
International Journal of
Environmental Research
and Public Health
Article
The Effects of a Forest Therapy Programme on Mental
Hospital Patients with Affective and
Psychotic Disorders
Ernest Bielinis 1,* , Aneta Jaroszewska 2, Adrian Łukowski 3 and Norimasa Takayama 4
1 Department of Forestry and Forest Ecology, Faculty of Environmental Management and Agriculture,
University of Warmia and Mazury, Pl. Łódzki 2, 10-727 Olsztyn, Poland
2 Department of Psychiatry, University of Warmia and Mazury, Aleja Wojska Polskiego 35, 11-041 Olsztyn,
Poland; anetajaroszewska@tlen.pl
3 Faculty of Forestry, Poznan´ University of Life Sciences, Wojska Polskiego 71c, 60-625 Poznan´ , Poland;
adrian.lukowski@up.poznan.pl
4 Environmental Planning Laboratory, Department of Forest Management, Forestry and Forest Products
Research Institute in Japan, 1 Matsunosato, Tsukuba, Ibaraki 305-8687, Japan; hanri@ffpri.affrc.go.jp
* Correspondence: ernest.bielinis@uwm.edu.pl
Received: 6 November 2019; Accepted: 20 December 2019; Published: 23 December 2019
Abstract: The positive effect of forest bathing on the mental health and wellbeing of those suffering
from post-traumatic stress disorder or experiencing stress has been proven. It is not known, however,
how ‘forest therapy’ affects the mental health of people who are treated in a psychiatric hospital
for affective or psychotic disorders. Potentially, forest therapy could bring many benefits to these
people. To test the potential effectiveness of this therapy, a quasi-experiment was carried out in a
psychiatric hospital in Olsztyn (north Poland). In the summer and autumn of 2018, the patients of
the psychiatric hospital in Olsztyn participated in forest therapy interventions. The proposed forest
therapy consisted of participating in one hour and forty-five minutes walks under the supervision
of a therapist. Subjects filled out the Profile of Mood States Questionnaire (POMS) and the State
Trait Anxiety Inventory (STAI-S) before and after the study. In the case of a group of patients with
affective disorders, forest therapy had a positive effect on nearly all POMS scale subscales, with the
exception of the ‘anger–hostility’ subscale, which did not change its values significantly after the
intervention. In these patients, the greatest impacts were noted in the subscales ‘confusion’ and
‘depression–dejection’; the level of anxiety measured with the STAI-S scale also significantly decreased.
In the case of patients with psychotic disorders, the values of the ‘confusion’ and ‘vigour’ subscales
and the STAI-S scale exhibited the greatest changes. These changes were positive for the health of
patients. Regarding the ‘fatigue’ subscale, no significant changes were observed in patients with
psychotic disorders. The observed changes in psychological indicators in psychiatric hospital patients
with both kinds of disorders indicate that the intervention of forest therapy can positively affect their
mental health. The changes observed in psychological indicators were related to the characteristics of
the given disorder.
Keywords: depression; forest bathing; forest therapy; mental disorder; mental hospital inpatients;
psychosis; Shinrin-yoku
1. Introduction
Forest recreation is any activity conducted in a forest environment for pleasure and to refresh the
mental attitude of an individual [1]. One type of forest recreation meant to improve human health is
often called forest therapy, forest bathing or Shinrin-yoku, and is often used as an alternative method to
Int. J. Environ. Res. Public Health 2020, 17, 118; doi:10.3390/ijerph17010118
www.mdpi.com/journal/ijerph

Int. J. Environ. Res. Public Health 2020, 17, 118
2 of 10
treat many afflictions. Nevertheless, the effectiveness of forest recreation as a complementary therapy
for mental hospital inpatients has not yet been examined with a large sample size. Several studies
have confirmed that this therapy is effective for some psychiatric conditions, such as in the treatment
of depression and anxiety in patients with chronic stroke [2], in the cure of depression [3,4], and as
treatment for depression of alcoholics [5] and post-traumatic stress disorder [6]. The effect on a larger
sample of patients (more than 20) in a mental hospital, however, has not been examined in any studies
reported in the accessible literature (e.g., in [7] there were 20 patients involved, 10 per group).
Forest therapy is also helpful in coping with chronic widespread pain [8] and in lowering
blood pressure in hypertensive and high-normal patients [9,10]. Many non-clinical studies give
evidence that forest recreation for the purpose of health improvement may have a salutary influence
on participants from many countries. Studies conducted in Japan showed that staying in a forest
environment reduced negative symptoms of stress [11], induced cardiovascular relaxation [12], and
had an impact on physiological and psychological indices [13–17]. Studies from Taiwan also reported
that this intervention may be effective in stress reduction [18], as did studies conducted in South
Korea [19,20] and in Denmark [6]. The above examples indicate that forest recreation is an effective
remedy for many health problems in many countries and could be considered as a possible additional
therapy for mental diseases. Furthermore, other research has suggested that forest recreation may also
cause immunological stimulation or increase the number of cells involved in the body’s response to
cancer [21–24]. It is worth mentioning that also other forms of nature therapy are effective [25].
