, relational chakra, which can then open the door to feeling
acceptance from others, adding to experiencing greater self-acceptance, which is related
to the energy of confidence at the third chakra in the solar plexus. This can lead to a
deepened sense of belonging, related to the energies of the heart chakra and love. The
world becomes more dependable when the solid foundation of the first three core needs
have been redressed by a reliable therapist as respectful and honoring witness within a
sacred temenos. When there is a felt sense of safety, trust, acceptance, and belonging it
becomes more possible to give and receive love. From this place of stability, connecting
with Earth adds to self-care by communing with nature to resource oneself.
Earth and Ecopsychology
Earth is represented by the sixth chakra at the third eye in the center of the
forehead, which has to do with intuition, visualization, imagination, and dreaming
(Judith, 2004). Connecting with the essence and energy of the natural world adds to a
sense of being able to imagine and dream. Van der Kolk (2016) reported that research has

38
shown that when people can imagine their future again—create goals and seek to
accomplish them—they are healing their trauma. This is a sixth chakra function, and
spending peaceful time in nature can add to one’s ability to visualize, rejuvenate, and
create. This is possible when the core needs of maintaining a certain degree of felt safety;
trust in the world; acceptance of self and others; a feeling of belonging; and some sense
of love has occurred.
For people in a state of crisis, receiving the healing power of nature and the
chance to dream is often not on the radar. I can think of a female victim of domestic
violence who could not remember the last time she had gone to the ocean even though
she lived 15 minutes away and had loved going in the past. Leaving her home did not feel
safe and due to somatized trauma she lacked the psychic and physical energy to go to the
beach. Tending unresolved trauma and her core needs for safety, trust, acceptance, and
love had to come first before she would resume going to the beach again regularly.
I added ecopsychology as the seventh chakra and the hidden E in STABLE©
because when people feel higher levels of their wholeness, a felt sense of the wellbeing
and connection with all of life can occur. The late Theodore Roszak, social activist and
social scientist (1992, Roszak et al., 1995), first coined the term ecopsychology—in
essence blending the words and concepts of ecology and psychology. Roszak (1992)
explained,
Once upon a time, all psychologies were “ecopsychologies.” Those who sought to
heal the soul took it for granted that human nature is densely embedded in the
world we share with animal, vegetable, mineral, and all the unseen powers of the
cosmos. (p. 14)
And yet, so many people experience feelings of separateness, a lack of belonging,
a lack of safety, a longing for love, and on the whole a longing for connection. This

39
blended field of therapy arose out of the notion that people have cast a spell on
themselves and ascribed to the notion of being separate from nature. This spell needs to
be broken so that humanity can live from a place of wholeness within the web of life.
Therapy for people has existed in a bit of a vacuum—as though the four walls
surrounding client and therapist could contain all the healing necessary to put a person
back together. By opening to therapy in natural settings outside, there is a chance to feel
one’s nature as “the Wild Indigenous One [who] is our most instinctual dimension, every
bit as natural and at home on Earth as any elk, elm, or alp” (Plotkin, 2013, p. 51). Human
bodies are ecosystems, walking around completely influenced by the other systems they
encounter. As an ecosystem the body can become physiologically unbalanced by and
contain remnants of the trauma. This then can be seen linking ecopsychology with the
importance of somatic-oriented therapy.
Exploring the Application of Somatic Modalities
I am fascinated by how trauma resides in the body and in one’s memory at the
same time. Professor of somatic psychology at the Naropa Institute, Christine Caldwell
(2012) discussed the neuroscience of what happens when clients in a therapeutic
relationship experience memories:
When we remember, we bring the past into the context of the present, and as that
past surfaces, it is exposed to the different experiential elements residing in the
here and now. If those new elements are safe, calm, welcoming, and relationally
secure (i.e. a therapeutic relationship), a painful memory can be consciously
worked with on a body level, as a way to re-encode the past situation with new,
more regulated associations. (p. 261)
I participated in these exact phenomena with my clients during my clinical
practicum when I worked with them utilizing the somatic methods of deep breathing,
mindfulness, and EFT tapping to release and integrate trauma. First and foremost, as I

40
began my exploration of somatic modalities in the literature with breath work, I began
with something free and simple: breathing. Trauma can cause people to hold their breath
unconsciously, among other symptoms. I have witnessed this firsthand in my own body
through the practices of Vipassana meditation and mindfulness techniques, as well as
being the recipient of many forms of body and energy work over the past 25 years. In
essence, mindfulness of holding one’s breath begins with simply bringing one’s attention
to it in the present moment.
Different modalities can be effective for different clients. In both my practice as a
Soma Neuromuscular Integration® bodywork practitioner and as a psychotherapist in
training, my experience with mindfulness breathing and EFT tapping have been highly
effective for many clients. The youngest clients with whom I have tried mindfulness
breathing and EFT tapping were 6 years old. Perhaps it might work with children even
younger. For example, one delightful and precocious 6-year-old girl liked the
mindfulness breathing and worked with it at home, but did not like the feeling of tapping.
Other clients ranging in age from 6 to in their mid-60s also enjoyed the mindfulness
breathing but did not prefer the EFT tapping, whereas others experienced greater ease and
more calm when in heightened states of arousal using the simple tapping technique. I
found combining mindful belly breathing and EFT tapping a great way to work with
teenagers when I cofacilitated a group on mindfulness and emotional regulation.
As a client, I have found acupuncture, EFT self-tapping, EMDR, Soma
Neuromuscular Integration® bodywork, chiropractic care, and energy medicine
particularly effective in the somatic release of cumulative trauma. Each of these
modalities assists in a process of reintegration from trauma into a felt and lasting sense of

