

A Portfolio of Research Work
Including an investigation into motherhood
experiences using content analysis.
By Lisa Corbett
Submitted to the University of Surrey for the partial fulfilment
of the degree of Practitioner Doctorate (PsychD) in
Psychotherapeutic and Counselling Psychology
School of Psychology
University of Surrey
July 2015
1

Statement of Copyright
No aspect of this portfolio may be reproduced in any form without the written
permission of the author, with the exception of the librarian of the University of
Surrey, who is empowered to reproduce the portfolio by photocopy or otherwise
and lend copies to those institutions or persons who require them for academic
purposes.
© Lisa Corbett 2015
2

Statement of Anonymity
To preserve the confidentiality and anonymity of clients, research participants
and professionals, pseudonyms have been used and all identifying information
has been changed or omitted through the portfolio.
3

Acknowledgements
I would like to thank the course team, professional tutors and administrative
staff, and in particular Dr. Martin Milton, who provided me with much
appreciated support and motivation during his time on the course.
For my clinical supervisors on each placement, I am so grateful for the support
and encouragement I received from you, and the diverse wealth of knowledge
that you allowed me to tap into.
I would like to thank my clients and research participants for sharing their
experiences with me, trusting me with their stories, and allowing us to learn
together.
Special acknowledgements go to my therapist. The work we did was integral to
my development both as a professional and as a person. I highly value having
had the opportunity to work with someone who provided such an honest,
challenging, but containing space for me.
I would like to thank my husband, for his enduring understanding and support
throughout this process, and my two wonderful children, Alexander and Amélie,
who have arrived since this course began, and motivate me and distract me in
equal measure.
And finally, I dedicate this portfolio to my Dad, who would have been so proud
to see me come to the end of this course. His unwavering belief in me
throughout my life is perhaps my strongest motivator, and I thank him for his
generous spirit and wicked sense of humour, missed now more than ever.
4

Contents
Abstract
p.6
Introduction to the Research Dossier
p.7
Literature review: Breaking the Cycle: Could Ecopsychology
and Existential Therapy be Useful Approaches to Trauma Therapy?
Research report one: The Client Experience of Existential
Therapy: An Investigation into the Experience of Existential Therapy
for a Client using Interpretative Phenomenological Analysis
Research report two: The final chapter in the book of growing up:
a content analysis of motherhood experiences
p.8
p.48
p.85
5
Abstract
This portfolio was submitted to the University of Surrey for the completion of the
Practitioner Doctorate in Psychotherapeutic and Counselling Psychology. The
research dossier contains a literature review about ecopsychology and
existential therapy as approaches for trauma, followed by two empirical studies
using qualitative methodologies. The first study uses Interpretative
Phenomenological Analysis to explore the client experience of existential
therapy, while the second study explores how the existential dimensions
manifest when women talk about becoming mothers for the first time. This was
achieved through Content Analysis.
6

Introduction to the Research Dossier
The Research Dossier consists of a literature review and two pieces of qualitative research. The
first report presented was a literature review which aimed to explore how ecopsychology and
existential therapy could be used as approaches to trauma. Through conducting this work, it
appeared that areas of knowledge appeared to be lacking substantial research. With this in
mind, it was decided that it would be beneficial to focus on one such area lacking in research,
and conduct an empirical study to investigate the client experience of existential therapy. My
second year research project explored the clients’ subjective experience of existential therapy
using Interpretative Phenomenological Analysis to analyse the data. A further empirical study
also took existential therapy as a focus, but this time explored the ways in which the existential
dimensions appear in accounts of individuals who have experienced motherhood using
qualitative Content Analysis.
Within my clinical practice, my research into existential therapy has emphasised for me a
requirement to allow an individual's experience to unfold without constricting a person strictly to
one model. While I was reliant on theory initially, I have found over time that I have developed a
more open-minded curious stance during assessment and formulation, bringing in theory when
required rather than from the outset. My research has prompted me to consider my stance on
the diagnosis, and raised thoughts for me about how I can balance working within the medical
model while prioritising the subjective experience of the client. I have found myself considering
the existential dimensions at times when working with clients, and believe this gave me an
opportunity to gain a richer insight into a client's experience. The ecopsychological concepts
explored also pervade in my clinical work, and I still routinely use some of the practices outlined
in my literature review both professionally and personally.
7

Breaking the Cycle: Could Ecopsychology and Existential Therapy be Useful
Approaches to Trauma Therapy?
Lisa Corbett, Supervised by Martin Milton
Abstract
Literature has suggested that the cyclical nature of psychological trauma can cause enduring
long-term effects on individuals and those around them. This review examines the effects of
psychological trauma and its relationship with ecopsychology and existential therapy. Despite
being relatively unexplored with regards to psychological trauma, empirical evidence is
beginning to amass for these approaches. Some contributions are considered along with their
limitations and empirical challenges. Speculative practical and therapeutic implications for
counselling psychology are identified and relevant future research is suggested.
Keywords: ecopsychology; existential therapy; psychological trauma; posttraumatic stress
disorder; nature
8

Breaking the Cycle: Could Ecopsychology and Existential Therapy be Useful
Approaches to Trauma Therapy?
Introduction
A traumatic incident is a shocking and emotionally overwhelming situation in which an individual
experiences or perceives a threat to the physical and/or psychological integrity of self or others,
resulting in a reaction of intense fear, helplessness or horror (American Psychiatric Association
[APA], 2000; Rothschild, 2000). It has long been evident that such experiences can cause
psychological problems, with perhaps the first cataloguing of traumatic symptoms documented
on Sumerian cuneiform tablets of 2100 BCE following deaths in battle (Ben Ezra, 2001, Grey
2007). More recently, acts of terrorism such as the attacks in the United States on September 11
2001 and widespread natural disasters such as the tsunami in Southeast Asia in 2004, have
been increasingly formulated through the perspective of trauma by professionals and the media
(Courtois & Gold, 2009). Indeed, trauma is increasingly being recognised not as a specialised
area, but a fundamental aspect of human experience (Gold, 2008).
This paper begins by addressing some responses to traumatic events and the effects of
traumatisation documented within the literature, before briefly outlining the key features of
posttraumatic stress disorder (PTSD) and compiling some of the current therapeutic options for
trauma therapy. Stolorow (2007), took a personal and philosophical reflection on the
psychological and emotional impact of trauma, defining it as ‘an experience of unbearable affect’
in a context in which there is an ‘absence of adequate attunement and responsiveness to the
[individual’s] painful emotional reactions’ (pp.9-10). Traumatisation can be subdivided into
primary, secondary, vicarious and trans-generational trauma (Lodrick, 2007). Those subjected
to primary trauma are present when the traumatic incident occurs; secondary trauma can occur
to those who witness the aftermath of a traumatic incident; vicarious trauma concerns people
who hear about traumatic incidents; and trans-generational trauma describes the traumatic
symptomatology displayed by the descendants of trauma survivors (Lodrick, 2007), as
exemplified for instance by the second generation of Holocaust survivors (e.g. Solomon et al.
1988).
Reactions to traumatic events vary considerably, ranging from relatively mild, creating minor
disruptions in the person’s life, to severe and debilitating. It is common for people to experience
anxiety, terror, shock, and upset, as well as emotional numbness and personal or social
disconnection. Nightmares of the traumatic event are common, as is depression (ISTSS, 2003).
9

The Diagnostic and Statistical Manual of Mental Disorders (DSM-IV APA, 2000) outlines
posttraumatic stress disorder (PTSD) as the development of characteristic symptoms of distress
or impairment that are present for over one month after exposure to trauma. Banyard (1999)
described its cyclical nature, outlining three main clusters of symptoms: re-experiencing
phenomena, avoidance/numbing and increased arousal. The DSM-V (APA, 2013) has revised
the diagnostic criteria by firstly moving PTSD from the Anxiety Disorders into a new category,
Trauma and Stressor-Related Disorders, and reorganised and renamed symptom clusters.
However, initial research has suggested that the revisions do not appear to adjust the
prevalence of PTSD (Miller et. al, 2013) and it would appear that the diagnostic review is
ongoing. Marx and Gutner (2015) report that the 11th edition of the International Classification of
Diseases (ICD-11) proposes to determine a diagnosis of PTSD through a combination of PTSD
symptoms falling under three categories: reexperiencing symptoms; avoidance symptoms, and
symptoms of heightened threat (Maercker et al., 2013). Additionally, while diagnosis ultimately
has a use and purpose, it can also be argued that this framework is also inherently limiting (Foa
et al., 2008). It has been proposed that PTSD is not a neutral term, but a social construction
(Maddux et al., 2004, cited in Joseph 2010) that may inadvertently pathologise normal and
natural reactions to traumatic events. Joseph (2010) also states that the very diagnosis of PTSD
and the medicalisation of trauma reactions essentially deny the existential nature of such
responses and stifle people's ability to emotionally process their experiences in meaningful and
purposive ways.
A Repetitive Cycle
‘Traumatised people lead traumatic and traumatizing lives’ (van der Kolk & McFarlane, 1996,
p.11). Themes of repetition are central: the individual is subjected to intrusive replays of the
original trauma (Lodrick, 2007). Trauma re-enactments are common and take the forms of re-
victimization, self-injurious and self-harming behaviours and externalizing the trauma by
victimizing others (van der Kolk & McFarlane, 1996).
Totten (2005) writes that traumatic experiences in childhood can have enduring profound effects
on traumatic experiences as an adult; influencing their responses and creating patterns of
hyperarousal or dissociation; together with a tendency to re-enact traumatic experiences (Perry
et al., 1995; Schore, 2000). Wainrib (2006) argues that traumatic events can generate severe
psychological reactions that can manifest anytime. For some, the effects last throughout their
remaining lifetimes and traumatised individuals have been found to have elevated rates of
psychiatric disorders including major depression and alcohol or drug dependence (Wainrib,
2006). The negative impact of trauma extends beyond psychiatric morbidity and encompasses
10

multiple dimensions including functioning, quality of life and physical health (ISTSS, 2004).
Approaches to therapy
The National Institute of Clinical Excellence (NICE) guidelines advocate a course of trauma-
focused psychological treatment (cognitive behavioural therapy [CBT] or eye movement
desensitisation and reprocessing [EMDR]) for PTSD. While research appears to demonstrate
their efficacy (e.g. Moss, 2009), demand for evidence-based-practice has focused on
quantitative studies that address a finite number of parameters and struggle to examine
complex interactions (Coote et al, 2004). Limitations such as attrition have been identified to
suggest that evidence is frequently overstated or under explained (Foa et al., 2008). Follette
and Ruzek (2006) argued that many CBT clinicians do not have adequate training, while
Courtois and Gold (2009) drew attention to a disparity between the need for professionals with
expertise in psychological trauma and the availability of these services. Despite a solid base of
scientific literature on trauma, this area has yet to be incorporated into the core curriculum of
graduate training in psychology and other professions (Courtois, 2002). Research indicates that
victims of trauma usually turn first to medical providers, yet many have apparently little or no
knowledge of physical or psychological posttraumatic manifestations and often misdiagnose the
symptoms or misattribute them to other causes (Courtois & Gold, 2009).
Pitchford (2009) maintains that contemporary approaches to trauma are flawed, primarily
because of the narrow focus on symptom management rather than acknowledging the barriers
people have to expressing their freedom in choices and will (May, 1999; Paulson & Krippner,
2007). It has been argued that using CBT for PTSD reinforces the medical model of intervention
and Hemsley (2010) comments that this undermines professional autonomy within the National
Health Service (NHS) and private practice, since insurance companies could demand for
interventions to correlate with NICE guidelines (Fairfax, 2008). Tarrier (2010), meanwhile,
argues for continual innovation, which will come from 'recognition of variability and
heterogeneity and the development of new treatment strategies’ (p. 140).
Trauma therapy is a complex biological, psychological and social project that unfolds in stages
over time and may involve many different modalities to reach a stage of optimal recovery
(Herman, 1992). However CBT assumes that the individual’s inability to adequately process the
experience has led to the development of symptoms (Taylor, 2007) which makes little room for
inclusion of other modalities and implies that practitioners have knowledge of the client’s internal
world (Hemsley, 2010). This review aims to consider psychological trauma from
ecopsychological and existential perspectives, not to endorse a particular approach, but to
provoke questions about integration and stimulate debate pertinent to the field of counselling
11

psychology.
Ecopsychology
‘If we do not consider ourselves connected with nature we are in a state of disconnection and
this is what shattered lives are all about. If we cannot make a link with what is outside
ourselves, we cannot get to know ourselves. People who are imprisoned are starved of natural
light, of fresh air, of contact with the natural world. This deprivation of the natural element in our
lives causes psychological damage’ (Linden & Grut, 2002, p.18).
The Ecopsychology Institute (1996) defines ecopsychology as the emerging synthesis of
ecology and psychology; the application of ecological insight to the practice of psychotherapy;
the study of our emotional bond with the Earth; and the search for an environmentally-based
standard of mental health. However, exploring ecopsychology requires more than an overview
of its definition and past; but a critical look at the paths the field has evolved through; since it is
a continually evolving interdisciplinary approach (e.g. Roszak et al., 1995; Burns, 1998; Cohen,
2000; Scull, 2001).
Ecopsychology is a relatively new developing field. While Roszak (1992) publically defined it,
many of the key concepts originated in earlier work (Roszak, 1979; Shepard 1982). Fisher
(2002) proposed ecopsychology as a foundation for a critical theory of modern society, arguing
that it should be a catalyst for social change. He described ecopsychology as an evolving
project, rather than a discipline; identifying the dualism of outer, objective, and inner, subjective
reality which has become part of mainstream psychological discourse. Similarly Adams (2005,
p.270) described ecopsychology as a cultural phenomenon necessitated by our alienation from
nature and identifies ecopsychology as a means of addressing this crisis, which he typifies as
‘the idolatry of the supposedly separate egoic subject and its insatiable quest for security,
certainty, control, and power’.
An Ecopsychological Perspective on Trauma
van Deurzen’s (1997) described our relationship to the earth in a way that I found pertinent to
the premise of ecopsychology: the way we interact with our physical environment should be a
central concern, since it underpins the whole of one’s existence, yet ecological awareness is
kept on the fringes of society. According to May (1967/1982, 1992), Western culture started to
dismantle for a variety of reasons, such as its loss of recognition for the classics and its
depreciation of art, mythology, and historical contexts. This is identified in itself as a trauma by
Glendinning’s (1995, p.51) comment that society has endured a ‘collective trauma … the
12

systemic and systematic removal of our lives from the natural world’. The theme of a repetitive
cycle from the psychological trauma literature pervades here, as Adams (2005) describes a
vicious cycle of our impoverished self and ways of being; which provokes an impoverishment of
nature and in turn accelerates a further impoverishment of our self and ways of being. However,
literature concerning ecopsychology also addresses trauma from developmental and
evolutionary perspectives.
Chawla (1998) connected our relationship with nature to a childhood perception that we had of
the natural world being alive and conscious, suggesting that it plays a significant role in early
development. Shaw (2000) researched childhood nature connections and trauma, observing
that nature was characterised as a protector by traumatised children. For some, nature was the
only place they could feel safe; for others, it acted as a kind of parent. The significance of this
role reflects Khan’s (1964) conceptualisation of cumulative trauma which states that trauma
originates when the primary carer’s protective function is frequently absent or compromised. If
nature can represent such a crucial role in a traumatised child’s life, it could suggest further
required exploration into its therapeutic impact. Shaw makes a connection between such
individuals and later conservation work undertaken, which she attributes as an attempt to
resolve their trauma through restitution. Nature in this example appears to be a powerful
therapeutic resource. Gatersleben (2008) describes a requirement for counselling psychologists
to reinforce our understanding of the psychological components underlying the relationship
between people and their natural environment; a relationship that would appear to develop at a
young age. Connections such as this highlight a need for further detailed research to clarify the
sphere of nature’s role in our early development, identify its attributes, and explore how this
could influence the way we process trauma.
Considering the therapeutic features of nature, two dominant theories draw on evolutionary
perspectives. Kaplan and Kaplan’s (1989) attention restoration theory focused on nature’s
restorative capacity in relieving stress. They suggested that natural surroundings promote
healing by containing the elements that draw on involuntary attention. Ulrich (1984) proposed a
genetic basis for our appreciation of nature in his Stress Recovery Theory (SRT), theorising that
emotional and psychological recovery from stress was effectuated when observing scenes
precipitating reactions of interest, agreeableness and calm: negative affects are replaced by
positive affects; negative thoughts are obstructed. Wilson and colleagues (2008) cited
evolutionary perspectives suggesting that humans respond positively to natural environments
due to a genetic predisposition which once aided survival (Appleton, 1975; Orians &
Heerwagen, 1992). Similarly, Lodrick (2007) illustrates evidence indicating that people
instinctively respond in one (or more) of five predictable ways when threatened: ‘Fight, flight
and freeze’ are well documented responses (Levine, 1997); plus ‘friend’ and ‘flop’ (Ogden &
13