Many people in the world are affected by mental health problems [26]. This is costly and harmful
for societies and thus, interventions in this area are greatly needed. The development of additional
forms of therapy is therefore important. Based on this knowledge, it is necessary to assess the effectuality
of forest recreation on patients in mental hospitals. Previous studies [27] that have confirmed the
positive influence of forest recreation on indices of the physical and psychological health of psychiatric
inpatients suggest that negative symptoms of mental diseases may be reduced by such therapy. If this
is so, this activity could be helpful as an additional therapy in treating some mental health problems,
such as anxiety and depression. Alternatively, staying in an environment not appropriate for forest
therapy, such as a forest without a view and with a dense understory, could induce fear [28], which
is not a desired effect. For this reason, it is unclear whether or not forest recreation will induce a
therapeutic effect in mental hospital patients.
To determine if forest recreation can induce positive effects on mood and anxiety levels, a
pre-test–post-test design was used to assess the healing effect in two groups of patients: those with
affective disorders and those with psychotic disorders. A recreational walk in a suburban forest
near the mental hospital in the city of Olsztyn was applied as a form of forest therapy intervention.
Appropriate psychological questionnaires, the Profile of Mood States (POMS) and State-Trait Anxiety
Inventory (STAI), were administrated to assess any resulting health improvements. The results of
comparisons between pre- and post-test are herein described and discussed, and conclusions for forest
owners, foresters and therapists are also given.
The following research hypotheses were made in the study. For both groups of patients, with
affective disorders and with psychotic disorders:
- forest therapy will have a positive effect on mood (on the POMS scale subscales),
- forest therapy will have a positive effect on anxiety (STAI-S values).
2. Materials and Methods
2.1. Participants
Fifty patients from the Provincial Unit of Psychiatric Treatment in Olsztyn voluntarily participated
in this study. Patients were in the day-care hospital ward for reported mental health problems
confirmed by stuff. During a few-day stay in the hospital, the patients took medicines that were

Int. J. Environ. Res. Public Health 2020, 17, 118
3 of 10
appropriate to their medical conditions. The mean age of patients was 42.44 years (±13.23 SD); 27 were
female and 23 were male.
One of many therapeutic activities during these stays was participation in forest recreation in the
nearest suburban forest. Some patients could not attend the therapy due to poor health; for example,
patients with severe depression did not want to participate and those suffering hallucinations were
excluded. To balance the need to quickly perform the tests and the need to obtain reliable results, an
optimal sample size was used. Previous research indicates that a sample size of 12–16 participants is
sufficient to draw significant conclusions in forest therapy experiments [18,28], and thus the groups of
23 patients with psychotic disorders and 27 patients with affective disorders included in this study are
large enough to provide valuable information.
Patients were recruited according to strict criteria. Two factors determined the inclusion in the
study: belonging to one of the two disease criteria (patients with psychotic or affective disorders were
selected) and willingness to participate in the study. Participants were qualified for the examination by
a physician. Gender and age were not criteria for discrimination from the research. Patients were asked
for their willingness to participate in the study by the physician and a consent form had to be obtained.
The following inclusion and exclusion criteria were followed when selecting patients for the study.
Criteria for inclusion:
• at least two weeks of hospitalisation in a psychiatric ward
• psychotic disorders (mental disorders that cause abnormal thinking and perceptions, in this case:
schizophrenia) diagnosed by a specialist in the field of psychiatry (F20–F29) or affective disorders
(F30–F39) according to the International Classification of Diseases (ICD-10)
• consent to participate in the study.
Exclusion criteria:
• mental state that makes it impossible to leave the psychiatric ward
• movement disorders or other somatic diseases that prevent participation in the study.
2.2. Study site
The Provincial Unit of Psychiatric Treatment, which includes a mental hospital in its complex, is
located on the northern outskirts of the city of Olsztyn, in north-eastern Poland (GPS 20◦30’E 53◦47’N).
The hospital is in a part of the city that borders a suburban forest (Figure 1). The climate in Olsztyn is
temperate, mean annual temperature is 7.9 ◦C, mean annual precipitation is 635 mm and altitude is
139 m. The weather during days of forest recreation was fine, with an approximate temperature of
20–25 ◦C, without strong wind and without precipitation.
The area of the suburban forest is covered mainly by 65- to 180-year-old Scots pine (Pinus sylvestris
L.), with some 95- to 105-year-old Norway spruce (Picea abies (L.) H. Karst.) and 95- to 110-year-old
pedunculate oak (Quercus robur L.), and the occasional 15-year-old common beech (Fagus sylvatica L.).
Ground in this part of the suburban forest is covered with moss and herbaceous vegetation. All views
in the place selected for forest therapy showed forest, mainly undisturbed by buildings or other objects.
2.3. Procedure
Between August and September of 2018, patients of the mental hospital in Olsztyn participated
voluntarily in forest recreation interventions organised by medical staff at the hospital. On 12 different
occasions throughout the day (four to five patients per one forest therapy session), patients were
encouraged to participate in forest walks with additional exercises in the forest environment (walking,
stretching, watching landscapes). This intervention took place under the supervision of a qualified
therapist. Patients spent an hour and forty-five minutes in the forest during each forest recreation
programme. Patients participated in the therapy once, each time the therapy was organized around
noon. The first small group participated in the therapy on July 27th and the last group on November

Int. J. Environ. Res. Public Health 2020, 17, 118
4 of 10
29th. The number of patients in the hospital ward was small, so they could not communicate and
exchange experiences about the experiment at the time (patients who participated in the study stayed
in the hospital for a short time, hence they could not contact new patients and tell them about the
therapy). The walking route for forest recreation is shown in Figure 1. Before and after interventions,
psychological questionnaires were administrated to patients, allowing them to assess their perceived
feelings before and after the forest therapy. The questionnaires before and after interventions were
filled out in an indoor environment, in conference rooms in the hospital.