41
wellbeing. EMDR seems specifically indicated for single incident trauma, whereas
Parnell’s AF-EMDR (2013) has been adapted to work with cumulative, relational, and
developmental trauma. One can imagine that this methodology, especially from a
relational trauma perspective, could be useful in treating levels of trauma across a
continuum—from micro interactional traumas to more egregious incidents or durations of
highly charged relational instability.
Affect Regulation and the Introduction of Conscious Co-Regulation
Ogden and Fisher (2015) summarized regulation as it relates to self, affect, and
emotion as “the ability to monitor and modify internal processes; to soothe or intensify
our emotions, arousal, and sensations until they do not feel uncomfortably low or high, to
bring arousal within a window of tolerance” (p. 776). During my clinical practicum, I
tracked the state of regulation in my clients and their families as part of ongoing
assessment. One particularly interesting example of dysregulation coming back into
balance with somatic methods is discussed in Appendix B. I include how I used the
framework of STABLE© with this caregiver and the effect it had on the overall session.
The concept of co-regulation was introduced to me by the supervising
psychologist at my practicum during a session of group supervision. “Co-regulation is an
important quality of interaction during which the dyad functions as an integrated entity to
regulate each other’s behavior” (Fogel, 2000, p. 1150). Sitting with this new concept, I
found myself making associations of how often co-regulation occurs. As a therapist,
bodyworker, and energy medicine practitioner I reflected on how I have been in co-
regulating loops of interaction with my clients without calling it as such. Previously, I
called co-regulating with another person empathic attunement or helping someone to

42
ground their energy, but the term co-regulation gets to the heart of what is happening. In
family systems Bowen and Kerr (1988) referred to this as a borrowing or trading of self. I
prefer the concept of co-regulation because it fits with an attachment perspective of the
affiliative nature of human beings; that as communal creatures, people can assist one
another in co-regulating in a strength-based way when they become aware that co-
regulation is an option.
Consciously co-regulating one another is far different from unconsciously
entraining to the energy of others, which can have negative or positive effects depending
on the affect present. I have been experimenting with conscious co-regulation with family
members and specific friends who have a calming and regulating effect in my life and
whom I in turn co-regulate. As a therapist co-regulation can help a client stay present to
memories as they arise from the unconscious and as well as return to a state of
equilibrium when encountering the arousal of distressing affect.
Shadow Integration
Trauma work is depth work inclusive of shadow. Sharp (1991) defined shadow as
hidden or unconscious aspects of oneself, both good and bad . . . either repressed
or never recognized. . . . All those things about oneself one is not proud of. The
unacknowledged personal characteristics are often experienced in others through
the mechanism of projection. (p. 123)
I have found shadow integration to be a key component in coming to terms with the
wounds life brings for me and for my therapy and bodywork clients. Although there are
the wounds of trauma that are socially acceptable, such as being the victim in a car
accident, there are also trauma wounds that people would rather not share aloud. These
wounds are crying to be met with the arms of love. Levine (2010) spoke to working with
one’s shadow and to the notion of healer heal thyself when he sought the original wisdom

43
of shamanic cultures and then contrasted two methods of going about the treatment of
patients.
In common therapy . . . the therapist instructs the PTSD victim to assert control
over his feelings, to manage his aberrant behaviors and to alter his dysfunctional
thoughts. Contrast this alignment to that of shamanic traditions, where the healer
and the sufferer join together to re-experience the terror while calling on cosmic
forces to release the grip of the demons. The shaman is always first initiated, via a
profound encounter with his own helplessness and feeling of being shattered,
prior to assuming the mantle of healer. Such preparations might suggest a model
whereby contemporary therapists must first recognize and engage with their own
traumas and emotional wounds. (pp. 34-35)
Jung (1937/1966) wrote, “An analyst can only help his patient just as far as he
himself has gone and not a step further” (p. 330). I agree with Jung’s assertion that as a
therapist or any health practitioner, it is essential to explore and heal personal wounds. It
is a part of shadow integration and movement toward a felt sense of wholeness within.
This is certainly true in the practice of effective trauma work.
Integration in the practice of psychotherapy involves bringing aspects of a client’s
shadow to consciousness. Shame and anger are two energies that are essential to meet in
the process of shadow integration. There is a saying that shame is anger turned inward.
Once shame is identified, how can one work with it to help this frightened expression of
self return to equilibrium and wellbeing? To shed some light on how to work with shame,
an emotional experience so often encountered in the treatment of trauma, Gestalt
therapist Robert Lee (2007) revealed,
The phenomenon of shame encompasses much more than our common cultural
sense of having done something wrong, this being shameful, or of being flawed in
some manner. At its core, shame is about pulling back. It is our way to attempt to
protect ourselves or others when we perceive that we won’t be received. (p. 2)
Schwartz (2008) acknowledged that there are different parts of the self that have
needs and their own unique voice—parts such as the protector or an exiled one. In this