Minton, 2000; Porges, 1995, 2004). For instance, Levine noted that ‘freeze’, aids mammals
when threatened by a predator: the predator has reduced possibility of detecting immobile prey;
many predatory animals will not eat meat that they consider to be dead; and if the predator kills,
the freeze mechanism provides a natural analgesic (Levine, 1997). Between mammals of the
same species the ‘freeze’ response denotes submission, with the conquering animal
acknowledging their dominance and abandoning the subordinate animal. Psychological trauma
occurs when these strategies continue to be adopted long after the threat has passed (Lodrick,
2007). If our trauma responses and characteristics are so inextricably linked to the natural
world, then surely it should be a relevant inclusion both into the conceptualisation of trauma and
therapeutic work undertaken by counselling psychologists.
Therapeutic Implications
A variety of interventions outlined by Buzzell and Chalquist (2009) exist under the
ecopsychology umbrella that could be considered as approaches to psychological trauma. This
review will present wilderness journeys, contemplative practices and the Natural Growth Project,
along with their therapeutic and practical implications.
Wilderness Journeys
Wilderness journeys are typically group retreats with personal growth or therapeutic purposes
(Friese et al. 1998). Used initially in psychotherapy under the name “psychoecology”
(Greenway, 1999), they are described as a powerful countermeasure to depression, anxiety,
and emptiness associated with life in modern society, with participants overwhelmingly reporting
stress reduction, mental clarity, and inner calm (Hendee & Martin 1994).
Driver et al. (1987) created an index of measurable benefits of wilderness journeys including
greater self-sufficiency (e.g. Brody et al., 1988; Klint 1990; Paxton & McAvoy, 2000) and self-
actualisation (Maslow, 1970); suggesting wilderness as a means of self-recovery from trauma
guided by intuition, instigated by and led by the client. Skill development and challenges
successfully met are reportedly perceived as empowering and proof of capability and self-worth
(Johnson 2002). Indeed, Putman et al. (2009) reported in a survey conducted with Guatemalan
aid workers that levels of personal accomplishment were inversely related to PTSD symptoms.
Johnson (2002) advised that wilderness facilitates therapeutic healing as it has limited factors
that require an outward focus, thereby directing the participant’s attention towards inwards self-
reflection. However, research concerning the effects of wilderness therapeutically for trauma is
scarce and inconsistent. Russell et al. (2000) reviewed wilderness therapy and reported positive
14

outcomes, yet the treatment focused on adolescents not exclusive to trauma, making it difficult
to generalise.
Driver et al. (1987) reported that being in the wilderness is a physically-demanding experience,
including associated health benefits set against the detrimental effects of trauma (ISTSS, 2004).
A clinical resource written to facilitate primary health care providers working with survivors of
war trauma and torture advised that such clients could benefit from physical challenges
(Johnson, 2005). However many individuals might find themselves at a disadvantage in this
situation. Tedeschi and Calhoun (1994), advocated caution to be taken with those who might
have serious physical limitations, for they may have insufficient resources to benefit much from
rigorous physical activity; with implications for a counselling psychologist’s assessment to
ensure that a client’s limits and perceptions of the wilderness are accounted for.
The Natural Growth Project
Linden and Grut described the Natural Growth Project in The Healing Fields (2002), which
offers traumatised clients a programme of long-term rehabilitation through a combination of
horticultural work and psychotherapy. This is not an isolated initiative: horticultural therapy has
previously proved effective for addressing the trauma of refugee displacement and resettlement
(Tristan & Nguyen-Hong-Nhiem, 1989). The book documents the first ten years of this project, in
which nature is used as a medium for communication and as a source of healing, based on the
premise that a person who has suffered a trauma can find relief by restoring a sense of
autonomy and self-responsibility through making a connection with a natural environment. The
role of nature is described not only being a place of peace but a space in which clients can
process the trauma: ‘…using nature as a metaphor, it is possible very quickly to access deeply
traumatic events and to work on the most difficult feelings, and the life cycle embodied in nature
carries the promise of healing’ (p.12). It is intended as a handbook for those interested in
establishing something similar, providing an overview of the project, the necessary practicalities,
interwoven with three cases.
Just as I found significance in Keenan’s (1994) incarceration and subsequent reconnection with
the natural world, I remembered that stolen glimpses of vegetation through prison walls were
elements that saved him from hopelessness. The authors describe that for some clients, being
outdoors is often where they have felt safe throughout their lives. For others, the outdoors is
merely more containing than the closed consulting room for sharing traumatic experiences. The
authors describe nature as a significant focus for traumatised clients: identification with the
natural cycle plays out themes of birth, growth, decay and death, providing powerful metaphors
to be worked through therapeutically. A re-connection with the natural cycle appears to be a
15

powerful therapeutic tool.
The medicalised approach for PTSD recommended by NICE guidelines fails to acknowledge
cultural, religious and socio-economic factors (McHugh & Triesman, 2007), and despite an
escalating acknowledgement that PTSD is a universal response to trauma, research
overwhelmingly originates in Western nations (Foa et al., 2008). However, the authors observe
that since these clients come from a number of countries with diverse cultural, religious and
linguistic backgrounds, their difficulty expressing themselves in words was felt to be impeding
any psychotherapeutic work in a typical setting. Traumatic incidents can be difficult to articulate,
yet the authors consider how nature can supply a means of communication for clients to
express memories of painful experiences and their impact. The cross-cultural relevance of
ecopsychology is clear: ‘acknowledgement that they are inhabitants of a shared earth, rather
than inhabitants of a fractured nation, or state, can create an important new healing perspective’
(p.21). Such observations suggest that the natural world transcends national, ethnic, religious
and racial boundaries.
The authors indicate a number of practical considerations, including the contrasting dynamics
which must be managed between serving the therapeutic needs of the client and the need for
the project to generate its own funding, with a risk that clients could ultimately just fulfil the
needs of plant production. Boundaries are also considered: there is no ascribed therapeutic
space or fixed time, requiring perhaps a more mature or experienced practitioner, plus practical
issues such as confidentiality and client feedback would need to be managed outside the
boundaries of the therapy room. As counselling psychologists know, the therapeutic relationship
is an essential component of therapy when working with traumatised clients (Kohlenberg & Tsai,
1991). The natural world could bring another dimension into this relationship, and further work
could investigate this, by considering how aspects of the natural world impinge on our
consciousness. Many of our assumptions developed in early childhood result in the construction
of beliefs about the self and world consistent with these experiences (Janoff-Bulman, 1989),
suggesting that therapeutic work in the natural world could repair some of the cognitive damage
to a trauma survivor’s perception after their world-view has been fragmented.
Contemplative Practices
Adams (2005) discussed awareness practices as a powerful means of building non-dual
relationships with nature. Mindfulness meditation involves the use of focused attention upon
personal experiences to promote calmness and stability (Kabat-Zinn, 1990) and is thought to
help achieve self-acceptance (Chodron, 2001). It typically focuses on several domains,
including interactions between behaviour and the universe (Harvey, 1990), and Follette and
16

colleagues (2006) argue for the inclusion of mindfulness practices for those who have
experienced a traumatic event. Several branches of research indicate a potential link between
trauma and mindfulness-related processes: Pennebacker and O’Heeron (1984) discovered that
the individual’s attempt to suppress memories of trauma can increase the occurrence of
intrusive thoughts (Clark et al, 1991; Wegner et al., 1990) and intensify the negative emotional
experience (Cioffi & Holloway, 1993; Wegner & Zanakos, 1994). Mindfulness interventions have
been integrated into behavioural treatments for trauma with promising preliminary results
(Becker & Zayfert, 2000; Simpson et al., 1998).
Practical Implications
If we are so inextricably linked with the natural world, then it would suggest that a therapist’s
conceptualisation of clients requires expansion. A commitment to good practice, as outlined by
the British Association for Counselling and Psychotherapy (2010), is to keep up-to-date with the
latest knowledge. Since research has demonstrated the benefits of nature, practitioners have an
ethical responsibility to explore how ecopsychology could be used to benefit clients. The
pertinent considerations would therefore concern whatever adjustments counselling
psychologists could make in order to look beyond the presenting problem or routine
methodology and incorporate ecopsychological concepts into trauma therapy.
The assessment could be broadened to incorporate questions about a client’s environment, the
impact that this has on them and their perceived relationship with the natural world (Milton,
2009). Laszloffy (2009) proposed questions that explore potential associations between typical
presenting problems and broader ecological planetary dynamics, allowing the therapist to
consider how a client’s presentation of trauma might be linked to expansive issues like
consumerism, a disconnection from nature, and environmental degradation. Laszloffy (2009)
also advised trainees to expand their frameworks by considering their own relationship with the
natural world; identifying didactic and experiential methods which could be used. Variety
appears to be significant, as the curative powers of nature are enhanced by the degree of
mindfulness and mental focus one brings to these interactions (Louv 2005). Practically, van
Deurzen (1997) observed that clients can be influenced strongly by the consulting room,
requiring consideration around the therapeutic space created to provide an environment for
consultation.
Adams (2005) commented on our requirement for rushed target-based delivery, reminiscent of
the current system of managed health care and evidence-based practice, in which the
requirement is to cure rather than understand (Milton, 2009). This alludes more to an appeal to
change pace, in line with the client as opposed to the treatment, to see the environment in
17

which they function outside of their presenting problem and slow life down to a healing, natural
pace; for to define is to limit, just as to manualise is to generalise. Despite NICE guidelines
advocating otherwise, Hairon (2006) revealed that 93 per cent of general practitioners
prescribed antidepressants due to lack of treatment options, at substantial cost, even if they did
not see this as an effective approach (Halliwell, 2005). Mind (2007) estimated that in 2005, 27.7
million antidepressant prescriptions were written in England, costing the NHS £338 million.
Medications used to treat PTSD include a range antidepressants, adrenergic agents, and
atypical antipsychotics (Friedman et al., 2009).
The NHS era of austerity was indicated by the Department of Health in March 2010 as it
illustrated how it will actualize £4.35 billion of savings annually by 2012-13 (Laurence, 2010).
Budget constraints are seemingly unavoidable, but the inclusion of ecopsychology could
potentially provide a cost-effective and natural addition to existing approaches. Mind (2007)
illustrated that 88 per cent of participants in an ecotherapy study reported an improvement in
mood merely following a green outdoor walk, and recommend ecotherapy as an affordable
treatment for mental distress. Ulrich (1984) discovered that patients following gallbladder
surgery recovered faster with fewer painkillers when they had a view of trees through their
hospital window than when they looked out on a brick wall. Specifically to trauma, Lefkowitz et
al. (2005) proposed an animal-assisted-therapy (AAT) model for survivors of sexual abuse
suffering from posttraumatic stress, anticipating decreased number of therapy sessions. This is
by no means conclusive, but perhaps future research could analyse the costs and benefits: if
one were to abandon a short term schedule, ecopsychology may well prove to be more cost-
effective than existing options; and in the longer term, may even be a preventative measure.
Existential Therapy
‘Trauma individualises us, but in a manner that manifests in an excruciating sense of singularity
and solitude’ Stolorow (2007, p.41).
Existential therapy is ultimately a creative, evolving process though, as Cooper (2003) notes, a
diverse and difficult to define body of psychological theory, practice, and research reflecting an
existential influence with the aim of exploring human reality from the perspective of the client.
The answers to fundamental philosophical questions shape the theory and practice of existential
therapy (Boss, 1979; Cannon, 1991; Cohn, 1984). This fundamentally began with the works of
Kierkegaard (1813-1855) and Nietzsche (1844-1900), as a cultural movement that emerged in
response to the growing awareness of alienation and disconnection pervading contemporary
life, exploring its paradoxes to understand the dimensions of existence that underpin human
dilemmas.
18

The therapeutic process is the experiencing of one's existence, and the client’s identity is not a
fixed quantity. Yalom (1980) described it as a homeless waif that did not belong anywhere,
resolving the problem of definition by listing the themes relating to existence (e.g. isolation,
freedom). This review follows a similar example, by considering the applicability of existential
therapy to trauma. To do this, van Deurzen’s existential dimensions (1997) - a development of
Binswanger’s (1958) framework - and Jacobsen’s existential conceptualisations of crisis are
considered in some depth.
Existential Dimensions: An Existential Perspective on Trauma
Quinn’s (2007) description of transgenerational trauma reported it as a process that stripped
people of their knowledge, spirituality, physical and emotional well-being, and most sadly, has
led to the loss of community (Locust, 2000). This depiction brought to mind van Deurzan’s
existential dimensions documented within her book Everyday Mysteries (1997). The author
separated the four dimensions within which existence takes place, spanned by polar opposites
manifesting as paradoxes, dilemmas, contradictions and conflicts; each with connections and
overlaps which prevail when considering their implications as an approach to trauma.
Physical Dimension
van Deurzen claims we are firstly regulated by physical, biological and natural forces.
Throughout life the basic challenge of our physical survival remains a continuously threatened
primary concern. Just as psychological trauma leads to, among other things, a heightened
sense of mortality and vulnerability (Sadavoy, 1997), it is unsurprising if people wish to abstain
from preoccupations with birth and death, which remind us of our humble and fragile nature.
Jacobsen (2006) conceptualises crisis, a term sometimes used interchangeably with trauma (du
Plock, 2010), as identifying three dimensions: loss, adversity and the opening of existence.
‘Crisis as loss’ can involve direct and physical losses of a specific object or person that they
subsequently miss, resulting in grief. Jacobsen observes that when something is lost, so is a
part of oneself that was attached to that person or thing. Bollnow (1966, p.66) made a similar
connection by discussing bereavement in which ‘…the bereaved does not inhabit his or her
world in the same way as before. Therefore the death of a loved one is loss of existence. The
individual shrinks. The death of a loved one is a piece of one’s own Death’. Just as trauma
heightens our sense of mortality, it potentially induces a range of physical consequences which
continue to threaten it: Kendall-Tackett (2009) claimed that people who have experienced
traumatic events have elevated rates of serious and life-threatening illnesses including
19

cardiovascular disease, diabetes, gastrointestinal disorders, and cancer.
van Deurzen equates our prioritisation of physical needs with a wholly unnatural cycle. She
postulates that physical life is based upon a cycle of need: to fill an empty stomach. However,
we once (as animals still do) enjoyed the process of gathering food and eating at the same time:
the effort was as important as the goal. However, we have since learnt to postpone gratification,
and work is perceived as depleting and exhausting. The natural cycles in which pleasure and
effort are commensurate have been replaced with unnatural cycles of entitlement, comfort,
instant gratification and whatever else might reinforce such views. To me, this reflects an over-
simplified prioritising of quick-fix solutions for psychological trauma, while simplifying - if not
negating - the core issues. Research has indicated that the long-term benefits of CBT are not
quite as clear and certain as sometimes portrayed (e.g. Rufer et al., 2005, Rowe, 2007). Just as
van Deurzen observes that we prefer to outsmart nature and obtain our livelihood with minimal
effort, the reality is that we gain relatively little, for the journey is everything, and the 'goal' is
indefinable and ever-shifting, according to the individual's perspective and the passage of
time. Trauma seemingly affects us all at some point. For some, the real work on personal
development begins with the awareness of the need, the lack, the black hole, the pain: not to be
filled or numbed. The real work is on shaping ourselves and recreating ourselves - reconnecting
with natural cycles within and without. This is an ultimately rewarding effort, the very challenge
of our physical existence.
Social Dimension
Secondly, van Deurzen writes that we are social creatures, inserted into a cultural network
which we internally assess, categorise and ultimately, need to connect with. The author extends
this into a social commentary about the abandonment of our ancestral history; a network that
could be considered therapeutically from individual’s response to trauma. Denham (2008)
described the varied ways people experience, construct and transmit traumatic experiences
intergenerationally within American Indian families, revealing that the family’s history of trauma
and their related narratives appeared to function as a significant carrier of cultural and family
identity. Embedded within the trauma narratives were numerous strategies for resilience, or non-
pathological adaptive responses and abilities to maintain equilibrium after experiencing
adversity (Bonanno, 2004; Conner, et al., 2003; Dion-Stout & Kipling, 2003; Luthar et al., 2000).
Similarly, ven der Hart (1983) described the tribal culture Navahos, for whom to be sick is to
become fragmented, to be healed is to become whole, and to be whole one must be in harmony
with family, friends and nature. This exemplifies the pervasion of the natural world into this
dimension, an area also considered by McCallum and Milton (2008) who discussed the
incorporation of one’s ancestral human and animal history in the therapeutic environment.
20