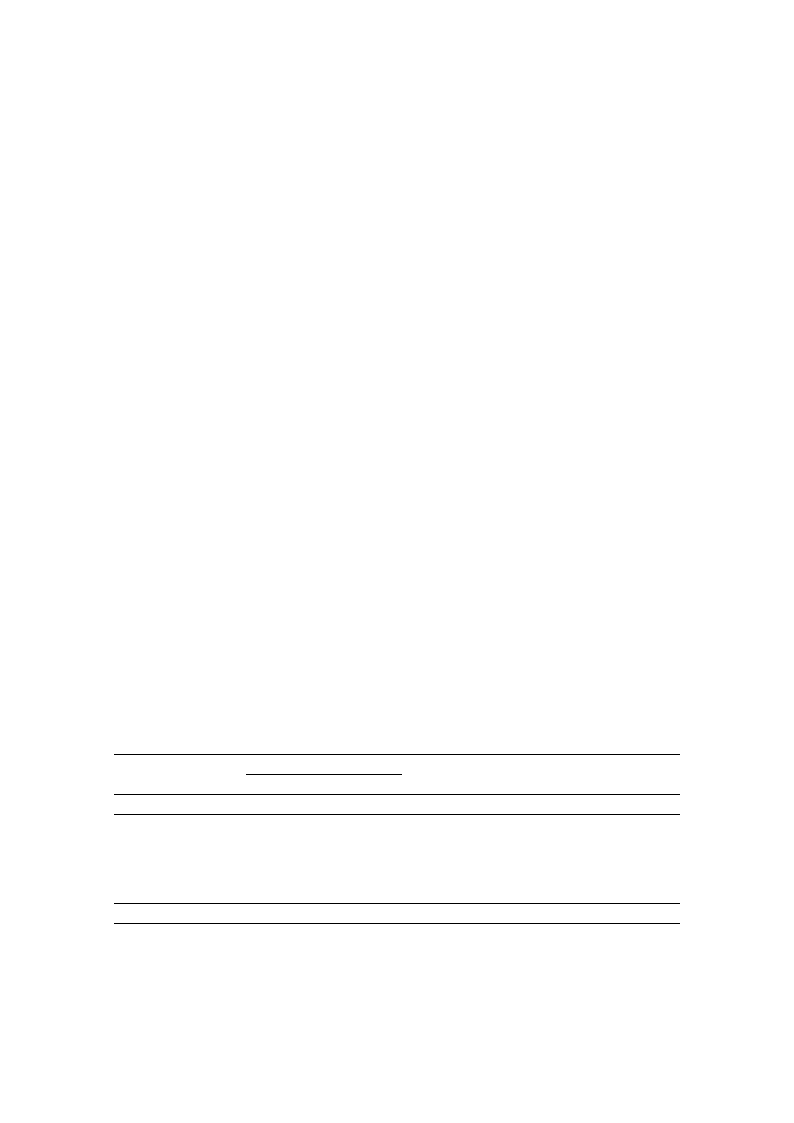
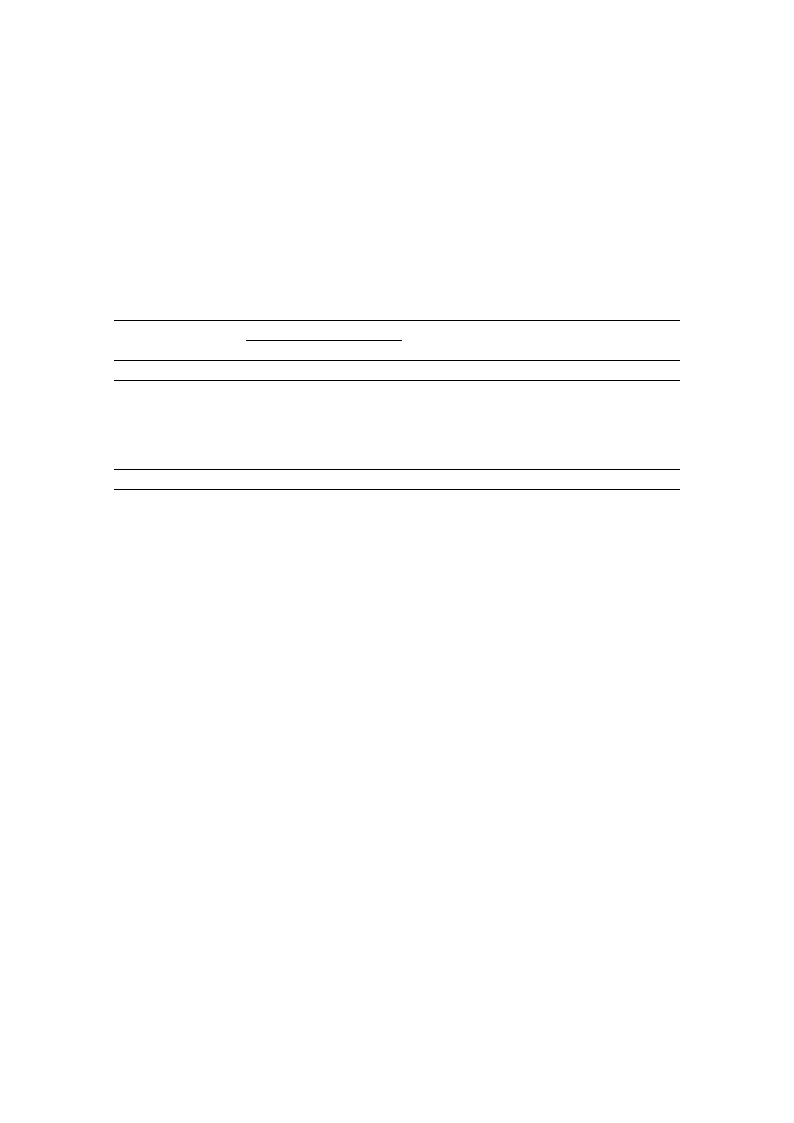
Figure 1. The route walked during a typical forest recreation programme at the Provincial Unit of
Psychiatric Treatment in Olsztyn, Poland.