44
method of seeing the various parts of self, the one who feels ashamed and the angry one
could be added to help in the understanding of what part is acting out, and thus seeking to
be integrated back into wholeness. Jungian analyst Monica Wikman (2004) discussed
shadow integration in a way that speaks to my understanding of the process.
Integration experiences come as the fruit of the hard work, and the journey, and
stem from a life lived close to the unconscious for the sake of this inner
development of unity itself. Integration experiences also stem from weathering
the storms of inner and outer life in such a way that instead of splitting between
the opposites, a new unity is born. When the alchemical processes have cooked
the complexes long enough into ash, the manifest Self emerges, and acceptance
and joy return. (p. 280)
The image of inner processes being cooked and turned to ash, ready for the
phoenix of the soul to emerge, awakens the poetic beauty that can be present in trauma
work and the healing of emotional wounds. When they are not seen as something to hide
from they can represent the strength that comes from surviving and emerging, wizened
and more whole. Wikman’s (2004) summarization of being catalyzed by alchemical
transformation segues into what I see as a myth that demonstrates the initiation potential
of trauma integration.
The Myth of Inanna as an Allegory for Processing Trauma
Trauma experiences can be seen as taking the form of a kind of initiation. The
myth of Inanna depicted an initiation into and a return from the underworld—a theme in
ancient myths recorded in numerous cultures (Perera, 1981). Jungian analyst Sylvia
Perera (1981) noted,
There are many myths and tales about the descent of and to the goddess . . .
Japanese Izanami, the Greek Kore-Persephone, Roman Psyche, and the fairytale
heroines who go to Mother Hulda or Baba Yaga or the gingerbread house witch.
(p. 9)

45
The myth of Inanna from 3rd millennium BCE is considered the oldest recorded allegory
that acknowledged this theme of a descent, an alchemical transformation, and an ascent
back into usual life—forever changed with the opportunity to honor oneself for the pain
and sacrifices made to do one’s inner work (Perera, 1981, p. 9).
Inanna’s descent through the seven gates to the underworld can be a helpful lens
when reflecting on a client’s experience of trauma symptoms. A correlation can be made
between the underworld’s gates and the seven chakras in the human energy system. The
root chakra would begin at the crust of the earth where heaven meets Earth—the seat of
safety in the world that is lost when trauma occurs. From there life force must be rebuilt.
A stripping away of vitality and life force occurs when trauma shakes the foundation of
one’s being—the root, the first gate. Some people may experience a more subtle or mild
death, transformation, and rebirth process and others may experience a cycle of initiation,
or dark night of the soul, that lasts for years (Henderson, 2005; Moore, 2004). This
depends on what kind of wound or relational trauma occurs and on the level of one’s
resilience at the time of the psychic injury. How long a person’s transformation through
trauma takes is not to be taken as a value judgment about how evolved a person is. Rather
it reflects the nature of trauma as on a continuum from micro to macro, and as cumulative
as well. There may be parts of a person in multiple layers of death and rebirth processes
simultaneously, while on the outside, they are performing all the duties of their life with
seeming ease. Humans are complex creatures.
The final chakra correlates to the seventh gate, entering into the heart of the
underworld, to experience the process of alchemical metamorphosis, or shadow
integration. The myth of Inanna is an analogy of being alchemically changed by facing

46
one’s trauma and transforming through it. When one goes through a traumatic event or
experiences a resurfacing of cumulative trauma symptoms, it may feel as though the
person is experiencing a loss or a death, just as Inanna did at the hands of Ereshkigal,
queen of the underworld.
For some clients descent may involve the depressive or anxious symptoms of
apathy, grief, tearfulness, hyposomnia, hypersomnia, nervousness, hypervigilance, anger,
verbal outbursts, or even physical altercations when extreme dysregulation or substance
use is involved. Learning to own one’s own shadow can be highly effective in the process
of transforming mental behavior from judging others and one’s self to seeing through the
eyes of compassion. Symptoms then become cues that soul is seeking to point out a
certain wounded part of self in an attempt to rebalance into a state of wellbeing and
wholeness. Cultural anthropologist and mythologist Joseph Campbell (1988) illuminated
some of the essential and universal wisdom that is born out of the hero’s journey:
We have not even to risk the adventure alone, for the heroes of all time have gone
before us. The labyrinth is thoroughly known. We have only to follow the thread
of the hero path, and where we had thought to find an abomination, we shall find
a god. And where we had thought to slay another, we shall slay ourselves. Where
we had thought to travel outward, we will come to the center of our own
existence. And where we had thought to be alone, we will be with all the world.
(p. 123)
Campbell (1988) alluded to Ariadne with her spider’s thread guiding the hero by
way of offering a path to return home—being a priestess or facilitator in the journeys of
psyche and soul. The theme of entering the process of transformation—the labyrinth—
and returning home, experiencing unification with all of life showed up in the myth of
Inanna as well (Perera, 1981). The myth of Inanna is a hero’s journey. Ninshubar,
Inanna’s handmaiden, waited for her at her point of descent and when Inanna failed to