Psychological trauma no doubt disturbs the social dimension, evidenced in trauma-related
literature that describes our instinctive responses to threat. Our struggle for survival requires us
to distinguish between those who will protect or attack, and when fearful many people trigger
their social engagement system (Porges, 1995). Lodrick (2007) distinguishes ‘friend’ as the
earliest defensive strategy available to us, evident even in the child who smiles - or even laughs
- when being scolded; and highlights the survival strategies ‘fight’, which involves the threatened
individual responding with overt aggression, and ‘flight’ as a means of putting space between
oneself and the threat. It would seem that our way of existing within the social dimension affects
our response to trauma, just as a trauma impacts upon us socially. Research (Maercker, 2008a,
2008b; Nietlisbach & Maercker, 2009, 2009b) has revealed how features of post-traumatic
symptomatology and interpersonal factors may provoke an increase of social exclusion which
may be an additional emotional burden for trauma victims. PTSD is often accompanied by
impairment of psychosocial functioning that is not reflected within the recommendations by
NICE (Hemsley, 2010); and McFarlane and Van der Folk (1996) argue that symptoms such as
repression, denial and dissociation have a social as well as an individual consciousness.
The relevance of the social dimension to trauma draws attention to a central preoccupation for
counselling psychology: the role of the therapeutic alliance. Existential therapy encourages
clients to view their experiences of the world while acknowledging the developing therapeutic
relationship (May, 1995, 1996; May et al., 1958), practically implying that clients are encouraged
to become aware of their experiences, potentialities, and means of interaction with the therapist
(Bugental, 1978; May, 1995; Schneider & May, 1995; Yalom, 1980). The nature of the
relationship may differ from more classical kinds of therapy: for instance the existential therapist
functions as a person in a meaningful encounter with another person. This is particularly
pertinent to traumatised clients, as case examples have illustrated how the development of the
therapeutic relationship has significantly contributed to resolution of thematic issues that defined
the therapeutic work (Roth & Batson, 1993).
Psychological Dimension
van Deurzen writes that we are regulated by our personality, character and mental processes;
referring to the personal space which we protect and develop in relation to our established
physical and social dimensions. Just as trauma shatters the world around us, a prematurely
defined self may develop, which will eventually falter and become depleted. As in the social
dimension, our biological responses to threat could also relate to the psychological dimension.
Lodrick (2007) described ‘flop’ as occurring when muscle tension is lost and the body and mind
become malleable: if impact is imminent the likelihood of surviving will be increased if the body
21

yields, and psychologically the situation will be more bearable if the higher brain functions are
‘offline’.
The formation of self is described by van Deurzen as a constant challenge, but if physical and
social well-being has been acquired at some point, a more positive experience can be drawn
upon to overcome difficulties. Similarly Jacobsen’s (2006) conceptualisation of ‘crisis as loss’
includes psychological losses of a connection with the mind or soul or existential losses of a
relationship with self or other. Though the potential of trauma is consistently prevalent, so is the
possibility of generating bonds of emotional attachment within which debilitating emotional pain
can be held, constructed as more manageable, and ultimately integrated (Vogel, 1994). Here,
the social and psychological dimensions interweave; just as Herman’s (1997) commonality and
reconnection theory suggests that people affected by trauma need to reconnect and rediscover
themselves as well as to connect with those who have endured similar circumstances. This
relational interplay suggests an inter-connection between the existential dimensions and
Jacobsen’s crisis conceptualisations in approaching trauma therapeutically; perhaps
exemplifying the therapist’s requirement to step back and question multiple possibilities.
Jacobsen’s ‘crisis as adversity’ dimension outlines existential givens, which an individual must
learn to accept or face living under false premises. Trauma can enduringly affect one’s sense of
being-in-the-world by altering our preconceptions: the world is unpredictable and can offer no
guarantee of security or consistency (Stolorow, 2007). Such concepts epitomise the subjective
conceptualisation of trauma, with therapeutic implications that listening to the subtleties of
interpretation and remembrance, nuances of affect and self-experience and idiosyncratic social
constructions will provide insight into the client’s unique posttraumatic response (Harvey, 1996).
Spiritual Dimension
van Deurzen suggests that we are modulated by our relationship to the overall framework of
meaning through which we experience the world and make sense of it on a spiritual dimension.
Trauma can indeed provoke an altered philosophy of life that may include spiritual beliefs (Park
et al., 1996). When exposed to trauma, the client can experience a level of death awareness
that enables them to more clearly and richly experience the joys, meanings, values and life
purposes (Frankl, 1969; Yalom, 1980). Jacobsen’s ‘crisis as loss’ dimension includes loss of
meaning and world-view, but his conceptualisation of ‘crisis as an opening-of-existence’ also
resonates here. Trauma presents the therapist with an opportunity to help the client discover a
paradoxical respect for life that occurs in response to the proximity of death, identified by Frankl
(1969) as "finality meanings".
22

Trauma can result in growth, inasmuch as adversity and distress can push someone to develop.
Parkes (1971, p.101) characterises traumas as ‘psychosocial transitions’, explaining that
individuals must ‘restructure [their] ways of looking at the world and [their] plans for living in it’.
Research suggests that a range of traumas can precipitate positive development, for example,
cancer (Cordova et al., 2001; Taylor, 1983); HIV infection (Schwartzberg, 1994); rape (Ashley,
2005; Burt & Katz, 1987; Veronen & Kilpatrick, 1983); incest (Silver et al., 1983); bereavement
(Schwartzberg & Janoff-Bulman, 1991; Calhoun & Tedeschi, 1989; Lehman et al., 1993); heart
attacks (Affleck et al., 1987) and disasters (McMillen et al., 1997). Jacobsen’s (2006, p.46)
describes this concept like a crack in the ground ‘…the crack allows the individual to look deep
into something very significant. In this way, the crisis becomes existential and can become a
personal turning point, a new life possibility.’
Just as trauma can disturb the existential dimensions, it would seem that they could each be
considered therapeutically alongside Jacobsen’s crisis dimensions. Yalom (1980) asserted that
a confrontation with death and freedom could ultimately lead to existential isolation; while
Heidegger used the term “throwness” to refer to the fused affect of loneliness and helplessness:
finding ourselves inserted into an existence not of our choosing.
Therapeutic Implications
In working therapeutically with a trauma, du Plock (2010) cited Jacobsen’s (2006) paper
suggesting that it could work as a counselling psychologist’s guide: which claims that the client
would need to confront and articulate losses, affording the opportunity to sense, acknowledge
and express feelings, while confronting the material that was split off during the traumatic event.
Ultimately, the therapist would collaborate with the client to induce meaning, implications and
possible consequences.
Feelings and Moods
van Deurzen-Smith (1988) summarised the most common feelings that emerge after a trauma
and regarded them, rather like the consequences of trauma are experienced as succeeding one
another in a cycle (e.g. van der Kolk 1989). Each has a destructive and a constructive side, and
the client needs to experience and understand the varying feelings that surface, become
accustomed to them and learn something from them about one’s way of life. Boss (1994)
discussed moods as ways in which an individual’s relationship with the world may manifest.
Boss stressed the need for the individual to be able to sense their varying moods and gradually
open themselves up to them, so that they are able to meet the world freely and be present to
what emerges. This perhaps exemplifies the importance of the counselling psychologist’s own
23

engagement with personal therapy, affording the therapist to have worked through their
personal existential concerns, feelings and moods, since therapists may experience intense
counter-transference feelings and a traumatised client’s process of recovery could be extensive.
I found the cyclical nature and emphasis on the individual’s role a progression from the
bereavement phases (Parkes 1970; Sanders 1999) which imply a degree of passivity and carry
the risk of an assumption that the phases are passed through in order.
Reintegration
du Plock (2010) commented that when someone experiences a trauma, their defences are
activated and some events are so horrific that the consciousness cannot contain them.
Jacobsen cites Spinelli’s (1994) theory of dissociated or divided consciousness, in which certain
aspects of a traumatic experience are placed into one of two compartments of consciousness.
The more humiliating or anxiety-ridden memories are placed in one compartment, while the
more positive memories allocated to the other, with reflections of Brewin’s (1996) Dual
Representation Theory which depicts the traumatic memory stored in two parallel forms. The
individual must gradually attempt to recall these details in therapy. This has similarities to
exposure or reliving associated with CBT, which aims to update and correct trauma history on
the basis that certain aspects of a trauma are omitted from recollections (e.g. Ehlers & Clark,
2000). The subtle distinction lies in the focus on recollection, not correction, as an important part
of the repair process is the confrontation of the client’s beliefs and assumptions that would
influence the compartment that certain memories were initially assigned to, rather than
identifying them as maladaptive.
Reconstruction
Jacobsen observed how therapy can naturally generate a more positive interpretation for the
trauma survivor, as they re-attribute meaning to the traumatic event. This resembles but goes
beyond cognitive restructuring (e.g. Ehlers & Clark, 2000), as the reconstructed meaning and
orientation of one’s life can be characterised by a more intense and intimate life containing
features like reconciliation and acquiescence to one’s existence. Jacobsen provides case
examples from an interview to illustrate positive reconstructions of cancer patients, which could
have been developed to include Spinelli’s (1994) suggestions about the self-construct, which he
proposed was maintained and validated by a remembered past that has flexible meaning and
significance. In this way, as PTSD sufferers demonstrate poor autobiographical memory (Ehlers
& Clark, 2000), a memory of a traumatic incident would selectively reflect the client’s views
about themselves.
24

Ecopsychology and Existential Therapy: Empirical Considerations
While doing this review I was struck by how much empirical evidence there was available to
promote CBT in comparison to these approaches. While I found the discussions and
presentations for ecopsychology to be compelling, many were experiential and not empirical.
Gatersleben (2008) also noted that most experimental environmental psychology research
concentrates on healthy young individuals and advocated future research concerning nature’s
role in the health and well-being of individuals suffering from longer-term psychological
problems to clarify the processes which may underlie environmental preferences and the
restorative effects of nature. This suggests a requirement to collaborate associations between
ecopsychology and its approach to trauma before it can be considered methodologically robust
enough to form solid conclusions.
While The World Health Organization’s (WHO) emphasis that a holistic approach to health is
defined as a state of complete physical, mental and social wellbeing (1946, 1986),
ecopsychology is still an emerging field. It is difficult to define the connection and effects of
nature, with all its interactions and distinctions. However, while a counter argument to
ecopsychological research, this is also its biggest support: for nature also enables people to
‘express the inexpressible’ (Linden & Grut, 2002, p.16).
Despite methodological difficulties, qualitative and quantitative empirical evidence is beginning
to amass. Doherty (2009) noted that ecopsychology has advanced through substantial
clarification and theoretical and practical development, while Winter and Koger (2004) indicated
how ecopsychology can be empirically validated and used in a conventional psychology
framework (e.g., Johnson & Johnson-Pynn, 2008; Vakoch, 2008). Wilson et al. (2008)
acknowledged the emergence of quantitative studies evidencing positive findings to suggest
that the application of nature can improve and conserve mental health, with advanced national
and international policy considerations and directives (WHO, 1997; Guite et al 2006; Grahn &
Stigsdotter, 2003; Hansmann et al. 2007; Diette et al., 2003). They discussed studies in which
symptoms associated with trauma such as self-esteem and depression (ISTSS, 2003), are
significantly observed to improve (e.g. Mind, 2007., Pretty et al. 2005, Reynolds, 2002).
Tedeschi and Calhoun (1994) suggest potential physical benefits to be derived from existential
work after a trauma, and while further exploration is required, this may be a promising area for
investigation. For instance, Epel et al. (1998) discovered that elevations on spiritual growth and
appreciation of life were related to quicker cortisol habituation to a laboratory stressor. Similarly,
25

Bower et al. (1998) reported that HIV sufferers were less inclined to have accelerated declines
in CD4 T-cell levels if they cognitively processed their situation into something meaningful;
paralleling earlier discoveries of reduced rates of mortality in heart attack victims who derived
advantages from their illness (Affleck et al.1987).
Within the existential literature, Yalom (1980), comments that as far as therapy is a deeply
personal human experience, the empirical study of it will contain errors and limitations. A core
epistemological theme within existentialism is concern for the uniqueness and irreducibility of
human experience; unsurprisingly, scientific methods seem inadequate to the task of
understanding the meaningful complexities of human experience (Boss, 1979; May & Yalom,
1995; Norcross, 1987). This relevance of scientific evidence to natural approaches has similarly
been questioned (Adams, 2005; Chalquist 2009); while McCallum and Milton (2008) proposed
acceptance for both empirical and representational approaches so the meaning of natural
phenomena is not lost. Chalquist (2009) goes further to suggest that unrestrained empiricism is
itself a version of trauma; an intellectualised resistance from experiencing the world on its own
terms. EMDR has a substantial supportive empirical base, yet I realised that this was
discovered in a natural setting (Shapiro, 1995). Shapiro created EMDR by chance while taking a
walk in the park, noticing that while she was thinking about negative life issues and voluntarily
moving her eyes back and forth, the intensity of the negative thoughts and feelings were
reduced (Levine & Frederick, 1997). While research has focused on the eye movements
themselves, seemingly little has been done to address the natural setting in which this took
place. This is somewhat like fixating on mere finger movements in instrumental playing, without
cognisance of the actual music. There may be some effect, but it is by no means necessarily the
whole picture.
Conclusions: Integration and Future Research
This review examined the potential for the use of ecopsychology and existential therapy in
psychological trauma. Literature has demonstrated that the cyclical nature of trauma can lead to
prolonged psychological problems, while both of these evolving approaches appear to have
substantial therapeutic benefits, and openings for creative integration. More detailed research
would be beneficial in providing valid and useful information about the efficacy of these
approaches in effecting recovery from psychological trauma, assisting in generating a
conceptual framework that will guide future empirical studies, increasing practitioner awareness
and providing more distinct means of integrating ecopsychology and existential therapy.
While the approaches were presented separately, they were not perceived as mutually
exclusive; indeed, areas frequently overlapped. For instance, literature concerning both
26

approaches acknowledged the significance of a client’s inter-relational presence in the world:
from being-in-the-world to one’s relationship with the natural world. The cyclical theme of
repeated symptoms pervades psychological trauma literature and manifests in both
approaches, reminiscent of van Deurzen’s (1997) observation about our loss of connection with
the natural cycle; the cyclical emergence of feelings in therapy, and Linden and Grut’s (2002)
description of the healing metaphor provided by natural themes of growth and decay. It would
be interesting if future research examined this in more depth, identifying the existential
components which underlie the beneficial therapeutic features of nature as an approach to
psychological trauma.
Despite broad philosophical underpinnings and definitions, the issues raised by existential
therapy appear to be universally perceived and basic to human experience (Yalom, 1980),
suggesting that they could be integrated into almost any approach, while ecopsychology
appears to transcend cultural boundaries. Cross-cultural studies could be applied to both
approaches to investigate their accessibility; exploring how cultures that embrace nature
respond to psychological trauma, and to ultimately address psychological trauma with a broader
all-encompassing focus. Increased accessibility to the most appropriate therapeutic approach
could potentially reach a wider client group, thereby preventing trauma from being simply
displaced onto the next generation in yet another ever-repeating cycle.
This review is not about endorsing a new prescriptive methodology, but an integration and
incorporation of other methods so that the practice of counselling psychology continues to
evolve. CBT is conclusively recommended within the NICE guidelines, with a concentration on
symptoms and diagnostic criteria (Hemsley, 2010), yet this fails to adequately provide a richer
understanding of responses to trauma (McHugh & Treisman, 2007). Adams (2005) comments
that it is typically most effective when ecopsychology operates on the outskirts of the
predominate culture, working collaboratively, striving to alleviate oppressive structures, and
developing possibilities for the actualisation of new experiences. People can only heal from
trauma if supported as whole beings and provided a safe channel to explore their world and
reconnect with themselves (Herman, 1997; Paulson & Krippner, 2007). The responsibility of
counselling psychologists lies in understanding their clients’ anxieties and experiences rather
than coercing them into conforming to a therapeutic model.
Counselling psychology draws upon and seeks to develop phenomenological models of practice
and enquiry in addition to that of traditional scientific psychology (BPS, 2005). While empirical
evidence is beginning to amass for these approaches, further projects should be monitored and
evaluated to reinforce existing findings and expand data. Perhaps scientific methods are
inadequate to comprehend the idiosyncratic meanings we assign to trauma and the unique
27

relationship we have with the natural world, or maybe we are just inter-connected in ways
beyond our understanding. So it is possible that more is needed, namely, a willingness to
experiment and explore other approaches; to identify ways in which these approaches may be
integrated; and to constantly question and debate the accepted methods as a reflective and
critical practitioner.
28