2.4. Measurements
To measure the response of patients to the forest recreation intervention, two psychological
questionnaires were administrated before and after the intervention.
To assess the effect of forest therapy on emotional state, the Polish 65-item version of the Profile of
Mood States (POMS) questionnaire was chosen [29,30]. The POMS is a reliable and valid instrument
for assessing psychological distress [31], and has been used previously to estimate the influence of a
forest environment on mood states [32,33]. This questionnaire measures six mood states: confusion,
fatigue, anger–hostility, tension–anxiety, depression–dejection and vigour. A five-point Likert scale
was used for each item to evaluate participants’ mood states, with each item assessed from 0 (strongly
agree) to 4 (strongly disagree).
To measure the effect of forest recreation on levels of anxiety, the State-Trait Anxiety Inventory
(STAI) was used [34]. The original STAI questionnaire is composed of two parts (STAI-S and -T).
The STAI-S is meant to measure the level of anxiety in the present moment (20 items, state anxiety)
and the STAI-T is meant to measure anxiety levels as a personal characteristic (another 20 items).
For this research, the former was most appropriate and thus the Polish 20-item STAI-S was applied [35].
A four-point Likert scale, ranging from (1) strongly disagrees to (4) strongly agree, was used to evaluate
patients’ anxiety levels.
Int. J. Environ. Res. Public Health 2020, 17, 118
5 of 10
Both scales used are reliable and have been tested in terms of their usefulness in research regarding
forest therapy. Anxiety measurement in psychiatric hospital patients is very important, which is why
we chose to also apply the STAI-S questionnaire, despite the tension–anxiety subscale already included
in the POMS.
2.5. Data Analysis
All data were stored in Excel (Microsoft, Redmont, WA, USA), and mean values and standard
deviation (SD) values were also calculated using this programme. All further analysis was conducted
using SPSS Statistics Version 24 (IBM, Armonk, NY, USA). For comparison between pre-test and
post-test measurements, a paired sample t-test was applied and the Holm correction was used to adjust
p values. The effect size (ES) with Cohen’s d was also calculated. An ES value of approximately 0.2 was
described as a small effect, approximately 0.5 as a medium effect and approximately 0.8 as a large effect.
3. Results
3.1. Age and gender distribution
The study involved 18 women (average age = 44.88) with affective disorders and 9 women
(average age = 39.77) with psychotic disorders. Nine men (average age = 44.44) with affective disorders
and 14 men (average age = 39.71) with psychotic disorders also participated in the study.
3.2. Patients with Affective Disorders
Results of the paired sample t-test examining the psychological differences for patients with
affective disorders before (pre-test) and after (post-test) the forest recreation programme are presented
in Table 1. Following the forest recreation programme, there was a significant decline in four negative
mood states of the POMS scale: tension–anxiety (t = 4.51, p < 0.001), depression–dejection (t = 6.42,
p < 0.001), fatigue (t = 3.23, p = 0.006) and confusion (t = 8.82, p < 0.001). Furthermore, there was a
significant increase in vigour levels post-test in comparison to those levels before the test (t = −4.35,
p = 0.001). Regarding anxiety, patient levels showed a significant decrease post-test (t = 4.88, p < 0.001).
The level of the anger–hostility mood state did not change after the forest recreation programme
(t = 0.52, p = 0.605). In addition, in patients with affective disorders, the size of the effect was greatest
for two mood states of the POMS scale, confusion (ES = 3.46) and depression–dejection (ES = 2.51),
meaning that these two indicators were the most responsive to change.
Table 1. Effects of the forest recreation programme on mood states and anxiety of patients with
affective disorders.