47
reappear at the appointed time sent for help—Ninshubar played the same role for Inanna
as Ariadne in the labyrinth myth by holding the knowing of Inanna’s wholeness.
The theme of departing, going through trials, and returning changed shows up in
stories and myths throughout history with male and female protagonists. So many
therapists and health care professionals can relate to the journey of being transformed
through rites of passage inwardly or outwardly in their own lives. Some might say to be
truly effective in helping others the wound of Chiron is inevitable. The myth of Chiron
centered on receiving a wound or trauma (Ronnberg & Martin, 2010, p. 738). The wound
itself became the wizening agent of initiation—one where compassion and empathy grew
out of being able to relate to the pain of another. Out of vulnerability, woundedness, and
experiencing trauma wisdom emerged.
Discovering and Cultivating Wellbeing
If you travel far enough, one day you will recognize yourself coming down the
road to meet you. And you will say YES.
Woodman, M. & Mellick, J. 2000, p. 98
When I conceptualized the importance of the topic of wellbeing in this thesis, I
recognized that every time I experienced trauma, whether micro accumulations or macro
incidents, I went through a catharsis and reintegration that led to greater wholeness and
wellbeing. Siegel (2010) brought to light the idea that “integration is at the heart of
wellbeing” (p. 32). I observe this with my clients as well. There is another way that I saw
wellbeing as essential, which is to connect with the restorative properties of the natural
world. The E in STABLE©, stands for Earth as it relates to experiencing solace in nature
in addition to pertaining to the potential for ecopsychological connection with Earth,

48
where psyche experiences oneness with all of life—the miraculousness and the
degradation.
I resonate with Siegel’s concept of returning to the river of wellbeing from the
shores of chaos and rigidity (Siegel & Bryson, 2011, p. 11). I use this metaphor with
many of my clients. It appeals to clients of all ages. I think of the river of wellbeing as a
place of balance and cortical calm between the vacillation of depression and anxiety
experienced by so many of my clients. In fact, I see depression and anxiety symptoms on
a continuum. Professor and clinical neuropsychologist at Cal Poly University in San Luis
Obispo, California, Mike Selby (2016) reflected that he most often sees depression and
anxiety symptoms as co-occurring. Selby’s assertion that anxiety and depression are often
co-occurring was eye opening for me in addressing these symptoms clinically. Whereas I
had been working with a mental model of depression being on one end of a continuum
and anxiety being at the other end, Selby (2016) added an interactive dimensionality to
these two categories of emotional symptoms. Now, I see these states as far more
dynamic, almost as if a person who experiences depression and anxiety is in an inner
dance with his or her symptoms in an attempt to find balance and wellbeing.
The use of adjunctive therapy in collaboration with other practitioners can be
highly effective in supporting clients to re-enter the river of wellbeing (Siegel & Bryson,
2011). Mindfulness is an integral component cultivating a connection with the river of
wellbeing within oneself. Like a waterfall that is tumbling into a deep pool someplace on
this vast jewel of a planet in this very moment right now, the river of wellbeing is
constantly flowing awaiting the return again of an earnest and attentive explorer.

49
Clinical Applications
The framework of STABLE© can be applied universally. Addressing the human
needs of feeling emotionally and physically safe; being able to trust others; feeling
accepted; experiencing a sense of belonging; receiving the energy of loving or
compassionate presence; and resourcing with a connection to the earth adds to a felt sense
of wholeness. Moreover, it is important to recognize how inextricably connected the body
and human psyche is with planet Earth and with one’s environment in an
ecopsychological sense. It is my belief that all people need what STABLE©
encapsulates, and that these are healing balms to the wounds of humanity. This model can
be adapted to work environments, government structures, social justice practices, post
war adjustment, conflict resolution, school and university settings, family values, spiritual
practices, and health clinics as tenets for mindfulness. As a model, STABLE© can be
used in conjunction with Maslow’s (1943, 1954) hierarchy of needs to add the dimension
of the chakra analogy to cast new light on his hypothesis of emotional needs in a
hierarchical representation. Both of these methods of seeing human needs complement
each other.
An additional hope and intent in offering the framework of STABLE© is that I
will use this model when designing curricula for outdoor and adventure education and in
the facilitation of retreats. In addition to mental health clinic or private practice settings, I
have found this need for containment, mirroring, and safety for emotional activation to be
the most optimal way to facilitate outdoor trips and wilderness therapy. This does not
mean that every participant on such trips will have an experience of emotional activation
from current or previous trauma, but it is well documented by organizations such as

50
Outward Bound and NOLS that forming, storming, norming, and performing occur in the
backcountry—storming being the operative concept connected with emotional activation
among adventure education participants (Jostad, Paisley, & Gookin, 2012, p. 24).