References
Adams, W.W. (2005). Ecopsychology and phenomenology: towards a collaborative
engagement. Existential Analysis, 16(2), 269-283.
Affleck, G., Tennen, H., Croog, S., & Levine, S. (1987). Causal attribution, perceived benefits,
and morbidity following a heart attack: An eight-year study. Journal of Consulting and
Clinical Psychology, 55(1), 29-35.
Affleck, G., Tennen, H., and Rowe, J. (1991). Infants in crisis: how parents cope with newborn
intensive care and its aftermath. New York: Springer-Verlag.
American Psychiatric Association (APA) (1980) Diagnostic and Statistical Manual of Mental
Disorders, 3rd edition, Washington, DC: APA.
American Psychiatric Association (APA) (2000). Diagnostic and statistical manual of mental
disorders: Fourth edition - text revision (DSM-IV-TR). Washington DC: American
Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders
(5th ed.). Arlington, VA: APA.
Ashley, H. (2005). To what extent can traumatic events be viewed as developmental
opportunities? What are the implications of such a position for counselling
psychologists working with clients who have experienced trauma? Cited within a
portfolio of academic, therapeutic practice and research work submitted to the
University of Surrey in partial fulfilment of the degree of Practitioner Doctorate in
Psychotherapeutic and Counselling Psychology, pp.6-18.
Appleton, J. (1975) The Experience of Landscape. London: Wiley.
Banyard, P. (1999). Controversies in Psychology. Florence, KY, USA: Routledge.
Becker, C. B., & Zayfert, C. (2000). Implementation of empirically supported treatment for
PTSD: Obstacles and innovations. Behaviour Therapist, 23: 161–168.
29

Ben Ezra, M. (2001). Earliest evidence of post-traumatic stress? British Journal of Psychiatry,
179(5), 467.
Binswanger, L., 1958. The case of Ellen West. In: May, R., (Ed)., 1958. Existence, Simon and
Schuster, New York, pp. 237–364.
Binswanger, L. (1963). Being-In-The-World: Selected Papers of Ludwig Binswanger. New
York: Basic Books.
Bollnow, O. (1966). Krise und neuer Anfang. Heidelberg: Quelle und Meyer.
Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the
human capacity to thrive after extremely aversive events? American Psychologist,
59(1), 20–28.
Boss, M. (1979). Existential Foundations of Medicine and Psychology (S. Conway & A. Cleaves,
Translation). Northvale: Aronson.
Boss, M. (1994). Existential Foundations of Medicine and Psychology. Northvale: Aronson.
Bower,J. E., Kemeny, M. E., Taylor, S. E,,& Fahey,J. L. (1998). Cognitive processing, discovery
of meaning, CD 4 decline, and AIDS-related mortality among bereaved HIV-seropositive
men. Journal of Consulting and Clinical Psychology, 66(6), 979-986.
Bowlby, J. (1969). Attachment and loss: Attachment. (Vol. 1). London: Hogarth.
British Association of Counselling and Psychotherapy (2010). Ethical Framework. Retrieved 15th
June 2010 from: www.bacp.co.uk/ethical_framework/good_standard.php
British Psychological Society (2005). Professional practice guidelines for counselling
psychologists. Retrieved 16th June 2010 from: http://www.bps.org.uk/publications/prof-
pract/prof-pract_home.cfm.
Brewin, C.R. (1996). The scientific status of recovered memories. British Journal of Psychiatry,
169, 131-134.
Brewin, C.R. (2003) Posttraumatic Stress Disorder: Malady or Myth? New Haven, CT: Yale
30

University Press.
Brody, E., Hatfield, B., & Spalding, T. (1988). Generalizations of self efficacy to a continuum of
stressors upon mastery of high risk sports skills. Journal of Sports Psychology. 10, 32-
44.
Bugental, J. (1978). Psychotherapy and process: The fundaments of an existential-humanistic
approach. Boston: McGraw-Hill.
Burns, G.W. (1998). Nature-Guided Therapy – Brief Integrative Strategies for Health and Well-
being. Brunner/Mazel, Philadelphia.
Burt, M.R. and Katz, B.L. (1987). Dimensions of recovery from rape: focus on growth outcomes.
Journal of Interpersonal Violence, 2, 57-81.
Buzzell, L, & Chalquist, C. (2009). Ecotherapy: healing with nature in mind. San Francisco CA:
Sierra Club Books.
Calhoun, L.G. and Tedeschi, R.G. (1989). Positive aspects of critical life problems: recollections
of grief. Omega: Journal of Death and Dying, 20(4), 265-272.
Calhoun, L.G. and Tedeschi, R.G. (1999). Facilitating posttraumatic growth: A clinician’s guide.
London: Lawrence Earlbaum Associates.
Cannon, B. (1991). Sartre and psychoanalysis: An existentialist challenge to clinical metatheory.
Lawrence: University of Kansas.
Chalquist, C. (2009). A Look at the Ecotherapy Research Evidence. Ecopsychology, 1(2), 64-
74.
Chawla, L. (1998). Significant Life Experiences Revisited: A Review of Research on Sources
of Environmental Sensitivity, The Journal of Environmental Education, 29(3), 11-21.
Chodron P. (2001). The places that scare you: A guide to fearlessness in difficult times. Boston,
Shambhala.
Chu, A., Thorne, A. & Guite, H. (2004) The impact on mental well-being of the urban and
31

physical environment: an assessment of the evidence. Journal of Mental Health
Promotion. 3(2), 17–32.
Cioffi D., Holloway J. (1993). Delayed costs of suppressed pain. Journal of Personality and
Social Psychology 64(2), 274–282.
Clark D. M., Ball S., Pape D. (1991). An experimental investigation of thought suppression.
Behaviour
Research
and
Therapy
29,
253–257
Cohen, M.J., 2000. Nature connected psychology: creating moments that let earth teach.
Greenwich Journal of Science and Technology 1(1), 1–22.
Cohn, H. W. (1984). An existential approach to psychotherapy. British Journal of Medical
Psychology, 57(3), 11-18.
Conner, K. M., Davidson J., & Lee, L. (2003). Spirituality, resilience, and anger in survivors of
violent trauma: A community survey. Journal of Traumatic Stress, 16(5), 487–494.
Cooper, M. (2003). Existential Therapies. Sage Publications Ltd.
Coote A, Allen J & Woodhead D (2004) Finding Out What Works: Building knowledge about
complex, community-based initiatives. London: King’s Fund.
Cordova, M.J., Cunningham, L.C.C., Carlson, C.R. and Andrykowski, M.A. (2001).
Posttraumatic growth following breast cancer: a controlled comparison study. Health
Psychology, 20, 176-185.
Courtois, C. A. (2002). Traumatic stress studies: The need for curricula inclusion. Journal of
Trauma Practice, 1, 1.
Courtois, C.A. and Gold, S.N. (2009). The Need for Inclusion of Psychological Trauma in the
Professional Curriculum: A Call to Action. Psychological Trauma: Theory, Research,
Practice, and Policy, 1 (1) 3–23.
Denham, A. R. (2008). Rethinking Historical Trauma: Narratives of Resilience. Transcultural
Psychiatry, 45(3), 391-414.
Deurzen, E., van (1997). Everyday Mysteries: Existential dimensions of psychotherapy.
32

Routledge.
Deurzen-Smith , E. van (1988). Existential Counselling In Practice, London: Sage
Diette, G.B., Lechtzin, N., Haponil, E., Devrotes, A., Rubin HR. (2003). Distraction theory with
nature sights and sounds reduces pain during flexible bronchoscopy. Chest 123(3),
941-8.
Dion Stout, M., & Kipling, G. (2003). Aboriginal people, resilience and the residential school
legacy. Ottawa, ON: Aboriginal Healing Foundation.
Doherty, J.T. (2009). A Peer Reviewed Journal for Ecopsychology. Ecopsychology 1(1), 1-8.
Driver, B., R. Nash, and G. Haas. 1987. Wilderness benefits: a state of knowledge review. In
Proceedings: national wilderness research conference: issues, state-of-knowledge,
future directions. R. C. Lucas compiler. General Technical Report INT-220. Ogden, UT:
U.S. Dept. of Agriculture, Forest Service, Intermountain Research Station. pp. 294-319.
Du Plock (2010). Trauma in the Relational World: An Existential Perspective. British
Psychological Society, Division of Counselling Psychology Conference: Approaching
Trauma. Attended 17th April 2010.
Ecopsychology on-line (1996). Sourced 17 March 2010 at
http://ecopsychology.athabascau.ca/0996/index.html.
Ehlers, A. & Clark, D.M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour
Research and Therapy 38, 319-345.
Epel, E. S., McEwen, B. S.,& Ickovics,J. R. ( 1998). Embodying psychological thriving:
Physical thriving in response to stress. Journal of Social Issues, 54, 301-322.
Erikson, E. (1950). Childhood and society. New York: Norton.
Fairfax, H. (2008). ‘CBT or not CBT’, is that really the question? Re-considering the evidence
base – the contribution of process research. Counselling Psychology Review, 23(4), 27-
35.
Fisher, A. (2002). Radical Ecopsychology: Psychology in the Service of Life. Albany, NY:
33

SUNY Press.
Foa, E.B., Keane, T.M. and Friedmad, M.J. (2008). Effective Treatments for Posttraumatic
Stress Disorder: Practice Guidelines from the International Society for Traumatic Stress
Studies. New York: Guilford Press.
Follette, V., Palm, K.M., Pearson, A.N. (2006). Mindfulness and Trauma: Implications for
Treatment. Journal of Rational-Emotive & Cognitive-Behaviour Therapy, 24(1), 45-61.
Follette, V.M. and Ruzek, J.I. (2006). Cognitive Behavioural Therapies for Trauma (2nd
Edition). New York: The Guilford Press.
Frankl, V. (1969). The Will to Meaning. New York: New American Library.
Friedman, M.J., Davidson, J.R.T., & Stein, D.J. (2009). Psychopharmacotherapy for adults. In
E.B. Foa, T.M. Keane, M.J. Friedman, & J.A. Cohen (Eds). Effective treatments for
PTSD: Practice guidelines from the International Society for Traumatic Stress Studies
(pp. 245-268). New York: Guilford.
Friese, G., Hendee, J. C., & Kinziger, M. (1998). The wilderness experience program industry in
the United States: Characteristics and dynamics. Journal of Experiential Education,
21(1), 40-45.
Gatersleben, B. (2008). Humans and Nature. Counselling Psychology Review, 23(2), 24-34.
Glendinning, C. (1995). Technology, trauma and the wild. In T. Roszak, M. E. Gomes & A. D.
Kanner (Eds.), Ecopsychology: Restoring the earth, healing the mind. San Francisco:
Sierra Club books.
Gold, S.N. (2008). About Psychological Trauma and the APA Division of Trauma Psychology.
Psychological Trauma: Theory, Research, Practice, and Policy, s(1), 1-2.
Grahn, P. & Stigsdotter, U.A. (2003). Landscape planning and stress. Urban Forestry and
Urban Greening, 2(1), 1–18.
Greenway, R. (1995). The wilderness effect and ecopsychology. In T. Roszak, M. E.
Gomes, and A. D. Kanner (Eds.) Ecopsychology: Restoring the Earth Healing the Mind.
San Francisco: Sierra Club Books.
34

Grey, N. (2007), Post-traumatic stress disorder: Investigation. In The Handbook of Clinical
Adult Psychology Third Edition. Stan Lindsay and Graham Powell (Eds.) (pp. 164-184).
London: Routledge.
Guite. H.F., Clark, C. & Ackrill, G. (2006). The impact of the physical and urban environment
on mental well-being. Public Health, 120(12), 1117–1126.
Hairon, N. (2006). PCTs Poles Apart over Depression Services. Pulse 9, March 9. Retreived
March 2010 from fromhttp://www.pulsetoday.co.uk/story.asp?storycode=4009074.
Halliwell, E. (2005). Up and Running? Exercise therapy and the treatment of mild or moderate
depression in primary care. Mental Health Foundation. London.
Hansmann. R., Hug, S.M. & Seeland, K. (2007). Restoration and stress relief through physical
activities in forest parks. Urban Forestry and Urban Greening, 6(4), 213–225.
Hart, O., ven der (1983). Rituals in psychotherapy: transition and continuity. New York:
Irvington Publishers.
Harvey, M.R. (1996). An Ecological View of Psychological Trauma and Trauma Recovery.
Journal of Traumatic Stress, 9(1) 3-23.
Harvey P. (1990). An introduction to Buddhism: Teaching, history and practices. Cambridge
University Press
Hemsley, C. (2010). Why this trauma and why now? The contribution that psychodynamic
theory can make to the understanding of post-traumatic stress disorder. Counselling
Psychology Review, 25(2) 13-20.
Hendee, J. C. & Martin, V. G. (1994). International wilderness allocation, management and
research: A symposium of the fifth world wilderness congress. International Wilderness
Leadership Foundation, Fort Collins, Colo.: pp. 304–308.
Herman, J.L. (1992) Trauma and recovery: The aftermath of violence-from domestic abuse to
political terror. New York: Basic Books
Higley, N., & Milton, M. (2008). Our connection to the Earth—A neglected relationship in
35

counselling psychology. Counselling Psychology Review, 23(2), 10–23.
International Society for Traumatic Stress Studies (2003). 19th Annual Meeting. New Orleans.
Retrieved 9 March 2010 from http://dynamic.uoregon.edu/~jjf/traumatalks.html.
International Society for Traumatic Stress Studies (2004). 20th Annual Meeting. Retrieved 9
March 2010 from http://dynamic.uoregon.edu/~jjf/traumatalks.html,
Jacobsen, B. (2006). The Life Crisis in a Existential Perspective: Can Trauma and Crisis be
Seen as an Aid in Personal Development? Existential Analysis 17(1) 39-54.
Janoff-Bulman, R. (1989). Assumptive worlds and the stress of traumatic events: Applications
of the schema construct. Social Cognition, 7, 113–136.
Johnson, B. (2002). On the Spiritual Benefits of Wilderness. International Journal of
Wilderness, 8(3) 28-32.
Johnson, D.R. (2005). Restoring the dignity of the human spirit. The Center for Victims of
Torture. Sourced 15 March 2010 at http://www.cvt.org/file.php?ID=5380.
Johnson, L. R., & Johnson-Pynn, J. S. (2008, August). Ecopsychological approach to studying
youth development across cultures. In D. A. Vakoch (Chair), Methodological challenges
in eco-psychological research. Symposium presented at the American Psychological
Association Annual Conference, Boston, MA. Sourced 18 February 2010 at
http://www.apa.org/science/.
Jordan, M. (2009). Nature and Self—An Ambivalent Attachment? Ecopsychology, 1(1) 26-31.
Joseph, S. (2010). Working with psychological trauma. Healthcare Counselling &
Psychotherapy Journal, 10(2).
Kabat-Zinn J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face
stress, pain, and illness. New York, Dell Publishing
Kaplan, R. & Kaplan, S. (1989). The Experience of Nature: A psychological perspective.
Cambridge: Cambridge University Press.
Keenan, B. (2002). An Evil Cradling. United Kingdom: Hutchinson.
36

Kendall-Tackett, K. (2009). Psychological Trauma and Physical Health: A
Psychoneuroimmunology Approach to Etiology of Negative Health Effects and Possible
Interventions. Psychological Trauma: Theory, Research, Practice, and Policy, 1(1), 35–
48.
Klint, K. 1990. New Directions of inquiry into self-concept and adventure experiences. In: Miles,
J. & Priest, S. 1990. Adventure Education. State College, PA: Venture. Pp 163-172.
Khan, M. (1964). Ego distortion, cumulative trauma and the role of reconstruction in the
analytic situation. International Journal of Psycho-Analysis, 45, 272-280.
Kohlenberg, R. J., Tsai, M., (1991). Functional analytic psychotherapy: Creating intense and
curative therapeutic relationships. New York: Plenum Press.
Kolk, B., van der (1989). The compulsion to repeat the trauma: re-enactment, revictimization
and masochism. Psychiatric Clinics of North America, 12(2), 389-411.
Kolk, B., van der (1996). The complexity of adaptation to trauma: self-regulation, stimulus,
discrimination, and characterological development. In van der Kolk, B., McFarlane, A.
& Weisaeth, L. [Eds] (1996). Traumatic stress: the effects of overwhelming experience
on mind, body and society. New York: The Guildford Press.
Laszloffy, T.A. (2009). Remembering the Pattern that Connects: Toward an Eco-Informed
MFT. Contemporary Family Therapy 31, 222–236.
Laurence, J. (2010, 25 March). Health: NHS ordered to find massive savings. The
Independent. Retrieved March 27 2010 at http://www.independent.co.uk/lifestyle
/health-and-families/health-news/health-nhs-ordered-to-find-massive-savingcs-
1927023.html.
Lefkowitz, C., Prout, M., Bleiberg, J., Paharia, I., & Debiak, D. (2005). Animal-assisted
prolonged exposure: A treatment for survivors of sexual assault suffering posttraumatic
stress disorder. Society & Animals, 13(4), 275–296.
Lehman, D.R., Davis, C.G., Delongis, A., Wortman, C.B., Bluck, S., Mandel, D. and Ellard, J.H.
(1993). Positive and negative changes following bereavement and their relations to
adjustment. Journal of Social and Clinical Psychology, 12, 90-112.
37