Psychological Indices
Pre-test
Post-test
t
(Affective Patients)
Mean ± SD Mean ± SD
p
Rate of
Change (%)
ES
Mood State (POMS)
Tension-anxiety
1.58 ± 0.75
1.05 ± 0.8
4.51
<0.000 ***
−33.85%
1.77
Depression-dejection
1.8 ± 0.86
1.11 ± 0.69
6.42
<0.000 ***
−38.05%
2.52
Anger-hostility
0.89 ± 0.43 0.85 ± 0.45
0.52
0.605
−4.86%
0.21
Fatigue
1.59 ± 0,8
1.27 ± 0.6
3.23
0.006 **
−20.27%
1.27
Confusion
1.77 ± 0.56 0.97 ± 0.56
8.82
<0.000 ***
−45.21%
3.46
Vigor
1.46 ± 0.75 2.05 ± 0.69
−4.35
0.001 **
40.64%
1.71
Anxiety (STAI-S)
50.26 ± 13.91 39.19 ± 9.41
4.88
<0.000 ***
−22.03%
1.91
Note: POMS: Profile of Mood States; STAI-S: The State-Trait Anxiety Inventory, State Anxiety; ES: Effect Size;
** p < 0.01, *** p < 0.001; Holm correction was applied; n = 27.
3.3. Patients with Psychotic Disorders
Results of the paired sample t-test regarding the psychological differences for patients with
psychotic disorders pre- and post-test are presented in Table 2. After the programme, there was
Int. J. Environ. Res. Public Health 2020, 17, 118
6 of 10
a significant decrease in three negative mood states of the POMS scale: tension–anxiety (t = 3.04,
p = 0.018), depression–dejection (t = 3.44, p = 0.009), confusion (t = 4.72, p = 0.001) and anger-hostility
(t = 2.57, p = 0.035), and also STAI-S level significantly decreased (t = 5.68, p < 0.001). There was also a
significant increase in one positive mood state of POMS, vigour (t = 5.78, p < 0.000). Anxiety levels
in patients with psychotic disorders decreased significantly after the forest recreation programme
(t = 5.68, p < 0.001). The level of the mood state fatigue did not change under the influence of the forest
recreation programme. The size of the effect was greatest for vigour (ES = 2.46) and tension–anxiety (ES
= 2.42), indicating that these two characteristics were most affected by the forest recreation programme.
Table 2. Effects of the forest recreation programme on mood states and anxiety of patients with
psychotic disorders.
Psychological Indices
(Psychotic Patients)
Pre-Test
Mean ± SD
Post-Test
Mean ± SD
t
p
Rate of
Change (%)
ES
Mood State (POMS)
Tension-anxiety
1.76 ± 0.97 1.18 ± 0.57
3.04
0.018 *
−32.88%
1.3
Depression-dejection 1.46 ± 0.82 0.99 ± 0.52
3.44
0.009 **
−32.08%
1.47
Anger-hostility
1.19 ± 0.51 0.95 ± 0.38
2.57
0.035 *
−20.06%
1.1
Fatigue
1.47 ± 0.8
1.34 ± 0.52
0.85
0.404
−8.90%
0.36
Confusion
1.69 ± 0.71 0.98 ± 0.53
4.72
0.001 **
−41.91%
2.01
Vigor
1.53 ± 0.59 2.22 ± 0.45
−5.78
<0.000 ***
45.04%
2.46
Anxiety (STAI-S)
49.39 ± 9.08 38.57 ± 6.56
5.68
<0.000 ***
−21.91%
2.42
Note: POMS: Profile of Mood States; STAI-S: The State-Trait Anxiety Inventory, State Anxiety; ES: Effect Size; * p <
0.05. ** p < 0.01. *** p < 0.001; Holm correction was applied; n = 23.
4. Discussion
4.1. Patients with Affective Disorders
This study indicated that a programme of forest recreation lasting one hour and forty-five minutes
has had a positive influence on the psychological health of patients with affective disorders, which
confirms other studies [2–6,8,9]. This intervention worked as healing therapy, with patients reporting
significantly lower levels of four negative aspects of mood measured by the POMS questionnaire:
tension–anxiety, depression–dejection, fatigue and confusion. Only one negative aspect of mood,
anger–hostility, showed no significant change between pre- and post-test. Vigour, an indicator of
positive mood, increased significantly after the intervention. Anxiety levels, measured using the
STAI-S questionnaire, significantly decreased. These findings are consistent with studies that tested
the effect of forest therapy on healthy Polish young adults [31,36] and found that some indicators of
negative mood decreased after exposure to a forest environment. These findings are in opposition to
those described in the work of Bielinis et al. [31], in which healthy Polish young adults were tested and
only one negative mood indicator, fatigue, increased significantly (mean pre-test = 1.61; mean post-test
= 0.80). In the current study, fatigue actually decreased (mean pre-test = 1.59; mean post-test = 1.27),
suggesting that the reactions of healthy adults and non-healthy adults may differ. In affective inpatients,
perhaps fatigue is difficult to change via a forest recreation programme, whereas in healthy adults, it is
more variable. In another study by Bielinis et al. [36], changes in fatigue levels of working or studying
healthy young adults were only marginally nonsignificant (p = 0.084, large effect size) and decreased
after exposure to a forest environment (mean pre-test = 1.22; mean post-test = 0.81), supporting this
suggestion. In other studies, in which psychiatric inpatients were examined, no significant effects of
forest therapy on mood states were found, but in these studies lower numbers of participants were
tested (10 patients in experimental group and 10 in control group). In these studies, levels of cortisol
and levels of depression measured using the Beck Depression Inventory were significantly lower in
inpatients after forest therapy [7], indicating observable positive mental health changes.