Chapter IV
Summary and Conclusions
Summary
In designing my thesis, there was a feeling tone I hoped to convey. My intent was
to incorporate a mythopoetic voice and a tone honoring the sacred feminine that could
emerge so that in the process of exploring the somatic release of trauma, a deeper quality
of soul could be revealed. Chapter II encapsulated many of the underlying key concepts
upon which somatic release and integration of trauma are based (Kerr & Bowen, 1988;
Johnson, 2013; Levine, 2010; Porges, 2011; Siegel, 2012; van der Kolk, 2014). I
explored 10 different modalities in the literature review to acknowledge some of the most
effective treatment methods for the release of somatically stored trauma (Bolesky, 2017;
Epstein, 2013; Konopatsch & Payne, 2012; Kurtz, 1990; Levine, 2010; Ogden & Fisher,
2015; Parnell, 2013; Siegel, 2012; Shapiro & Forrest, 2016; van der Kolk, 2014; Weiss et
al., 2015).
In Chapter III, seeing trauma as a continuum from micro traumas that slowly
accumulate, which can include relational trauma and attachment wounds, to macro
traumas was added to the definitions of trauma in Chapter II. There was also a focus on
the cumulative nature of trauma where incidents can build up over time (Crastnopol,
2015). Within the clinical findings, the concept of a sacred temenos and its clinical use to
honor patients and their symptoms in a strength-based way was highlighted. The acronym
STABLE© was introduced as a model for relating both internally and externally. Its
52
nonlinear and recursive nature add to the exploration of personal growth by offering a
foundation from which to work. The importance of shadow integration to the process of
healing trauma added to the allusion that experiencing trauma can be seen as an initiation
journey similar to that of the Sumerian goddess Inanna’s descent to the underworld to
emerge with greater wholeness (Perera, 1981). The recognition of wellbeing and
cultivating a relationship with the natural world were added to the conceptualization of
trauma work.
Suggestions for Further Research
I was not able to find studies or research articles on cumulative trauma or micro
trauma, as this seems to be an emerging subcategory of trauma on a continuum. I was
able to find one text that spoke to a psychoanalytic model for treating micro traumas
(Crastnopol, 2015). Cumulative and micro trauma could be an area of further research
that might assist therapists and health professionals as well as wilderness therapists in
treating their patients and clients. In addition, I did not come across any research studies
or scholarly articles on acupuncture and the treatment of cumulative trauma, emotional
regulation, affect regulation, or emotional stress. Further research in this area could be
very useful in the field of the somatic treatment of trauma.
Research could be done on what somatic modalities treat which kinds of trauma
on the continuum most effectively. I have begun to research this, but I was unable to find
comparative studies of how trauma is treated differently among the modalities explored
in this thesis and the multitudes of modalities that were not discussed in this thesis.
Acknowledging addiction as a method of coping with trauma symptoms and
cumulative trauma seems to be an area where greater focus on substance abuse could be

53
quite beneficial. This research could support the success rates for sobriety in treatment
centers, hospitals, and therapy practices by encouraging the therapists and other care
professionals to keep this connection in mind and might perhaps lead to an increase in
compassion for those who end up using substances in the process of attempting to come
to terms with their trauma. The next step in that process could be helping such clients and
patients to explore other methods of reducing overwhelm and learning to tolerate the
discomfort of life with greater self-love and increased self-care without the use of toxic
substances (Flores, 2004).
Exploring the effects of trauma on outdoor and adventure education participants
who display symptoms of dysregulation could be a fascinating way to expand trauma
research focusing on cumulative trauma and the entire spectrum of trauma with its effects
on human behavior in wilderness settings. This research could be factored in when
designing adventure education and wilderness therapy curricula and then utilized when
facilitating programs.
Conclusions
The body of this thesis is contained within the concept that trauma work of any
kind must begin with establishing safety by the therapist attuning to what the patient’s
definition of safety is. There is an opportunity for the therapist and client to cocreate a
sacred temenos to contain, deepen, and enrich the safety of delving into trauma work.
This synthesis of research aimed to add to the openness and inclusivity of trauma
research. Using myth as metaphor in trauma work can add soul, depth, and meaning to
this work both for practitioners and for patients, clients, and participants alike. There is
an opportunity to experience self-compassion through safety, trust, acceptance,

54
belonging, love, and a connection to Earth and ecopsychology for practitioners and those
they serve when embodying these truths. The co-occurrence of anxiety and depression
symptoms often results as a response to unresolved trauma. Each of the somatic
modalities presented in this thesis have beneficial and lasting effects on the reduction of
trauma symptoms and can add to greater levels of wellbeing. Conscious co-regulation
between therapists and clients can aid in stabilization and have positive ripple effects into
clients’ lives.
Appendix A
STABLE© Rainbow Drawing Used Clinically
Figure 5. Rainbow Drawing of STABLE©. Drawing by author, 2017