Levine, D. (1994). Breaking Through Barriers: Wilderness Therapy for Sexual Assault
Survivors. Women and Therapy, 15, 175-184.
Levine, P.A. & Frederick, A. (1997). Waking the Tiger, Healing Trauma. California: North Atlantic
Books.
Lewis, L. (1998). Forward to Shocks to the system. New York: Norton.
Linden, S. & Grut, J. (2002). The Healing Fields; Working with Psychotherapy and Nature to
Rebuild Shattered Lives. Published in Association with the Medical Foundation for the
Care of Victims of Torture, London: Frances Lincoln.
Locust, C. (2000). Split feathers: Adult American Indians who were placed in non-Indian families
as children. Ontario Association of Children’s Aid Societies Journal, 44(3), pp. 11-16.
Lodrick, Z. (2007). Psychological trauma – what every trauma worker should know. The
British Journal of Psychotherapy Integration. Vol. 4(2).
Louv, R. (2005). Last child in the woods: Saving our children from nature-deficit disorder.
Chapel Hill, NC: Algonquin Books of Chapel Hill.
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation
and guidelines for future work authors. Child Development, 71(3), 543–562.
Macy, J., & Brown, M. Y. (1998). Coming back to life: Practices to reconnect our lives, our
world. Gabriola Island, British Columbia: New Society Publishers.
Maddux J.E., Snyder C.R., Lopez S.J. (2004). Toward a positive clinical psychology:
Deconstructing the illness ideology and constructing an ideology of human strengths
and potential. In: Linley PA, Joseph S (Eds.), Positive psychology in practice (pp 320-
34). Hoboken, NJ: Wiley.
Maercker, A. (2008a). A social facilitation model of posttraumatic stress disorder. University of
Zurich: Unpublished manuscript.
Maercker, A. (2008b). Towards a new social facilitation model of PTSD. Paper 39. Berlin:
International Congress of Psychology.
38

Maercker, A., Brewin, C. R., Bryant, R. A., Cloitre, M., Ommeren, M., Jones, L. M., Reed, G. M.
(2013). Diagnosis and classification of disorders specifically associated with stress:
Proposals for ICD–11. World Psychiatry, 12, 198–206.
Manafi, E. (2010). Existential-phenomenological contributions to counselling psychology’s
relational framework. In M. Milton (ed) Therapy and Beyond: Counselling Psychology
Contributions to Therapeutic and Social Issues. Wiley-Blackwell.
Marx, B. P., & Gutner, C. A. (2015). Posttraumatic stress disorder: Patient interview, clinical
assessment, and diagnosis. In N. C. Bernardy, M. J. Friedman, N. C. Bernardy, M. J.
Friedman (Eds.) , A practical guide to PTSD treatment: Pharmacological and
psychotherapeutic approaches (pp. 35-52). Washington, DC, US: American
Psychological Association.
Maslow, A. H. (1970). Motivation and personality (2nd edition). New York: Harper & Row.
May, R. (1967). Existential psychotherapy. Toronto: Canadian Broadcasting Company.
May, R. (1982). Man’s search for himself. New York: Souvenir Press. (Original work published
1967).
May, R. (1992). The cry for myth. New York: Delta.
May, R. (1995). Discovery of being. New York: Peter Smith.
May, R. (1996). Psychology and the human dilemma. New York: Norton.
May, R. (1999). Freedom and destiny. New York: Peter Smith.
May, R., Angel, E., & Ellenberger, H. F. (1958). Existence: A new dimension in psychiatry and
psychology. New York: Basic Books.
May, R., & Yalom, I. D. (1995). Existential psychotherapy. In R. J. Corsini & D. Wedding
(Eds.), Current psychotherapies (5th ed., pp. 262-292). Itasca, IL: Peacock.
39

McCallum, I. and Milton, M. (2008). In Conversation: Ian McCallum with Martin Milton.
Counselling Psychology Review, 23(2), 62-67.
McFarlane, A.C. & van der Kolk, B.A. (1996). Trauma and its challenge to society. In B.A. van
der Kolk, A.C. McFarlane & L. Weisaeth (eds.), Traumatic stress: The effects of
overwhelming experience on mind, body and society. London & New York: The
Guildford Press.
McHugh, P.R. & Treisman, G. (2007). PTSD: A problematic category. Journal of Anxiety
Disorders, 21(2), 211-222.
McMillen, C., Smith, E.M. and Fisher, R.H. (1997). Perceived benefit and mental health after
three types of disaster. Journal of Consulting and Clinical Psychology, 65, 733-739.
Miller, M. W., Wolf, E. J., Kilpatrick, D., Resnick, H., Marx, B. P., Holowka, D. W., . . . Friedman,
M. J. (2013). The prevalence and latent structure of proposed DSM–5 posttraumatic
stress disorder symptoms in U.S. national and veteran samples. Psychological Trauma:
Theory, Research, Practice, and Policy, 5, 501–512.
Milton, M. (2009). Waking Up to Nature: Exploring a New Direction for Psychological Practice.
Ecopsychology, 1(1), 8-13.
Mind (2007). Ecotherapy – the green agenda for mental health. Sourced 10 June 2010 at
www.mind.org.uk/mindweek.
National Institute for Health and Clinical Excellence (2005). Post-traumatic stress disorder.
Retrieved 4 April 2010 from: www.nice.org.uk/Guidance/CG26
Nietlisbach, G. and Maercker, A. (2009a). Effects of Social Exclusion in Trauma Survivors With
Posttraumatic Stress Disorder. Psychological Trauma: Theory, Research, Practice, and
Policy, 1(4), 323–331.
Nietlisbach, G., & Maercker, A. (2009b). Social cognition and interpersonal impairments in
trauma Survivors with PTSD. Journal of Aggression, Maltreatment & Trauma, 18, 382–
402.
Norcross, J. C. (1987). A rational and empirical analysis of existential psychotherapy. Journal
40

of Humanistic Psychology, 27, 41-68.
Ogden, P. & Minton, K. (2000). Sensorimotor psychotherapy: one method for processing
traumatic memory. Traumatology, 6(3), article 3.
Ogden, P., Minton, K. & Pain, C. (2006). Trauma and the body: a sensorimotor approach to
psychotherapy. New York: Norton.
Orians, G.H & Heerwagen, J.H. (1992). Evolved responses to landscapes. In: JH Barkow, L
Cosmides & J Tooby (Eds) The Adapted Mind: Evolutionary Psychology and the
Generation of Culture. Oxford University Press.
Park, C.L, Cohen, L.H, Murch, R. (1996). Assessment and prediction of stress-related growth.
Journal of Personality, 64(1), 71-105.
Parkes, C.M. (1971). Psychosocial transitions: a field for study. Social Science and Medicine,
5, 101-115.
Paulson, D., & Krippner, S. (2007). Haunted by combat: Understanding PTSD in war veterans
including women, reservists, and those coming back from Iraq. Westport, CT: Praeger.
Paxton, T. & McAvoy, L. (2000). Social Psychological Benefits of a Wilderness Adventure
Program. USDA Forest Service Proceedings 15(3), 202-206.
Pennebacker J. W., O’Heeron R. C. (1984). Confiding in others and illness rate among spouses
of suicide and accidental-death victims. Journal of Abnormal Psychology 93: 473–476.
Perry, B.D., Pollard, R., Blakley, T.L., Baker, W.L., Vigilante, D. (1995). Childhood trauma, the
neurobiology of adaptation, and ‘use-dependent’ development of the brain: how ‘states’
become ‘traits’. Infant Mental Health Journal; 16(4): 271–91.
Pitchford, D.B. (2009). The Existentialism of Rollo May: An Influence on Trauma Treatment.
Journal of Humanistic Psychology, 49, 441.
Porges, S. (1995). Orienting in a defensive world: mammilian modifications of our
evolutionary heritage. A polyvagal theory. Psychophysiology, 32, 301-318.
Porges, S. (2004). Neuroception: a subconscious system for detecting threats and safety.
41

Zero to three, May 2004, 19-24.
Pretty. J., Peacock, J., Sellens, M. & Griffin, M. (2005). The mental and physical health
outcomes of green exercise. International Journal of Environmental Health
Research,15(5) 319–337.
Putman, K. M., Lantz, J.I., Townsend, C. L., Gallegos, A.M., Potts, A. A., Roberts, R,C., Cree,
E. R., de Villagrán, M., Eriksson, C. B., Foy, D.W. (2009). Exposure to Violence,
Support Needs, Adjustment, and Motivators Among Guatemalan Humanitarian Aid
Workers. American Journal of Community Psychology, 44(1-2), 109-115.
Quinn A 2007. Reflections on intergenerational trauma: healing as a critical intervention. First
Peoples Child & Family Review 3(4):72–82.
Reynolds V (2002) Well-being Comes Naturally: An evaluation of the BTCV Green Gym at
Portslade, East Sussex. Oxford: Oxford Brookes University School of Health and Social
Care.
Roszak, T. (1979) Person/Planet. New York: Doubleday
Roszak, T. (1992) The Voice of the Earth. New York: Simon & Schuster.
Roszak, T. (1995). Where Psyche Meets Gaia. In T. Roszak, M. E. Gomes, & A. D. Kanner,
Ecopsychology: Restoring the Earth; Healing the Mind. San Francisco: Sierra Club
Books.
Roszak T., Gomes M.E., Kanner A.D. (1995). Ecopsychology; Restoring the Earth, Healing
the Mind. San Francisco: Sierra Club Books.
Roth, S. & Batson, R. (1993). The creative balance: The therapeutic relationship and thematic
issues in trauma resolution. Journal of Traumatic Stress, 6(2) 159-177.
Roth, A. & Fonargy, P. (2005). What works for whom? London & New York: The Guildford
Press.
Rothschild, B. (2000). The body remembers: the psychophysiology of trauma and trauma
treatment. New York: Norton.
42

Rowe, D. (2007). Making Up the Mind. Blackwell Publishing: Oxford
Rufer, M. Grothusen, A., Mas, R., Peter, H., Hand, I. (2005). Temporal stability of symptom
dimensions in adult patients with obsessive–compulsive disorder. Journal of Affective
Disorders, 88(1) 99-102.
Russell, K.C., Hendee, J.C., Phillips-Meyer, D. (2000). How Wilderness Therapy Works: An
Examination of the Wilderness Therapy Process to Treat Adolescents With Behavioral
Problems and Addictions. USDA Forest Service Proceedings 15(3), 220-228.
Sanders, C. (1999). Grief: the morning after: Dealing with adult bereavement. New York:
Wiley.
Sadavoy, J.(1997). Survivors: A Review of the Late-Life Effects of Prior Psychological Trauma.
American Journal of Geriatric Psychology: 5, 4.
Schneider, K. J., & May, R. (1995). The psychology of existence: An integrative, clinical
perspective. New York: McGraw-Hill.
Schore, A.N. (2000). The effects of early relational trauma on right brain development, affect
regulation,and infant mental health. Infant Mental Health Journal, 22(1–2): 201–69.
Schwartzberg, S.S. (1994). Vitality and growth in HIV-infected gay men. Social Science and
Medicine, 38, 593-602.
Schwartzberg, S.S. and Janoff-Bulman, R. (1991). Grief and the search for meaning: exploring
the assumptive world of bereaved college students. Journal of Social and Clinical
Psychology, 10, 270-288.
Scull, J. (1999, March). Ecopsychology: Where does it fit in psychology? Paper presented at
the Annual Psychology Conference, Malaspina University College [Electronic version].
Retrieved March 30, 2010, from http://members.shaw.ca/jscull/ecointro.htm
Scull, J., 2001. Reconnecting with nature. Encompass , 5, 1–5.
Shapiro, F. (1995). Eye movement desensitization and reprocessing: basic principles,
43

protocols, and procedures. New York: Guildford Press.
Shaw, S. (2000). Childhood and Nature. Department of Social and Political Inquiry and
Graduate
School
of
Environmental
Science.
Sourced
at
http://www.ecopsychology.org/journal/gatherings/childhoo.htm
Shepard, P. (1982). Nature and Madness. San Francsiso: Sierra Club Books.
Silver, R.L., Boon, C. and Stones, M. (1983). Searching for a meaning in misfortune: making
sense of incest. Journal of Social Issues, 39, 81-102.
Simpson E. B., Pistorello J., Begin A., Costello E., Levinson J., Mulberry S., Perlstein T., Rosen
K., Stevens M. (1998). Use of dialectical behaviour therapy in a partial hospital program
for women with borderline personality disorder. Psychiatric Services 49, 669–673.
Solomon, Z., Kotler, M. and Mikulincer, M. (1988). Combat-related posttraumatic stress disorder
among second-generation Holocaust survivors: preliminary findings. American Journal
of Psychiatry, 145, 865-868.
Spinelli, E. (1994). Demystifying Therapy. London: Constable.
Stolorow, R.D. (2007). Trauma and Human Existence: Autobiographical, Psychoanalytic and
Philosophical Reflections. New York and London: The Analytic Press.
Sullivan, H. S. (1940). Conceptions of modern psychiatry. New York: Norton.
Tarrier, N. (2010). The Cognitive and Behavioral Treatment of PTSD, What Is Known and What
Is Known to Be Unknown: How Not to Fall Into the Practice Gap. Clinical Psychology:
Science and Practice, 17(2), 134-143.
Taylor, S.E. (1983). Adjustment to threatening events: a theory of cognitive adaption.
American Psychologist, 38, 1161-1173.
Taylor, S. (2007). Clinicians Guide to PTSD: A cognitive behavioural approach. London &
New York: The Guildford Press.
Tedeschi, R.G. & Calhoun, L.G. (1994). Posttraumatic Growth: Conceptual Foundations and
Empirical Evidence. Psychological Inquiry, 15(1),1-18.
44
Tedeschi. R. G., & Calhoun, L. G. (1995). Trauma and transformation: Growing in the aftermath
of suffering. Thousand Oaks. CA: Sage.
The Independent.ie (1999). Sourced on 2 May 2010 online at
http://www.independent.ie/national-news/how-brian-keenan-found-love-and-learned-to-
live-again-400576.html.
Totton, N. (2005). Can psychotherapy help make a better future? Psychotherapy and Politics
International, 3(2) 83–95.
Tristan, J., & Nguyen-Hong-Nhiem, L. (1989). Horticultural therapy and Asian refugee
resettlement. Journal of Therapeutic Horticulture, 4, 15–20.
Ulrich R.S. (1979) Visual landscapes and psychological well being. Landscape Research 4(1)
17–23.
Ulrich, R.S. (1984). View through a window may influence recovery from surgery. Science,
224(4647), 420–421.
Vakoch, D. A. (2008). Teaching ecopsychology in a doctoral training program. In D. A. Vakoch
(Chair), Teaching ecopsychology—Institutions and approaches that foster innovative
psychology curricula. August 2008. Symposium presented at the American
Psychological Association Annual Conference, Boston, MA.
Veronen, L.J. and Kilpatrick, D.G. (1983). Rape: a precursor of change. In E.J. Callahan and
K.A. McClusky (Eds), Lifespan developmental psychology: non-normative events. San
Diego, California: Academic Press.
Vogel, L. (1994). The Fragile 'we': Ethical Implications of Heidegger's Being and Time.
Evanston, IL:MIT.
Wainrib, B.R. (2006). Healing Crisis and Trauma with Body, Mind, and Spirit. New York, NY,
USA: Springer Publishing Company.
Wegner D. M., Shortt J. W., Blake A. W., Page M. S. (1990). The suppression of exciting
Thoughts. Journal of Personality and Social Psychology, 58(3): 409–418.
45

Wegner D., & Zanakos S. (1994). Chronic thought suppression. Journal of Personality, 62(4),
615–640.
Wilson, N.W.; Ross, M.K., Lafferty, K. Jones, J. (2008). A review of ecotherapy as an adjunct
form of treatment for those who use mental health services. Journal of Public Mental
Health, 7(3): 23-35.
Winter, D. D., & Koger, S. (2004). The psychology of environmental problems (2nd ed.).
Mahwah, NJ: Lawrence Erlbaum.
World Health Organization, (1946). Constitution of the World Health Organization. New York:
The World Health Organization.
World Health Organization (1986) Ottawa Charter for Health Promotion. First International
Conference on Health Promotion: The move towards a new public health. Ottawa:
World Health Organization, Health and Welfare Canada, Canadian Public Health
Association.
World Health Organization (1997) Twenty Steps for Developing a Healthy Cities Project (3rd
edition). Milan: WHO.
Yalom, I.D. (1980). Existential Psychotherapy. New York : Basic Books.
Young, R. and R. Crandall. 1984." Wilderness use and self-actualization." Journal of Leisure
Research 16(2):149-160.
46