Int. J. Environ. Res. Public Health 2020, 17, 118
7 of 10
Anxiety levels measured using the STAI-S questionnaire significantly decreased after the forest
recreation programme (mean pre-test = 49.39, mean post-test = 38.57), but remained higher than those
of healthy participants in a similar investigation (mean pre-test = 30.19, mean post-test = 25.44) [18].
These results may not be excellent, but they do provide good information for practitioners, as they
indicate that an intervention of approximately one hour and forty-five minutes of forest recreation may
occasionally decrease the anxiety of inpatients. This may provide a good background for additional
psychotherapy, in which a lower level of anxiety is helpful. As other studies confirmed, forest therapy
may be effective [2,4,5].
4.2. Patients with Psychotic Disorders
The one hour and forty-five minutes forest recreation programme significantly decreased four
indicators of negative mood states: tension–anxiety, depression–dejection, anger–hostility and
confusion. Fatigue, however, did not show significant change in response to the forest recreation
programme. For patients with psychotic disorders with symptoms that include a high level of fatigue
(pre-test means for psychotic patients = 1.47, affective patients = 1.59, healthy individuals = 1.22 [36]),
this fatigue may not be easily reduced by any kind of additive therapy, suggesting that one symptom of
schizophrenia, measured by fatigue, is likely difficult to change through forest therapy. Other important
symptoms of schizophrenia, however, such as high levels of anxiety (pre-test means for psychotic
patients = 1.76, affective patients = 1.58, healthy individuals = 0.90 [36]), may be significantly reduced
in these patients, which is valuable information for practitioners. The level of anxiety measured
using the STAI-S questionnaire was also lower (STAI-S score nearly 22% lower after forest therapy).
Additionally, level of vigour increased after therapy (by 45%) and, in contrast to patients with affective
disorders, anger–hostility significantly decreased. In other studies, the effect on psychotic symptoms
was also observable [7].
Once the abovementioned parameters decreased or increased after therapy, the new levels were
close to those of healthy individuals in other research [31]. The optimal levels of these psychological
parameters are important for patient health and are negatively related to symptoms of schizophrenia,
which may be ameliorated by a forest environment. In other research, some forms of physical
activity decreased these negative symptoms [37]. This is related to forest therapy, because one of
its elements is movement. Thus, forest therapy intervention may successfully stabilise the mood
and anxiety levels of patients with psychotic disorders. This is valuable information for therapists,
doctors and other practitioners, and forest therapy could perhaps be conducted as an occasionally,
complementary therapy in psychosis, despite appearing counterintuitive. Before conducting forest
therapy interventions, the authors of this research hypothesised that interactions between patients
with psychosis and a forest environment might increase negative symptoms, but the opposite occurred
here, as in other studies [7]. This is a positive outcome that should be tested in other experiments.
Additionally, other physiological indices (e.g., fMRI scans, biomarkers examinations in the blood)
should be measured to further investigate the real, physiological effects of forest therapy on patients
with psychosis. Any further information concerning this potentially extraordinary therapy will be
most useful, as it appears to effectively aid patients.
4.3. Limitations
There are some limitations to the study described in the article. Participants in the study were
of different sexes, but this factor was not included in the analysis. This will be possible in future
planned, randomized controlled studies. Another limitation in this work is the fact that in the study,
the researchers did not record how much of a given medical drug a particular patient took, therefore,
this factor could not be used as a covariate in the analysis. In future studies (this one can be considered
as a pilot test), the authors will consider this factor in randomized trials. The other limitation is
the quasi-experimental study design, without a planned control group (without control in which
participants would, for example, only participate outside the hospital, but not in the forest, just like

Int. J. Environ. Res. Public Health 2020, 17, 118
8 of 10
the experimental group). Thus, although pre- and post-effects were observed, whether they are due
to expectation (e.g., placebo effect) or true effects could not be discerned. This problem should be
resolved in further studies on this topic. The other limitation is the conducted analysis. There was no
control for potential confounders. Thus, any effects observed could be due to confounding factors
instead of treatment effects. This problem will be solved in subsequent experiments in which the level
of additional variables will be measured and analyzed. Also, it would be interesting to check whether
patients who show some kind of preferences for the forest environment will also achieve greater
benefits from forest therapy (according to the logic: the better they like the forest, the better the forest
works on them, according to the results of work, in which factors responsible for the prediction of the
positive impact of garden therapy on the subjects were described [38]). Unfortunately, this study did
not test this, which is another limitation, but it suggests direction of future activities for other scientists
in this area. Another limitation is the fact that there was no control group in the study. This problem
will be eliminated in future, randomized controlled trials. Unfortunately, in the study, the authors did
not know exactly how many patients there were in the ward, so it was difficult to calculate what was
the reliability of the sample in this study, so it was considered as one of the limitation. It is only known
that strictly new patients were involved in the experiment, and those who did not want to participate
remained in the ward.