Appendix B
Using STABLE© to Address Client Dysregulation: A Clinical Example
The following is an amalgamation of experiences I facilitated in therapy sessions
to give an example of how I worked using the STABLE© acronym. Many of my clients
worked with me using belly breathing and EFT tapping. Thus, the anonymity of any
individual cases has been expressly protected, such that no personal identification is
presented.
“When people move beyond their windows of tolerance; they lose their capacity
to think” (Siegel, 2012, p. 305). An example of trauma having a profound effect on
everyday functioning occurred when I worked with a caregiver of a troubled child who
came in for a therapy session with me. The caregiver’s affect included hypervigilance,
pressured speech, and it was clear just being in my office caused the caregiver to leave
their window of tolerance. I knew that before I could be of any help to my child patient, I
needed to help regulate the child’s caregiver if this child had any chance of going home
with a greater sense of stability than when arriving at my office. I worked one on one
with the caregiver by slowing down the process and attuning with the caregiver’s energy.
I suspected the caregiver had a trauma history in witnessing the caregiver’s highly
dysregulated affect during the session. My primary role was to meet that affect with love,
compassion, and security. I held the knowing that this was a safe place and that the
caregiver’s survival was not threatened in the present moment because at that time the
caregiver could not hold that awareness steadily and needed my support in the form of
57
conscious co-regulation. We began to regulate together, my calming presence helped to
ground the caregiver and transform the office and clinic into a safe container, a temenos
of Safety, the first element of STABLE©.
Opening the door into Trust became evident through checking in to see if the
caregiver would be willing to do some breathing and EFT tapping with me. The caregiver
consented to try it. I sat in front of the caregiver and modelled belly breathing—
expanding my belly on the in-breath, placing my hand on my belly to exaggerate the air
expanding, and contracting my belly on the outbreath. Once the caregiver was able to
follow the in-breath and out-breath, I modeled tapping the top of my head and paired it
with following my breath. The caregiver tapped head, trunk, underarms, and hands in
sequence through mirroring what I demonstrated.
The caregiver opened into huge sobs, and a verbal outpouring of an extensive
trauma history ensued. In the midst of this the caregiver trembled and shook into tears of
happiness for the release and began to laugh. Levine (2010) wrote extensively about this
kind of body response as in and of itself having a regulating effect. The caregiver relayed
not having experienced that much joy in many years! By me listening to the caregiver’s
trauma narrative with openness, huge parts of the caregiver’s self were welcomed back
into Acceptance, the third aspect of STABLE©. “Feeling listened to and understood
changes our physiology; being able to articulate a complex feeling, and having our
feelings recognized, lights up our limbic brain and creates an ‘aha moment’” (van der
Kolk, 2014, p. 234). I gave verbal cues of the universality of shame, guilt, fear,
abandonment, and that the caregiver was a normal human being who had gone through
horrific experiences.

58
By me contributing validation and genuine caring to what the caregiver shared,
the caregiver stepped up the ladder of STABLE© into a felt sense of Belonging in the
world again. The caregiver experienced dignity and through being truly seen by a me as
therapist or in the role of a person in a position of some authority, the caregiver started to
feel safe again and articulated that transformation. Now the caregiver could live with
head raised from the downcast gaze focused solely on survival to join in a sense of
Belonging and be a part of society, a part of community. I offered something like,
“You’re safe now. In this moment, all is well.”
I have found reassuring statements to have a profound effect on regulating affect
when a patient is ready to release the tight hold of a trauma state—this has been true for
me on a personal level in transforming my somatic releases of trauma as well, so I
understand the process from the inside out. This kind of reassurance can often open a
client into a place where the energetic experience of Love is welcome.
With the caregiver, a heart resonance occurred between us by me remaining in a
state of neutral yet loving presence (Kurtz, 1990). The caregiver shifted from a state of
hypervigilance, where crisis was the normal response to life, to one remembering the
caregiver’s connection to nature, to self-care, and to life again. Although I did not speak
with the caregiver about the phases of STABLE©, the caregiver had gone through all
seven, into a state of seeing the self in symbols of nature—a state of ecopsychological
connection. When my primary patient returned to the room, the relationship between the
two of them changed; there was a noticeable lightness with a sense of possibility and
hope for the future. Our work had just begun.

References
Abram, D. (1996). The spell of the sensuous. New York, NY: Vintage Books.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders (5th ed.). Arlington, VA: Author.
Aron, E. (1996). The highly sensitive person: How to thrive when the world overwhelms
you. New York, NY: Harmony Books.
Aron, E. (2010). The undervalued self. New York, NY. Little, Brown.
Bolesky, K. (2004, June/July). Soma. Massage Bodywork Magazine. Retrieved from
http://www.massagetherapy.com/articles/index.php/article_id/715/Soma
Bolesky, K. (2017). Soma Neuromuscular Integration®. Retrieved from
http://www.soma-institute.org/
Bram, A. D., & Peebles, M. J. (2014). Psychological testing that matters: Creating a
roadmap for effective treatment. Washington DC: American Psychological
Association.
Brooks, J., & Walkenhorst, R. (Producers). (2014). Inner world: Somatic experiencing
[Video file]. Healing Quest TV. Rescue, CA: Lightbridge Media. Retrieved from:
https://www.youtube.com/watch?v=-Y9thBpfUDk
Brown, R., & Gerbarg, P. (2012). The healing power of the breath: Simple techniques to
reduce stress and anxiety, enhance concentration, and balance your emotions.
Boston, MA: Shambhala.
Caldwell, C. (2012). Sensation, movement, and emotion: Explicit procedures for implicit
memories. In S. Koch, T. Fuchs, M. Summa & C. Muller (Eds.), Advances in
consciousness research: Body, memory, metaphor and movement (pp. ??-??).
Amsterdam, Netherlands: John Benjamin.
Campbell, J. (with Moyers, B.). (1988). The power of myth (B. S. Flowers, Ed.). New
York, NY: Anchor Books.
Campbell, J. (2013). Goddesses: Mysteries of the feminine divine (S. Rossi, Ed). Novato,
CA: New World Library.
60
Chodorow, J. (1991). Dance therapy and depth psychology: The moving imagination.
New York, NY: Routledge.
Church, D., Piña, O., Reategui, C., & Brooks, A. (2012). Single session reduction of the
intensity of traumatic memories in abused adolescents after EFT: A randomized
controlled pilot study. Traumatology, 18(3), 73-79.
Coppin, J., & Nelson, E. (2005). The art of inquiry: A depth psychological perspective.
New York, NY: Spring Publications.
Crain, W. (2011). Theories of development: Concepts and applications (6th ed.). Upper
Saddle River: NJ: Pearson Prentice Hall.
Crastnopol, M. (2015). Micro-trauma: A psychoanalytic understanding of cumulative
psychic injury. New York, NY: Routledge.
Creswell, J. (2009). Research design: Qualitative, quantitative, and mixed methods
approaches (3rd ed.). Thousand Oaks, CA: Sage.
Dane, F. (2011). Evaluating research: Methodology for people who need to read
research. Thousand Oaks, CA: Sage.
Epstein, M. (2013). The trauma of everyday life. New York, NY: Penguin Books.
Estés, C. P. (1992). Women who run with the wolves. New York, NY: Ballantine Books.
Feinstein, D. (2008). Energy psychology: A review of the preliminary evidence.
Psychotherapy: Theory, Research, Practice, Training, 45, 199-213.
Feinstein, D., Eden, D., & Craig, G. (2005). The promise of energy psychology:
Revolutionary tools for dramatic personal change. New York, NY: Penguin.
Flores, P. (2004). Addiction as an attachment disorder. Lanham, MD: Jason Aronson.
Fogel, A. (2000). Developmental pathways in close relationships. Child Development,
71(5), 1150-1151.
Greene, R. (2014). Lost at school: Why our kids with behavioral challenges are falling
through the cracks and how we can help them. New York, NY: Scribner.
Harper, D. (2017). Sacred. In Online etymology dictionary. Retrieved from:
http://www.etymonline.com/index.php?term=sacred
Henderson, J. L. (2005). Thresholds of initiation. Wilmette, IL: Chiron.
Herman, J. (1997). Trauma and recovery: The aftermath of violence—From domestic
abuse to political terror. New York, NY: Basic Books.