Appendix A
Counselling Psychology Review Notes for Contributors
Manuscript requirements:
1) The front page (which will be removed prior to anonymous review) should give the
author(s)’s name, current professional/ training affiliation and contact details. One
author should be identified as the author responsible for correspondence. A statement
should be included to state that the paper has not been published elsewhere and is not
under consideration elsewhere. Contact details will be published if the paper is
accepted.
2) Apart from the front page, the document should be free of information identifying the
author(s).
3) Authors should follow the Society’s guidelines for the use of non-sexist language and
all references must be presented in the Society’s style, which is similar to APA style (the
Style Guide, available from the Society, or downloadable from /publications/submission-
guidelines/).
4) For articles containing original research, a structured abstract of up to 250 words
should be included with the headings: Background/Aims/Objectives,
Methodology/Methods, Results/Findings, Discussion/Conclusions. Review articles
should use these headings: Purpose, Methods, Results/Findings,
Discussion/Conclusions.
5) Approximately five key words should be provided for each paper.
6) Authors are responsible for acquiring written permission to publish lengthy
quotations, illustrations, etc. for which they do not own copyright.
7) Graphs, diagrams, etc., must have titles.
8) Submissions should be sent as e-mail attachments. Word document attachments
should be saved under an abbreviated title of your submission. Include no author
names in the title. Please add ‘CPR Submission’ in the e-mail subject bar. Please
expect an e-mail acknowledgement of your submission.
9) Proofs of accepted papers will be sent to authors as e-mail attachments for minor
corrections only. These will need to be returned promptly.
47

The Client Experience of Existential Therapy
An Investigation into the Experience of Existential Therapy for a Client using
Interpretative Phenomenological Analysis
Lisa Corbett
Supervised by Martin Milton
Abstract
Existential theory is a relatively emerging field and to date, the experience of a client who has
undertaken existential therapy has been overlooked as a distinct research focus. This paper
presents findings from a qualitative study with six participants who had all received existential
therapy. Interviews were transcribed and the data was analysed using interpretative
phenomenological analysis. Emerging themes focused on essential components of existential
therapy; paradoxes of thinking; preconceptions and relational issues. The study could be seen
as expanding the knowledge base for existential therapy, and for integrative practitioners who
may wish to consider ways their own practice could potentially incorporate and adapt some of
the insights.
Key words: existential therapy; client.
48

I didn’t feel that she had any sort of clichéd approach, I think it was very individual based on
what I was bringing, and there wasn’t any judgement on what I was bringing
An Investigation into the Experience of Existential Therapy for a Client using
Interpretative Phenomenological Analysis.
Introduction
The term 'existential therapy' is difficult to explicitly define because it has been used to refer to a
number of therapeutic practices, all aiming to explore human reality from the perspective of the
client (Cooper 2003). The answers to fundamental philosophical questions that underpin the
way the world is perceived shape the theory and practice of existential therapy (Boss, 1979;
Cannon, 1991; Cohn, 1984). Rather than pathologising the client, existential therapy ‘does not
seek to cure or explain, it merely seeks to explore, describe and clarify in order to try to
understand the human predicament’ (van Deurzen, 1997, p.3). Lantz (2004) highlights that
existential psychotherapists generally believe that effective therapy is not procedurally based,
but instead evolves out of the therapist’s willingness to utilise the self to facilitate relationship,
action and reflection to help the client work through and struggle with the ultimate issues of
human life during the therapeutic process (Frankl, 1969; May, 1983; Mullan and Sangiuliano,
1964; Whitaker, 1976; Yalom, 1980). Existentially oriented therapists strive toward honest,
mutually open alliances with their clients, encouraging them to consider their experiences of the
world while acknowledging the developing therapeutic relationship (May, 1995, 1996; May et al.,
1958).
While existential therapy is a relatively emerging field, van Deurzen (2009) notes that it is
becoming a household name and there are numerous mental health and therapeutic services
both in the voluntary and public sector that specialise in the approach. Despite this, existential
therapy is largely understudied and existing literature focuses largely on the aims and
philosophy of the approach, conveying a multitude of forms, styles and approaches (Cooper,
2003). With so much variety and definitional difficulties, one might wonder how this could
translate to a client considering therapy. Little is known so far about what draws someone to
choose an existential therapist and the impression that this approach leaves the client with.
Research Question
The aim of this research was to explore clients’ subjective experience of existential therapy, in
order to enhance practitioner awareness in this under researched area and potentially inform
49
those considering an existential approach. Within this, it aims to add to our understanding of
individual experiences and perceptions of existential therapy and in turn help trainees and
therapists reflect upon and evaluate their therapeutic style – an important focus for counselling
psychology. The objective of the study was to acknowledge the subjective experiences of a
range of clients who had received existential therapy. With these principles in mind, the
research is guided by the question ‘how do clients describe their experiences of existential
therapy?’
The Existential Client Experience
‘Clients want a psychotherapist who is trustworthy, understanding and capable’ (van Deurzen,
1997:189). While such assumptions have yet to be substantially investigated, some literature
has speculated on the motivations a client might have for choosing existential therapy. van
Deurzen (2007) observed that the approach often attracts clients who feel disinclined to trust
other human beings because they perceive the existential approach as leaving them in total
control, but also states that the existential approach is often misconstrued as ‘intellectual’. With
potential pre-conceptions held about existential therapy and specific reasons that a client might
have for choosing this approach, a qualitative study could enrich our understanding about both
the perception of existential therapy and the impression that it makes on a client.
The client experience could be considered from the perspective of a learning tool for
practitioners and trainees, with which to evaluate their therapeutic style. van Deurzen (1997)
notes that the work of existential therapists can vastly improve if they are willing to learn from
clients’ responses and comments. Boss(1963), Frankl (1959), Mahrer (2000), May (1983),
Whitaker (1989) and Yalom (1980) have all reported that becoming a good therapist demands
that psychotherapists rigorously and consistently expose themselves to the involvements,
commitments, vulnerabilities and responsibilities that occur in a therapeutic relationship with a
real client requesting help. In this way ‘clients are our supervisors, or even therapists (van
Deurzen, 1997:224). Exploring client’s responses and comments regarding existential therapy
could substantiate this principle by providing qualitative data to generate insight for practitioners
and trainees about the impact of such an approach.
Exploring the client’s experience of therapy is both appropriate and necessary for the
development of the field of counselling psychology. Clients make an active contribution to the
therapeutic process: the therapeutic encounter is fundamentally an interpersonal one in which
therapist and client interact in an attempt to produce the conditions necessary for change (Butler
& Strupp, 1986). However, most research to date has focused on the techniques, actions and
competencies brought by therapists and has tended to neglect the feelings, values, attributes
and skills brought by clients (Macran et al., 1999). While Macran et al (1999) acknowledge the
50

importance of recognising and responding to client requirements, little work has been conducted
into defining these requirements and exploring clients' perspectives. The client experience is a
vital area of research given the rapidly changing political and economic context in which therapy
is delivered, and made even more pertinent since £70 million has been pledged to expand
psychological therapies across the NHS over the next year (Lansley, 2010). While the
availability of psychotherapy within the National Health Service (NHS) has always been limited,
pressures increase to justify services on the basis of effectiveness and user demand (Macran et
al., 1999). Investigations into the client experience of existential therapy will not only build up the
research base of this so far understudied approach, but could ultimately stimulate debate and
consideration regarding the development and incorporation of other approaches into existing
modalities.
Existential research currently suffers from a marked absence of client focused studies and is
indeed one of the most under-researched approaches in counselling and psychotherapy
(Cooper, 2004). Studies have addressed the experience of therapists conducting existential
therapy (Wilkes & Milton, 2006), and case studies have been presented from the perspective of
the therapist (e.g. du Plock, 1997; van Deurzen, 2007), yet research that reflects the client’s
experience is distinctly lacking. Some initial work has portrayed a client’s perception of
existential therapy in the form of a book by Elkin (Yalom & Elkin, 1990) who was in therapy with
Yalom, but again there seems to be little availability of qualitative research to thoroughly
investigate this perspective.
Other approaches have, however, been researched from a client perspective. O’Connor et al
(1997) conducted qualitative research to investigate clients’ experiences of narrative therapy,
while MacCormack et al (2001) conducted a qualitative investigation into cancer patients’
experiences of psychotherapy. Since qualitative research has already been applied to these
therapeutic approaches in highlighting what is helpful / unhelpful, it could also be useful and
worthwhile to quantitatively explore existential therapy from this angle.
Most existentialist claims are not subject to empirical investigation even though ‘evidence based
practice’ increasingly requires therapies to demonstrate efficacy and efficiency (Rowland &
Goss, 2000). Client experiences are captured quantitatively via feedback forms and surveys, for
instance by Bende and Crossley (2000) who collected psychotherapy patients’ views of
treatment via questionnaire. Epistemologically, existential therapy is hindered as “the basic
tenets of existential therapy are such that empirical research methods are often inapplicable or
inappropriate” (Yalom, 1980, p.10). However, existential therapists generally have reservations
about the use of systematic experimental research methods to generate knowledge about the
practice and effectiveness of existential therapy and for many such experimental research
51
methods are best replaced with the process of participation (Lantz, 2004). Therapy is
fundamentally a complex human endeavour, and so this study proposes to move beyond the
basics of the easy to measure efficacy studies, and into a more complex realm by generating
rich qualitative data that explores how participants make sense of their experience of existential
therapy.
Method
Design
The emphasis of the study was to offer insights into clients’ experiences of existential therapy. A
qualitative research method was adopted because the project involves a detailed exploration of
participants’ personal experience (Willig, 2008). Qualitative studies can also be particularly
appropriate to initial exploration of unchartered areas, as they aim to remain as faithful as
possible to the phenomenon and context in which it appears. Another advantage of qualitative
studies is that a limited number of participants allows for a more in depth analysis and can act
as a baseline for larger studies of the same type (Smith et al 1997). Since the research question
is concerned with the in-depth exploration of client experiences and how they perceive and
make sense of that experience, a phenomenological research method is appropriate.
Interpretative Phenomenological Analysis (IPA: Smith, 1996; Smith et al., 1997; Smith &
Eatough, 2007) was adopted to analyse the data since it provides a systematic way of analysing
qualitative data to explore participants’ experiences of the world (Smith, 2008). IPA is concerned
with an individual’s personal perception or account of an object or event, in this instance
existential therapy, as opposed to an attempt to produce an objective statement of the object or
event itself, and is also appropriate to explore the phenomenology of a small sample.
Sample
This study captures the experiences of clients who have experienced therapy undertaken by a
therapist who states that they work existentially. All participants had specifically sought out an
therapist who had advertised themselves as practising existentially, and all were either in
therapeutic training or had a psychological or therapeutic background. Suitable participants
were deemed to be those who had been offered a minimum of six sessions and attended at
least four sessions to ensure that they have sufficient experience to discuss the process in
some depth. This promoted the likelihood of securing a relatively purposive homogeneous
sample, meaning that participants shared certain basic similarities and were chosen for the
purpose of the research project (Smith, Flowers & Larkin, 2009) and thereby increasing the
likelihood of being able to discern commonalities of viewpoint and reported experience.
Participants were recruited by opting into the study. The study was publicised two ways - by
52
posters, and also electronically through website forums with an existential interest. Existential
therapists were also contacted and requested to publicise the study to past clients who meet the
criteria. Participants who expressed an interest were emailed an information sheet containing
the title and brief description of the research. Smith and Osborn (2003) note that sample size
depends on a number of factors and that there is no 'right' sample size (p.54), though 4-6
participants will ideally be sourced for the study to allow sufficient in-depth engagement with
each individual case but also a detailed examination of similarity and difference, convergence
and divergence. Six participants were recruited, three women and three men aged between 24
and 56. When describing their ethnicity, four participants described themselves as British, one
German, and one Greek. Participants had all specifically decided upon a course of therapy with
a practitioner who explicitly stated that they practise existentially, and collectively they had all
received existential therapy ranging from four sessions to two and a half years. Once they
agreed to participate, a consent form was signed (appendix C).
Procedure
A pilot interview was carried out, at the end of which the participant had the opportunity to give
feedback about the procedure, which informed the way that subsequent interviews were
conducted. Interviews took place in a quiet public place or via Skype with a webcam at a time
that was convenient for the participant. All participants were re-briefed as to the purpose of the
study, how the data is recorded and used and issues related to confidentiality and the disposal
of recordings (appendix B). Time was allocated to answer any questions participants had.
Consent forms were signed at this point (appendix C). The interviews lasted between 30
minutes and 1 hour 15 minutes. During interviews, participants were invited to interact with
minimal prompting or structure and the interview style aimed to be non directive and the
researcher was mindful of counselling skills as advocated by Rogers (1957). In order to remain
entirely phenomenological and give the participant maximum freedom to explore their
experience, just one question was asked which was “can you tell me about your experience of
existential therapy” (Langdridge, 2007); the participant led the entire interview thereafter. This
question was decided upon because it closely resembled the research question, and was used
in the pilot interview to determine its coherence and potential to allow the participant space to
explore their experience in greater depth. It was anticipated that this broad open-ended question
would allow the participant to set the parameters of the topic, and prevent the researcher from
imposing their understanding of the phenomenon on the participant’s narrative (Smith et al.,
2009). The interview was therefore more likely to be conversational in style, generating the
potential for genuine rapport to be formed, and consequently more open and honest responses
(Langdridge, 2007). There was no attempt to test a predetermined hypothesis, but to just allow
the participant the space to flexibly explore this area in some detail. Broad prompts were
employed as required which were discussed in supervision, such as “could you give an
53