5. Conclusions
In the case of a group of patients with:
(1) affective disorders
-
forest therapy had a positive effect on nearly all POMS scale subscales, with the exception
of anger–hostility,
-
confusion and depression–dejection were significantly decreased,
-
the level of anxiety measured with the STAI-S scale significantly decreased.
(2) psychotic disorders
-
the confusion and vigour subscales and the STAI-S scale showed the greatest change,
-
in the case of the fatigue subscale, no significant changes were observed in patients with
psychotic disorders.
The observed changes in psychological indicators in psychiatric hospital patients indicate that
the intervention of forest therapy may positively affect their mental health. Varying reactions were
also observed depending on the group of diseases a patient experienced. In the case of people with
psychotic disorders, the greatest effect of therapy was observed regarding vigour, whereas in the case
of patients with affective disorders, the largest reactions were observed in relation to the confusion
and depression–dejection traits. Changes in psychological indicators are therefore appropriate to
the characteristics of a given disorder. This is valuable information for therapists, doctors and
other practitioners.
Author Contributions: E.B. and A.J. conceived and designed the experiment, conducted data analysis, and
prepared the first version of the manuscript. A.Ł. consulted on experimental design, as well as reviewing and
editing the manuscript. N.T. contributed to publication by reviewing and editing the manuscript and giving
methodological advices. All authors have read and agreed to the published version of the manuscript.
Funding: This research received financial support for the manuscript’s publication from Faculty of Forestry at
the University of Life Sciences in Poznan´ . The publication is co-financed within the framework of Ministry of
Science and Higher Education program as "Regional Initiative Excellence" in years 2019-2022, project number
005/RID/2018/19.
Acknowledgments: We would like to thank the Faculty of Forestry at the University of Life Sciences in Poznan´
for organizing financial support for the manuscript’s publication.
Conflicts of Interest: The authors declare no conflict of interest.

Int. J. Environ. Res. Public Health 2020, 17, 118
9 of 10
Ethic Approval: The ethical code of commission of ethic in research of University of Warmia and Mazury in
Olsztyn (Ethic Review Board) for these research is 6/2018.
References
1. Douglas, R.W. Forest Recreation, 3rd ed.; Pergamon Press: New York, USA, 1982; p. 336. ISBN 9781483148267.
2. Chun, M.H.; Chang, M.C.; Lee, S.J. The effects of forest therapy on depression and anxiety in patients with
chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [CrossRef] [PubMed]
3. Lee, I.; Choi, H.; Bang, K.S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms
among adults: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 1–18. [CrossRef] [PubMed]
4. Woo, J.M.; Park, S.M.; Lim, S.K.; Kim, W. Synergistic effect of forest environment and therapeutic program
for the treatment of depression. J. Korean Soc. Forest Sci. 2012, 101, 677–685.
5. Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ.
Health. Prev. Med. 2012, 17, 73–76. [CrossRef]
6. Poulsen, D.V.; Stigsdotter, U.K.; Djernis, D.; Sidenius, U. ‘Everything just seems much more right in nature’:
How veterans with post-traumatic stress disorder experience nature-based activities in a forest therapy
garden. Health Psychol. Open 2016, 3, 1–14. [CrossRef] [PubMed]
7. Kim, M.H.; Wi, A.J.; Yoon, B.S.; Shim, B.S.; Han, Y.H.; Oh, E.M.; An, K.W. The influence of forest experience
program on physiological and psychological states in psychiatric inpatients. J. Korean Soc. Forest Sci. 2015,
104, 133–139. [CrossRef]
8. Han, J.W.; Choi, H.; Jeon, Y.H.; Yoon, C.H.; Woo, J.M.; Kim, W. The effects of forest therapy on coping
with chronic widespread pain: Physiological and psychological differences between participants in a forest
therapy program and a control group. Int. J. Environ. Res. Public Health 2016, 13, 1–13. [CrossRef] [PubMed]
9. Sung, J.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “forest
therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive
patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [CrossRef]
10. Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.;
et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal
blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [CrossRef]
11. Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.;
Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing,
walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [CrossRef]
12. Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.;
Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid.-Based Compl.
Alt. 2014, 2014, 834360. [CrossRef] [PubMed]
13. Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y.
Physiological and psychological effects of a forest therapy program on middle-aged females. Int. J. Environ.
Res. Public Health 2015, 12, 15222–15232. [CrossRef] [PubMed]
14. Takayama, N.; Saito, K.; Fujiwara, A.; Tsutsui, S. Influence of Five-day Suburban Forest Stay on Stress Coping,
Resilience, and Mood States. J. Environ. Inform. Sci. 2018, 2017, 49–57.
15. Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Morikawa, T.; Kagawa, T.; Miyazaki, Y. Physiological effects of forest
recreation in a young conifer forest in Hinokage Town, Japan. Silva Fenn. 2009, 43, 291–301. [CrossRef]
16. Li, Q.; Kawada, T. Effect of forest therapy on the human psycho-neuro-endocrino-immune network. Jap. J.
Hyg. 2011, 66, 645–650. [CrossRef]
17. Li, Q.; Otsuka, T.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Li, Y.; Hirata, K.;
Shimizu, T.; et al. Acute effects of walking in forest environments on cardiovascular and metabolic parameters.