61
Johnson, S. (2013). Love sense: The revolutionary new science of romantic relationships.
New York, NY: Little, Brown.
Jostad, J., Paisley, K., & Gookin, J. (2012). Wilderness-based semester learning:
Understanding the NOLS experience. Journal of Outdoor Recreation, Education,
and Leadership, 4(1), 16-26.
Judith, A. (2004). Eastern body, Western mind: Psychology and the Chakra system as a
path to the Self. New York, NY: Celestial Arts.
Jung, C. G. (1966). Appendix: The realities practical psychotherapy (R. F. C. Hull,
Trans.). In H. Read et al. (Eds.), The collected works of C. G. Jung (Vol. 16, 2nd
ed., pp. 327-339). Princeton, NJ: Princeton University Press. (Original work
published 1937)
Jung, C. G. (1970). Mysterium coniunctionis (R. F. C. Hull, Trans.) (H. Read et al., Eds.),
The collected works of C. G. Jung (Vol. 14). Princeton, NJ: Princeton University
Press. (Original work published 1956)
Kabat-Zinn, J. (2013). Full catastrophe living: Using the wisdom of your body and mind
to face stress, pain, and illness. New York, NY: Bantam Books.
Kerr, M., & Bowen, M. (1988). Family evaluation: The role of the family as an
emotional unit that governs individual behavior and development. New York,
NY: W. W. Norton.
Konopatsch, I., & Payne, H. (2012). The emergence of body memory in Authentic
Movement. In S. Koch, T. Fuchs, M. Summa & C. Muller (Eds.), Advances in
consciousness research: Body, memory, metaphor and movement (pp. ??-??).
Amsterdam, Netherlands: John Benjamin.
Kornfield, J. (1993). A path with heart: A guide through the perils and promises of
spiritual life. New York, NY: Bantam Books.
Kurtz, R. (1990). Body-centered psychotherapy: The Hakomi method. Mendocino, CA:
Life Rhythm.
Lee, R. (2007). Shame and belonging in childhood: The interaction between relationship
and neurobiological development in the early years of life. British Gestalt
Journal, 16(2), 1-13.
Levine, P. (2010). In an unspoken voice: How the body releases trauma and restores
goodness. Berkeley, CA: North Atlantic Books.
Maslow, A. H. (1943). A theory of human motivation. Psychological Review, 50(4),
370-397.