example?” and “how do you experience that?”, but the researcher was mindful to follow the lead
of the participant. Finally, participants were given the opportunity at the end to say anything
further on the subject that had not been talked about and whether they had any questions for
the interviewer.
Ethical Considerations
Ethical approval was obtained through the Ethics Committee of the Faculty of Arts and Human
Sciences at the University of Surrey (appendix A) and risks and potential hazards for the
participant and researcher were identified and considered (appendix E). It was possible that
some clients opting into the study were still undergoing existential therapy, and potentially
vulnerable, so distress was minimised by participants opting in to the study; informed consent
and applying the principles of person-centred counselling including empathy, genuineness and
unconditional positive regard in conducting interviews. Participants were informed that if they felt
distressed during the interview they were free to withdraw at any time, and alternative support
networks would have been suggested if distress was caused. After the interview participants
were given the opportunity to reflect on how they felt during the interview and informed that they
could still withdraw from the study until the point of data analysis without the need to provide
further explanation. As a safety precaution, the researcher met participants in a quiet but public
meeting place, informed someone of their whereabouts and telephoned that person after the
interview.
Data Analysis
In order to analyse the data, the recorded interviews were transcribed verbatim and the data
was analysed using IPA. IPA aims to explore in detail how participants make sense of their
personal and social world, and how they think about the phenomenon under investigation. It
focuses on how the participants experience the phenomenon, rather than whether their
accounts are true or false or to what extent their perceptions correspond to an external reality
(Willig, 2001). In order to explore these experiences using IPA, four recommended stages were
followed (Smith & Osborne, 2003). Firstly, the transcripts were read repeatedly to enable the
researcher to develop a deeper connection to the data and the participant's experience.
Secondly, the researcher began to note observations, ideas and potential interpretations on the
transcripts. Thirdly, emerging themes were identified, which required a higher degree of
interpretation from the researcher. This was done systematically for each transcript, and the
researcher considered throughout how the previous transcripts could have impacted upon the
researcher's knowledge throughout the process (Smith et al., 2009). Fourthly the themes were
clustered across all transcripts by strength of association to each-other and super-ordinate and
subordinate themes were determined. While doing this, the researcher was aware of their own
insights from being either a client or therapist, and was careful to bracket any assumptions so
54
that any emergent theme was based upon the participant's own account. The recordings were
listened to one final time so that the researcher could reflect upon the themes identified while
listening to the participants' accounts and check for coherence. The themes were places in a
table of super-ordinate and subordinate themes and the interpretations and appropriateness of
the connections made between text and themes were subsequently discussed in supervision.
Evaluative Criteria
Qualitative research is embedded in a philosophy of knowledge development distinct from the
positivist tradition. Whilst positivist research attempts to establish objective knowledge
‘represented as regularities, even laws’ (Elliott et al., 1999, p.217), qualitative research
relativises the knowledge gained to the participants, the situation studied and the researcher.
Therefore traditional evaluative criteria such as validity and reliability become inappropriate.
This study adhered to alternative evaluation criteria suggested by Elliott et al. (1999) such as
persuasiveness; owning one’s perspective; situating the sample; resonance with readers;
grounding in examples and providing credibility checks and audit trail coherency.
Analysis
For the following analysis, direct quotes from the interview transcripts are written in italics.
Ellipses points (…) are used to indicate that a passage has been omitted from the original
transcript. In order to preserve participants’ anonymity, they are referred to as P1-6, and
situations that might disclose personal details have been omitted and/or changed with a
fictitious equivalent.
Using IPA, four super-ordinate themes across all the transcripts were identified. Each super-
ordinate theme has its own set of identified subordinate themes, though only subtle differences
lie between one super-ordinate theme and another and also within the subordinate internal
themes. These are reported in table 1 below.
Table 1
Super-ordinate Theme
Essential characteristics
Paradoxes of Thinking
Preconceptions
Subordinate Theme
Not being labelled
Non judgemental acceptance
Client responsibility
A lack of defined structure
Being in the present
Difficult to Define
Intellectual yet Unknowing
Decompartmentalisation leading to
Connection
Well trained
55
Relationship
Intellectual
Lack of information
Boundaries
A shared space
Trust
Adult-to-adult
Due to word limitations it is not possible to elaborate each theme in detail. I therefore intend to
focus on those themes that are relevant to my research question and have not been addressed
in previous literature. These are: Essential components of existential therapy and Paradoxes of
thinking.
Essential characteristics of existential therapy
This theme concerns the particular characteristics of existential therapy, how these came across
to the participant, and what made the therapy existential. Subthemes include how participants
found the therapy to be structured, labelling, acceptance, client responsibility, the focus on the
present moment, and the difficulties in defining the nature of the work.
Not being labelled
Several participants highlighted the impression that they did not experience the therapy as
labelling. P4, who was in psychotherapeutic training at the time of interview and had received
both Cognitive Behavioural Therapy (CBT) and existential therapy respectively, talks about
labelling in two terms: that the therapy itself did not fit a label of any sort, and that it similarly did
not apply labels.
The thing that has appealed to me about the existential modality is its its lightness of touch in
terms of needing you to be you know fitting a model err fitting a label fitting a pigeon hole or
whatever, as well as the way it was seen as being quite fluid and no one really is stuck in a
certain model or given a certain label. (P4)
By reflecting on an experience of CBT, P4 offered insight into the nature of existential therapy:
CBT was quite it was quite labelling and quite you know very specific and terribly sure about a +
b leads to c and so on – and although that was great for me at the time um and it helped me to
sort my life out a bit err there is something about it I found a little bit uncomfortable um err and I
don’t find that in the existential modality I find it much more freer and moulding itself around
your own situation. (P4)
P4 appears to experience the lack of labelling in therapy as liberating, by explaining that it
works around him rather than the other way around. The experience of not being given a label
is also described in terms of movement: ‘fluid’ as opposed to ‘stuck’.
56

P6, who had received existential therapy while in psychotherapeutic training, said that his
therapy was: a rejection of labelling um and that really works for me because I just think it’s a
very limited way of looking at the world and can buy into people’s stereotypes and just expand
upon people’s idea of who they are and what the world is rather than opening up the world.
An example of this is: if I call myself narcissistic or another she rejects the term, not outright she
just says she would rather not use those terms, better instead to ask someone ‘what do you
really mean by that, why do you ask me if you’re narcissistic, what do you understand as
narcissistic (P6)
We come into therapy with ideas about who we are, and those ideas, if I am this then I’m not
the other and the other is often something else or I find myself in opposition, so I can’t label
myself without labelling the other two. By getting rid of the labels completely I can walk into the
room and I can experience myself afresh, because labels are symbolic and if we’re trying to get
away from the mind and into the feeling well then to say ‘why do you feel narcissistic’ rather
than one of the eight criteria, is a very different ball game. (P6)
P6 appears to describe the therapy as being quite dismissive of labels, and admits that he is
challenged by his therapist when he applies them to himself. Once he dismisses one label, then
the implication is that he would dismiss others. He offers insight into the impact that this has
upon him, as being able to experience himself ‘afresh’ once he abandoned his usage of labels.
He also comments that it has helped in terms of thinking of emotions rather than thoughts,
because he has considered how it feels to be narcissistic, rather than just accepting the term as
a label.
Non judgemental acceptance
Related to the concept of a lack of labelling, some quotes also describe a sense of non
judgemental acceptance in existential therapy.
You know it was very kind of accepting it was incredibly accepting. (P2)
The key thing I find in existential therapy is this sense of acceptance, he doesn’t know what’s
best for me and he never seeks to tell me such [...] he is the only therapist that I’ve ever
worked with who doesn’t question it, who totally accepts that that is the way I want it to be that
is the way I choose it to be. (P4)
Whereas I’ve found in the past there’s a particular uncertain relationship, other therapists have
been very quick to say that is dysfunctional that means such and such that err you know that’s a
57
trap you need to move on from that and so on and so forth – and I don’t get that from err from
an existential therapist. (P4)
P4 asserts that previous therapists have been quick to term something as dysfunctional, and
also to see something in quite certain or definite terms. Whereas now he appears to feel that the
therapist accepts him without question, and does not impose judgement. P4 also refers to the
idea that his therapist did not ‘know what’s best for me’, which could imply that he experiences a
sense of balance in their relationship: rather than looking to a therapist for guidance, it would
appear that he perceived his therapist as an equal participant in the process, working
collaboratively in order to try and understand his issues.
My initial impression was um that it was very un-judgemental, and very accepting and very um
supportive um and yeah the particular thing at the beginning was ‘what is it to be a student,
why, what is it to be, why am I doing this and I’m not doing something else’ and exploring all of
that was really important. (P5)
P5 also describes this sense of non judgemental acceptance which she appears to have felt
from the onset of therapy and found supportive. However she also mentions that her therapist
demonstrates a level of curiosity about what she does, questioning how aspects of her life are
experienced.
Client responsibility
Several participants gave their impression of client responsibility in existential therapy. Some
gave a sense that they found the therapy to be non directive and open, and others describe it as
being very client led, giving the client a sense of ownership.
I think it allows much more freedom on behalf of the therapist to be able to listen more intently
so that the focus really comes from the client and not from the therapist (P1)
I felt that she didn’t sort of denigrate what I might have wanted to talk about she didn’t say to me
‘oh no that’s not – lets go back and talk abut your childhood’ but we did talk about my childhood
as well but it was done in a natural way – it was done in a way that I would bring a topic, and
then we would look at it from all angles. (P5)
P1 explains that because the focus comes from the client, the therapist has the opportunity to
really take in what the client is saying. P5 comments that her therapist did not lead the
discussion, but allowed it to come from her. She appeared to perceive this as positive; as she
notes that the alternative would have been to ‘denigrate’ what she said.
58
P3, a counselling psychologist in training, said that her therapist showed her that people: are
trying to do two things, the one is to forget that they are just thrown here without knowing why,
and the other is to create a meaning that is going to be quite strong for their whole life uhhhh
and push convince themselves that they found the meaning out there, like convince themselves
that it was not there that they created it, that it was out there and they found it (P3).
P3 went on to link this to client responsibility when she said: so at the moment although it made
me feel a bit better it still was very heavy for me to realise that it depends on me, it’s kind of
taking responsibility as well and err this was the reason that I wanted to be in therapy with an
existential therapist. (P3)
While P3 explains that the concept of taking responsibility underpinned her decision to take up
therapy within the existential modality, she appeared to find it simultaneously reassuring and
challenging, as she realised that the meanings that she creates ‘depends on me’.
A lack of defined structure
Along with the experience of the direction largely emanating from the client, some quotes
describe a lack of defined structure or way of working to the therapy, and a sense of an open
space within which to work.
P6 describes existential therapy as ‘open landscape’, with no specific way of how things should
be done, but also describes the unstructured way of working as a sense of possibility, and
appears to find it liberating.
In existential therapy there’s no set sort of idea about how it needs to be done, it’s much more
sort of open landscape than that. I think there’s a sense of possibility that’s in there, that there’s
no dogma that one’s sort of working around, instead it’s very free. (P6)
P2, who was in psychotherapeutic training with an existential focus at the time of receiving
existential therapy, talked about his experience of working within a big space as a less positive
experience, and reported that it felt too big and lacked focus:
… it was more just trying to get a grip on something where there were just no foot holes really,
of trying to climb up a wall where you know there’s just nothing to hold onto- it just felt there was
nothing to hold onto that I could pull myself up on (P2)
You know there’s a lot of focus on the authentic and the individual and not having manuals and
not following particular practice guidelines, you know it was just somebody doing whatever they
felt like at the time. (P2)
P2 explains his frustration that there was actually too much space for him in the therapy room,
59

which he appeared to feel did not give him something tangible to work with. For him, the space
seemed to be quite uncontaining. While he acknowledges that authenticity was in place and the
therapy worked around the individual, it did not appear to be enough for this participant: the
open nature of the therapy just seemed to feel like a form of improvisation on behalf of the
therapist.
I feel that it’s very open, the therapy with the existential therapist, it’s everything, she will explore
everything in the same way it’s not that she’s going in a specific direction. In the beginning it
was feeling very anxiety provoking – and there were times that I was impatient ‘what what are
we doing here? I need to find out, to find out all the time to find out all the links like that,
although now it feels that without trying things are coming up. (P3)
P3 also expresses frustration about the lack of structure, and claims to have found the
experience quite anxiety provoking initially, although over time, the links that she was searching
for begin to appear for themselves.
Being in the present
Some participants commented that their experience of existential therapy was very much
concerned with living in the present moment and the future.
P3 conveys that her therapist works very much in the present moment: She is about being in
the moment and about accepting this really and working with the here and now (P3)
P1 who was in psychotherapeutic training with an existential focus at the time of interview,
describes existential therapy as future focused: the therapist considers present issues in terms
of how they impact upon the future: The existential part of the therapy it’s not grounded in the
past, it’s dealing with issues of now and sort of allowing me to focus on well, which way do I
want to take whatever the problem’s about or the issue, you know, what options are open to me
and which way do I want to go with it and I select one way or the other, how is that going to
impact on anything else in the future. So it’s very future focused. (P1)
P4 also discussed being in the present in some depth:
The existential stuff in therapy I’ve found is solely about living in the present and my attitude
towards the future, yeah I mean my attitude towards the past as I carry it with me today but it’s
been so much more applicable to my relationships today. (P4)
I can’t live in that past time, I’m aware I carry it with me you know whatever memory I have of
the past is always with me but it is only a memory and my memory today might be different than
it is tomorrow. The real past has gone, so this is the other thing about the existential therapy I
don’t live in the past so much anymore, and something err something I noticed with this
60
therapist that I have just now is he hardly ever even now has asked me about my family, my
upbringing, simply because it wasn’t material I was bringing. I found that in the existential mode
there’s been hardly any emphasis on that, unless I’ve chosen to bring something. (P4)
It is possible that P4 perceives the past as a burden that he carries with him, but he appears to
attribute not living in the past so much to the existential work he has done. He comments that
the therapist did not actively pursue a dialogue about his past, unless it was material that he
brought to the session, which again highlights the client led element of existential therapy. P4
however is not discounting the past, but states that it is more his ‘attitude towards the past as I
carry it with me today’, just as May and Yalom (1995) commented that one’s world includes the
past events that condition one’s existence, but it is these as one relates to them, as one is
aware of them, moulds, and constantly reforms them, for to be aware of one’s world means at
the same time to be designing and constituting one’s world.
Difficult to Define
While participants have offered an insight into what they conceive as the existential elements of
the therapy, some participants struggled to directly see or explain what was particularly
existential.
P2 questions what was existential about the therapy that he received, finding it more as a
‘directionless conversation’, and goes on to say that it is not clear in general what an existential
therapist does.
There was nothing that actually would stand out to make this person an existential therapist, it
was just a directionless conversation, there was nothing, in sharing this with you I’m thinking
about this, you know this isn’t some – you know - where was the existentialism in that? (P2)
I don’t know actually I’m sure there’s a lot of good existential therapists out there but I don’t
know really, I don’t know I mean generally I don’t think anybody really knows what they do um
it’s not really clear what an existential therapist does. It’s very under specified in terms of the
literature about what it is, I think sometimes it um you know it’s just very vague, what it is and
what it means. (P2)
P4 comments that it is difficult to articulate the experience and say exactly what was existential
about it: It’s really hard to put it into words and explain it to you now in a way, how it was
existential exactly (P4)
P3 also comments that at times she can see that the therapy is very existential, whereas at
others it could seem person-centred.
61
It is very very existential, so in some sessions you can see that, in others it can feel very
person-centred you could not say that it’s existential I guess you know it can be it depends on
what I bring (P3)
Perhaps this reflects a bigger issue, in that existential therapy is hard for people to define.
However it also perhaps exemplifies the significant personal nature of this experience; that can
be ultimately hard to put into words.
Paradoxes of Thinking
The super-ordinate theme ‘Paradoxes of Thinking’ refers to a collection of paradoxes which
emerged during the analysis of the transcripts and is inclusive of themes intellectual but
unknowing, and unconnected but connected.
Intellectual but Unknowing
Some quotes referred to intellectual discussions and philosophical debate, while others
maintained that things were not over intellectualised.
P6 initially raises the importance of the philosophy to him, the prevalence of philosophical
discussions during his therapy sessions, and appeared to feel that this underpinned his reasons
for choosing this kind of therapy.
I think the philosophy’s critical. I mean I have existential ideas of my own to begin with which is
why I took that route, and I’d already done some philosophy so those ideas I suppose travel into
the room with me and they are of course part of her approach. But it is quite a philosophical
process I think for sure because I find myself speculating a lot in there and she’s up for the
speculating: what is meaning, where is the meaning held, who has the meaning, that sort of
thing. (P6)
P1 also talks about the philosophy as an aspect of the therapy that she liked. She discusses
working with the existential dimensions in therapy which she thought the approach highlighted:
I really like that the therapy involves philosophy, I think if you look at different dimensions in life
you know we’re all affected by physical social spiritual personal dimensions really and events
and things that happen in your lives and I think this is the first approach, existentialism is the
first approach that really highlights these four areas. (P1)
P6 goes on to highlight a risk of the therapy becoming a debate, of existing too much in the
mind, and underlines the importance in his opinion that the therapist is aware of this also, so as
62

not to lose sight of the encounter within the room:
I believe that there’s a danger for somebody like me who lives in my head an awful lot and is
fairly verbose as you can hear, to find myself in the room with somebody who is existential and
is interested in the philosophy, sometimes we can both end up debating and so much can be in
the mind. I would say built into the approach is a risk that for those that are quite in their head or
mechanical in their thinking or or edit and filter things via their mind, then with the wrong
existential therapist I’m sure you could get into a real rats nest of hours of debate. But I think
most properly trained existential therapist it very much comes back to the quality of the
encounter and what’s actually happening in the room in its totality – not just an exchange of
ideas. (P6)
P5 acknowledges that intellectual discussions take place, but they only go so far before coming
back to how this relates to her in real terms. P4 appears to support this view as he describes
discussions about philosophers but maintains that they go beyond an intellectual discussion, as
the therapist uses it in relevance to where they are at the time.
What’s interesting is yeah we do have sort of quite a lot of if you like almost some intellectual
discussions sometimes, and we don’t pretend that isn’t happening, but it won’t be very long
before we come back into why is that important for you to think or feel like that, how does that
relate to your relationship with your husband (laughs) do you see what I mean? (P5)
Well we err when we’re chatting he’ll make reference that Sartre would say this and Heidegger
would say that… but he’s not sitting there talking purely about Sartre and Merleau-Ponty you
know he is dragging on all sorts of stuff and bringing it into where we are (P4)
While there is a place for intellectual discussion and some participants found it helpful, there is
also discourse around the use of working within the unknowing. For instance, though talking
about philosophical discussions within therapy, P5 also mentions her therapist’s focus on
staying with the unknowing, and challenges her need to know everything.
No it’s just sometimes we might talk about the philosophy, so she might say ‘oh in existentialism
we think like this’. She might do that, not really often, but she might say for example ‘in
existentialism it’s very important to stay with unknowing, you know, do you have to know
everything’. (P5)
P3 also discusses this in terms of an acceptance of how you feel at the moment, and adds that
by accepting there is no real or right way, the explanation paradoxically manifests.
And another thing it’s the acceptance it’s like calling you, inviting you to accept how you feel at
the moment, without judging it too much and without explaining too much at the moment, and
then paradoxically the explanation comes itself, after that, which has been very helpful for me,
63
that I don’t have to find why this is happening now, it’s less focused on intellectualising it’s not
intellectualising. (P3)
Therefore this theme perhaps conveys the significance of the underlying philosophy of
existential therapy and the intellectual nature of the work, but also paradoxically a
acknowledgement that there is value in working without the answers, abandoning the
explanations, and allowing a solution to present itself through an acceptance of the present
moment.
Decompartmentalisation leading to Connection
P5, a counselling psychologist in training, revealed a different paradox of sorts, by referring to a
sense of connection that she began to find for herself in therapy, after the therapist had
decompartmentalised her life in other ways. It appeared that as a result of the therapist
decompartmentalising aspects of her life in therapy, it allowed her to independently begin to
make connections and see things holistically for herself.
First, she explains that something important about existential therapy is that it does not
compartmentalise you, but unifies your different roles across varying time spans.
But what I want to hold this thought as it’s something I think is important about existential
therapy, is that what it tries to do is it doesn’t try to break you down into all these component
parts as far as I, well my therapy isn’t put it that way, I feel it provides not only a thread across
time but also a thread across my different roles, and how I am able to be in the world. (P5)
However, as she goes on to explain in the second quote, it does this by acknowledging her
different roles yet also inviting her to consider how something that affected her in one role also
impacted on her in another role.
So all the things that I probably came to therapy thinking that this is my sort of self as a mother
this is my sort of self as a somebody’s work force, I couldn’t really see the connection always
between them, and I think what therapy’s done is allow me to see myself within all those
different roles. So she will sort of try to shine a light on, so I’m talking about work and she will
say so how did that affect your life outside work. If I’m talking about my studying she’ll say how
did that affect… so she sort of sees me as the same person across everything, which has
helped me reflect back and see myself as the same person across everything as well. (P5)
There is this idea of a thread of you across everything, rather than having to be different things
in different compartments of your life. It decompartmentalises things as far as I’m concerned, it
sort of makes everything connected, and me within it connected. (P5)
She’s seen all these different compartments but also a thread through my development, and
64