Eur. J. Appl. Physiol. 2011, 111, 2845–2853. [CrossRef]
18. Chen, H.-T.; Yu, C.-P.; Lee, H.-Y. The Effects of Forest Bathing on Stress Recovery: Evidence from Middle-Aged
Females of Taiwan. Forests 2018, 403, 1–9. [CrossRef]
19. Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female
workers’ stress. Urban For. Urban Gree. 2015, 14, 274–281. [CrossRef]
20. Shin, W.S.; Yeoun, P.S.; Yoo, R.W.; Shin, C.S. Forest experience and psychological health benefits: the state of
the art and future prospect in Korea. Environ. Health Prev. 2010, 15, 38. [CrossRef]

Int. J. Environ. Res. Public Health 2020, 17, 118
10 of 10
21. Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.;
Wakayama, Y.; et al. Visiting a forest, but not a city, increases human natural killer activity and expression of
anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [CrossRef]
22. Li, Q.; Kobayashi, M.; Inagaki, H.; Hirata, Y.; Li, Y.J.; Hirata, K.; Suzuki, H.; Katsumata, M.; Wakayama, Y.;
Kawada, T.; et al. A day trip to a forest park increases human natural killer activity and the expression of
anti-cancer proteins in male subjects. J. Biol. Regul. Homeost. Agents 2010, 24, 157–165. [PubMed]
23. Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.J.;
Wakayama, Y.; et al. A forest bathing trip increases human natural killer activity and expression of anti-
cancer proteins in female subjects. J. Biol. Regul. Homeost. Agents 2008, 22, 45–55. [PubMed]
24. Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17.
[CrossRef] [PubMed]
25. Ng, K.; Sia, A.; Ng, M.; Tan, C.; Chan, H.; Tan, C.; Rawtaer, I.; Feng, L.; Mahendran, R.; Larbi, A.; et al. Effects
of Horticultural Therapy on Asian Older Adults: A Randomized Controlled Trial. Int. J. Environ. Res. Public
Health 2018, 15, 1705. [CrossRef] [PubMed]
26. Saxena, S.; Funk, M.K.; Chisholm, D. Comprehensive mental health action plan 2013–2020. E. Mediterr.
Health J. 2015, 21, 461–463. [CrossRef]
27. Gatersleben, B.; Andrews, M. When walking in nature is not restorative—The role of prospect and refuge.
Health Place 2013, 20, 91–101. [CrossRef]
28. Takayama, N.; Saito, H.; Fujiwara, A.; Horiuchi, M. The effect of slight thinning of managed coniferous forest
on landscape appreciation and psychological restoration. Prog. Earth Planet. Sci. 2017, 4, 1–15. [CrossRef]
29. Dudek, B.; Koniarek, J. The adaptation of Profile of Mood States (POMS) by D.M. McNair, M. Lorr L.F.
Droppelman. Przegla˛d Psychologiczny 1987, 30, 753–762. (In Polish)
30. McNair, D.M.; Maurice, L. An analysis of mood in neurotics. J. Abnorm. Soc. Psychol. 1964, 69, 620–627.
[CrossRef]
31. Bielinis, E.; Takayama, N.; Boiko, S.; Omelan, A.; Bielinis, L. The effect of winter forest bathing on psychological
relaxation of young Polish adults. Urban For. Urban Gree. 2018, 29, 276–283. [CrossRef]
32. Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological
and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [CrossRef]
[PubMed]
33. Takayama, N.; Korpela, K.; Lee, J.; Morikawa, T.; Tsunetsugu, Y.; Park, B.J.; Li, Q.; Tyrväinen, L.; Miyazaki, Y.;
Kagawa, T. Emotional, restorative and vitalizing effects of forest and urban environments at four sites in
Japan. Int. J. Environ. Res. Public Health 2014, 11, 7207–7230. [CrossRef] [PubMed]
34. Spielberger, C.D. Manual for the State-Trait. Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA,
USA, 1983.
35. Sosnowski, T.; Wrzesniewski, K. Research with the Polish form of the State-Trait Anxiety Inventory. In
Cross-Cultural Anxiety; Spielberger, C.D., Diaz-Guerrero, R., Eds.; Hemisphere/Harper & Row: New York,
NY, USA, 1986; Volume 3, pp. 21–35.
36. Bielinis, E.; Bielinis, L.; Krupin´ ska-Szeluga, S.; Łukowski, A.; Takayama, N. The Effects of a Short Forest
Recreation Program on Physiological and Psychological Relaxation in Young Polish Adults. Forests 2019, 10,
34. [CrossRef]
37. Beebe, L.H.; Tian, L.; Morris, N.; Goodwin, A.; Allen, S.S.; Kuldau, J. Effects of exercise on mental and physical
health parameters of persons with schizophrenia. Issues Ment. Health N. 2005, 26, 661–676. [CrossRef]
[PubMed]
38. Cervinka, R.; Schwab, M.; Schönbauer, R.; Hämmerle, I.; Pirgie, L.; Sudkamp, J. My garden–my mate?
Perceived restorativeness of private gardens and its predictors. Urban For. Urban Green. 2016, 16, 182–187.
[CrossRef]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access
article distributed under the terms and conditions of the Creative Commons Attribution
(CC BY) license (http://creativecommons.org/licenses/by/4.0/).