62
Maslow, A. H. (1954). Motivation and personality. New York, NY: Harper and Row.
McWilliams, N. (2011). Psychoanalytic diagnosis: Understanding personality in the
clinical process (Rev. ed.). New York, NY: Guilford Press.
Moore, T. (1992). Care of the soul: A guide for cultivating depth and sacredness in
everyday life. New York: NY: Harper Collins.
Moore, T. (2004). Dark nights of the soul: A guide to finding your way through life’s
ordeals. New York, NY: Gotham Books.
Morris, W. (2015). Transformation: Treating trauma with acupuncture and herbs.
Austin, TX: 33 Publishing.
Moustakas, C. (1994). Phenomenological research methods. Thousand Oaks, CA: Sage.
Ogden, P., & Fisher, J. (2015). Sensorimotor psychotherapy: Interventions for trauma
and attachment. New York, NY: W. W. Norton.
Ogden, P., Kekuni, M., & Pain, C. (2006). Trauma and the body: A sensorimotor
approach to psychotherapy. New York, NY: W. W. Norton.
O’Malley, M. (2011). Belonging to life: The journey of awakening. Seattle, WA:
Awaken.
Paris, G. (2016). Wisdom of the psyche: Beyond neuroscience. New York, NY:
Routledge.
Parnell, L. (2013). Attachment-focused EMDR: Healing relational trauma. New York,
NY: W. W. Norton.
Plotkin, B. (2003). Soulcraft: Crossing into the mysteries of nature and psyche. Novato,
CA: New World Library.
Plotkin, B. (2013). Wild mind: A field guide to the human psyche. Novato, CA: New
World Library.
Porges, S. (2011). The polyvagal theory: Neurophysiological foundations of emotions,
attachment, communication, self-regulation. New York, NY: W. W. Norton.
Porges, S., & Buczynski, R. (2014). The polyvagal theory for treating trauma. Retrieved
from: http://stephenporges.com/images/stephen%20porges%20interview
%20nicabm.pdf

63
Reeds, M. (2015). Mindfulness and trauma states. In H. Weiss, G. Johanson & L. Monda
(Eds.), Hakomi mindfulness-centered somatic psychotherapy: A comprehensive
guide to theory and practice (pp. ??-??). New York, NY: W. W. Norton.
Ronnberg, A. & Martin, K. (Eds). (2010). The book of symbols: Reflections on archetypal
images. Hohenzollerning, Koln, Germany: Taschen.
Roszak, T. (1992). Voices of the earth: An exploration of ecopsychology. Grand Rapids,
MI: Phanes Press.
Roszak, T., Gomes, M., & Kanner, A. (Eds.). (1995). Ecopsychology: Restoring the
earth, healing the mind. San Francisco, CA: Sierra Club Books.
Schwartz, R. (2008). You are the one you’ve been waiting for: Bringing courageous love
to intimate relationships. Oak Park, IL: The Center for Self-Leadership.
Schwartz, R. (2015). Foreword. In H. Weiss, G. Johanson & L. Monda (Eds.), Hakomi
mindfulness-centered somatic psychotherapy: A comprehensive guide to theory
and practice (pp. ??-??). New York, NY: W. W. Norton.
Selby, M. (2016, September). Psychopharmacology. Unpublished lecture presented in the
course, Course Name, at Pacifica Graduate Institute, Carpinteria, CA.
Shapiro, F., & Forrest, M. (2016). EMDR: The breakthrough therapy for overcoming
anxiety, stress, and trauma. New York, NY: Perseus Books.
Sharp, D. (1991). C. G. Jung lexicon: A primer of terms and concepts. Toronto, Canada:
Inner City Books.
Shepsut, A. (1993). Journey of the priestess: The priestess traditions of the ancient
world—A journey of spiritual awakening and empowerment. San Francisco, CA:
Aquarian Press.
Siegel, D. (2010). The mindful therapist: A clinician’s guide to mindsight and neural
integration. New York, NY: W. W. Norton.
Siegel, D. (2012). The developing mind: How relationships and the brain interact to
shape who we are. New York, NY: Guilford Press.
Siegel, D. (2013). Foreword. In L. Parnell, Attachment-focused EMDR: Healing
relational trauma (pp. xiii-xv). New York, NY: W. W. Norton.
Siegel, D., & Bryson, P. T. (2011). The whole brain child: 12 revolutionary strategies to
nurture your child’s developing mind. New York, NY: Bantam.

64
Soma. (2017). In English Oxford living dictionaries. Retrieved from
https://en.oxforddictionaries.com/definition/soma
Stolorow, R. (2008). The contextuality and existentiality of emotional trauma.
Psychoanalytic Dialogues, 18, 113-123.
Van der Kolk, B. (2011). Foreword. In S. Porges, The polyvagal theory:
Neurophysiological foundations of emotions, attachment, communication, self-
regulation (pp. xi-xvii). New York, NY: W. W. Norton.
Van der Kolk, B. (2014). The body keeps the score: Brain, mind, and body in the healing
of trauma. New York, NY: Penguin Books.
Van der Kolk, B. (2016, April 12). Trauma, attachment & neuroscience: Brain, mind &
body in the healing of trauma. Unpublished lecture given in Seattle, WA.
Weiss, H., Johanson, G., & Monda, L. (Eds.). (2015). Hakomi mindfulness-centered
somatic psychotherapy: A comprehensive guide to theory and practice. New
York, NY: W. W. Norton.
Whitehouse, M. (2007). C .G. Jung and dance therapy. In P. Pallaro (Ed.), Authentic
movement (pp. 73-101). Philadelphia, PA: Jessica Kingsley.
Wikman, M. (2004). Pregnant darkness: Alchemy and the rebirth of consciousness.
Berwick, ME: Nicolas-Hays.
Wilson, E. O. (2016, March 3). The global solution to extinction. New York Times.
Retrieved from: http://www.nytimes.com/2016/03/13/opinion/sunday/the-global-
solution-to-extinction.html?_r=0
Woodman, M., & Mellick, J. (2000). Coming home to myself: Reflections for nurturing a
woman’s body and soul. San Francisco, CA: Conari Press.