that’s been helpful, to see things holistically (P5)
For this participant, it appears that segregating her roles in life has helped her to acknowledge a
more constant thread that intertwines them, In this way she found that the therapy
decompartmentalised her life, and yet paradoxically appeared to give her a sense of being very
centred and connected.
Discussion
This study provided a qualitative analysis of the client experience of existential therapy. The six
participants have disclosed some of the aspects of therapy that had stood out to them and
revealed some interesting paradoxes of thinking, which could be useful implications for
counselling psychology and future research.
IPA was considered suitable because of its potential to generate insights into the subjective
experience of existential therapy. There was no hypothesis or prior assumptions, and the
research question was open-ended, making it difficult to categorically state whether it was
answered; yet key features emerged and all themes were supported by multiple examples. IPA
is an idiographic mode of inquiry: while inferences were drawn for this sample, interpretations
for the wider population could only be made with great caution (Smith, Jarman and Osborn,
1999). It should be noted that all participants had received some form of therapeutic training,
which could have impacted upon their experience. The subjective nature of IPA also raises
questions over reliability and validity (Golsworthy and Coyle, 2001), which perhaps could have
been strengthened by having analysis independently checked and interpretations validated, to
ensure the credibility of the final account (Osborn and Smith, 1998). While this research
identifies areas for further exploration, perhaps the findings may have benefited from a larger
sample size while retaining its idiosyncratic focus, and may have been more relevant if the
minimum number of sessions required for participants had been increased, since a thorough
existential approach is most appropriate in long-term therapy (May & Yalom, 2005).
One challenge that stood out in analysis was that while participants highlighted areas of the
therapy that they felt were particularly existential, it appeared to be difficult to define exactly
what existential therapy was. Apparently when discussing the essential components of this, and
perhaps any type of therapy, there is something deeply personal about the experience that is
hard to put into words. Some initial insights into areas that appeared to be significant to
participants have been uncovered, but a more detailed exploration of what was particularly
helpful and why could be useful to practitioners. Perhaps future research could select some of
the areas that participants appeared to find significant, and question what exactly is the added
65

value of discussing philosophy with clients (for example), what philosophical insights have been
helpful to the client, and in what way does this influence the therapy.
It was also found that themes overlapped, for instance the client-led nature of the therapy re-
appeared when discussing the concept of working within an unstructured space, suggesting that
the therapy was not governed by distinct concepts, but rather a fusion of elements. In this way
perhaps the impact of therapists role is left unclear, in that rather than having a rigid perceived
way of working, it is more reflective of Yalom’s (1980) perception of the therapist as a "fellow
traveller" through life, who uses empathy and support to elicit insight and choices. While they
may overlap, it is perhaps important to elicit these themes, in order to attune a practitioner’s
awareness to the impact they can have upon a client. Some aspects such as the lack of defined
structure did not appear to benefit all participants, perhaps illustrating the premise that
existential therapy does not suit everyone, or maybe highlighting a requirement for more
information to be available about the therapy for potential clients. Perhaps the disparity, overlap
and lack of clarity is to be expected, since existential psychotherapy is not a specific technique
or set of techniques. Indeed, van Deurzen (2010) notes that existential therapists are reluctant
to say: ‘This is how you do existential therapy’ because one of the central principles of
existential therapy is that each therapist has to create his or her own personal way of working.
Rather, she comments that existential therapy is an enquiry into meaning based on the same
broad structures that underpin phenomenological research, with characteristic structures,
actions, disciplined interventions and specific skills to guide this enquiry and the task of
existential therapists is to make these their own.
Several participants gave the impression that they did not experience the therapy as labelling.
This perhaps reflects what Cooper (2009) refers to as understanding clients as ‘trans-diagnostic’
beings, which looks beyond a label or category, and considers how a diagnostic label can create
distance between client and therapist. Fletcher (2012) comments that the diagnosis system can
be frustrating, unsatisfactory and restricting in practice, since many of his clients have reported
that no single diagnosis or combination of diagnoses entirely captured their situation. He asserts
that the challenge for practitioners is to consider how to work within the diagnostic way of
working, and cultivate a therapeutic relationship that is less characterised by the stereotypes of
the diagnostic system, but ‘more focused on creating a genuine dialogue that recognises the
autonomy and uniqueness of the other and can be used to acknowledge and explore limitations
and possibilities for wider choice and change (Spinelli, 1989)’ (cited within Fletcher, 2012, p.7).
Some participants indeed appeared to support such views, by describing the rejection of
labelling and dismissal of stereotypes as a liberating experience. Implications for counselling
psychologists could be to consider this dimension of existential therapy and explore how to work
with diagnosis, but without ignoring the individual characteristics and requirements of their
66

clients. The therapist’s aim is perhaps ultimately to consider the client’s issues from an open
stance, for once the client realises that the therapist does not automatically assume
understanding, they are free to investigate their assumptions more carefully (van Deurzen
2002).
Several participants discussed the client led nature of the therapy and the sense of
responsibility that they experienced, although, the emphasis that existential therapy places on
self reflection and understanding appeared to lead to certain challenges. Some participants
appeared to find this way of working frustrating at times, and this sense of self-responsibility
could legitimately be perceived as a challenge by those who wish to rely on the therapist more.
Dryden (2007) notes that there is also an argument that the existential approach attracts clients
who perceive the therapy as leaving them in total control, and points out that such limitations
can only be overcome by a therapist who neither fights the need nor leaves it unchallenged, but
who assists the client in turning such self-reliance into a positive end. Therefore potential
implications for practitioners are to neither encourage the client to regress to a deep level of
dependency nor attempt to become a significant other in the client’s life, becoming more of a
consultant who is there to provide systematic support and allow the client to relate to
themselves more than the therapist (Dryden, 2007).
A theme that appeared to overlap with client responsibility was the sense of working within an
unstructured space, which also appeared to have its challenges for some. However, one
participant (P3) commented that once her initial anxieties were overcome of working in this way,
and realised the extent of her responsibility in the process, the links that she was searching for
began to appear for themselves. Perhaps this reflects Sartre’s (1956) equation of responsibility
to authorship: to be responsible means to be the author of one’s own life design. Facing this
concept of responsibility indeed could be integral to the work, since Yalom (1980) wrote that
acceptance of it enables an individual to achieve autonomy and their full potential. May and
Yalom (2005) highlight the need for the existential therapist to focus upon each client’s
responsibility for his or her own distress, and help clients recognise that they themselves, not
the therapist, must generate and choose among options. While this could be anxiety provoking
and challenging at times, it could also be liberating and empowering. The client process of
taking on responsibility can represent vital moments of therapeutic change as Anderson (1997)
notes, since when a client begins to work collaboratively with the therapist, they slowly achieve
self-agency and a sense of freedom and hope. This does not mean that the therapist abdicates
responsibility, but when the therapist adopts a reflective philosophical stance ‘the dualism and
hierarchy between a client and therapist collapse and responsibility and accountability are
shared’ (Anderson, 1997, p.105). Participants in this study revealed insights into their
experiences of taking responsibility in therapy, at times conveying that this was both reassuring
67

and challenging. Perhaps this suggests a requirement for the therapeutic space to be deemed
safe enough for the client to feel sufficiently empowered and supported while managing this
responsibility, with implications for counselling psychologists to consider how their clients are
given space to achieve this sense of responsibility in their clinical work, how they are supported
in doing so, and how this process might be experienced and managed collaboratively.
Some participants discussed how existential therapy was focused on the present moment, and
less about the past. It could be relevant for future research to capture what was helpful to clients
about defining and discovering meaning in the present and the future, since this temporal
orientation is another major distinction of the existential approach (May & Yalom, 1995). A more
in depth exploration could discover how it feels for a client to work in the present tense, and to
understand themselves from the perspective of what Yalom and May (1995) describe as a here-
and-now cross-section, as opposed to the perspective of a historical longitudinal section. This
could also have pertinence for counselling psychologists in terms of how existential therapy and
mindfulness practice could be used together, since this also focuses on the present moment
and the two practices have many parallels (Nanda, 2010).
A paradox of thinking was observed within the transcripts, with some participants finding the
therapy quite intellectual, containing philosophical discussion, while also getting a sense of
being able to work with the unknowing. This paradox could be useful for counselling
psychologists to have an awareness of, since existential therapy is commonly perceived as an
intellectual approach (van Deurzen 2007), and yet as one participant noted, the answers
manifest for themselves when working within the unknowing and accepting that there is no real
or right way. Additionally, Dryden (2007) notes that some clients are attracted to the approach
with the hope of avoiding senses, feelings and intuition, and therefore a therapist should heed
all these different levels of experience, as full self-understanding can only be achieved through
openness to all different aspects of being. Ultimately, perhaps working within the unknowing,
with the backdrop of intellectual and philosophical discussion, is particularly effective for
existential clients.
Conclusion
This study aimed to capture the client experience of existential therapy. Analysis revealed some
emerging themes that appeared to have significance for the participants, which offers insights
into how existential therapy is experienced from a client perspective and may generate ideas for
future research and implications for counselling psychologists.
Existential psychotherapy perceives the client as an existing, immediate person (May &Yalom,
68

2005) and so it is hoped that counselling psychologists and indeed all psychological therapists
may find it useful to acknowledge the various subjective client experiences of existential
therapy, which could inform their work with a client if they are working existentially, or consider
ways their own practice could potentially incorporate and adapt some of the insights. Therefore
having knowledge of these themes, challenges, and areas of confusion, may help a practitioner
to tune into the client’s perception of working in this way, reinforce the requirement to routinely
elicit clarification, and potentially help to quickly identify ruptures within the therapeutic alliance.
Future research may determine how the themes identified vary across wider populations, with
implications that counselling psychologists may need to identify various subjective
interpretations; recognise their therapeutic value, and be willing to support a client to explore
these meanings.
69
References
Anderson, H. (1997). Conversation, language and possibilities: A postmodern approach to
therapy. USA: Basic Books.
Bende, B. & Crossley, D. (2000). Psychotherapy patients' views of treatment. The Psychiatrist
(2000) 24: 453-456.
Boss, M. (1963). Psychoanalysis and daseinsanalysis. New York: Basic Books.
Boss, M. (1979). Existential Foundations of Medicine and Psychology. Northvale: Aronson.
Bugental, J. (1978). Psychotherapy and process: The fundamentals of an existential-humanistic
approach. Boston: McGraw-Hill.
Butler, S. F. & Strupp, H. H. (1986). Specific and nonspecific factors in psychotherapy: A
problematic paradigm for psychotherapy research. Psychotherapy, 23, 30-40.
Cannon, B. (1991). Sartre and psychoanalysis: An existentialist challenge to clinical metatheory.
Lawrence: University of Kansas.
Cohn, H. W. (1984). An existential approach to psychotherapy. British Journal of Medical
Psychology, 57(3), 11-18.
Cooper, M. (2004). Viagra for the Brain: Psychotherapy Research and the Challenge to
Existential Therapeutic Practice. Existential Analysis, 15, 2-14.
Cooper, Mick (2009) Welcoming the other: actualising the humanistic ethic at the core of
counselling psychology practice. Counselling Psychology Review, 24 (3/4).
van Deurzen, E. (1997). Everyday Mysteries: A handbook of existential psychotherapy. London:
Routledge.
van Deurzen, E. (2002) Existential Counselling & Psychotherapy in Practice, 2nd Edition.
London: Sage.
van Deurzen, E. (2007). Existential therapy. In Dryden’s Handbook of Individual Therapy.
70
London: Sage.
van Deurzen, E. (2009). Everyday Mysteries: A handbook of existential psychotherapy. 2nd
edition. London: Routledge.
van Deurzen, E. (2010). The Framework of Existential Therapy. Skills in Existential Counselling
& Psychotherapy. Sage.
Dryden, W. (2007). Dryden's Handbook of Individual Therapy. 5th Edition. Sage.
Elliott, R. Fisher, C.T., & Rennie, S.L. (1999). Evolving guidelines for the publication of
qualitative research studies in psychology and related fields. British Journal of Clinical
Psychology, 38, 215-229.
Fine, M. (2002). Disruptive Voices: The Possibilities for Feminist
Research. Ann Arbour: University of Michigan Press.
Fletcher, R. (2012). Introduction: Dealing with Diagnosis. In Diagnosis and Beyond: Counselling
psychology contributions to understanding human distress (ed M. Milton). 2012. PCCS
Books Ltd.
Frankl, V. (1959). Man’s search for meaning. New York: Simon and Schuster.
Frankl, V. (1969). The will to meaning. New York: New American Library.
Golsworthy, R. and Coyle, A. (2001). Practitioners accounts of religious and spiritual dimensions
in bereavement therapy. Counselling Psychology Quarterly, 14, 183-202.
Langdridge, D. (2007). Phenomenological Psychology: Theory, Research and Method. Essex:
Pearson Education Ltd.
Lansley, A. (2010). Psychological therapies offered across the NHS. Department of Health.
Retrieved
22
October
2011:
http://www.dh.gov.uk/en/MediaCentre/Pressreleases/DH_116919
Lantz, J. (2000). Meaning centered marital and family therapy: Learning to bear the beams of
love. Springfield, IL: Charles C. Thomas.
71
Lantz, J. (2001). Depression, existential family therapy and Viktor Frankl’s dimensional ontology.
Contemporary Family Therapy, 23, 19–32.
Lantz, J. (2004). Research and Evaluation Issues in Existential Psychotherapy. Journal of
Contemporary Psychotherapy, Vol. 34(4) 331-340.
Lantz, J., & Gregoire, T. (2003). Existential trauma therapy with men after a heart attack.
Journal Contemporary Psychotherapy, 33, 19–33.
MacCormack, T., Simonian, J., Lim, J., Remond, L., Roets, D., Dunn, S. and Butow, P. (2001),
‘Someone who cares:’ A qualitative investigation of cancer patients' experiences of
psychotherapy. Psycho-Oncology, 10: 52–65.
Macran S, Ross H, Hardy GE, Shapiro DA. (1999). The importance of considering clients'
perspectives in psychotherapy research. Journal of Mental Health, 8(4), 325-337.
Mahrer,A. (2000). Philosophy of science and the foundations of psychotherapy. American
Psychologist, 55, 1115–1125.
May, R. (1983). The discovery of being. New York: W.W. Norton.
May, R. (1995). Discovery of being. New York: Peter Smith.
May, R. (1996). Psychology and the human dilemma. New York: Norton.
May, R., Angel, E., & Ellenberger, H. F. (1958). Existence: A new dimension in psychiatry and
psychology. New York: Basic Books.
May, R., & Yalom, I. (2005). Existential psychotherapy. In R. J. Corsini & D. Wedding (Eds.),
Current psychotherapies (7th ed., pp. 269-298). Belmont, CA: Brooks/Cole- Thomson
Learning.
Nanda, J. (2010). Reflections on Mindfulness Based Cognitive Therapy (MBCT) and a Case For
Mindfulness Based Existential Therapy (MBET). A Single Case Illustration. Existential
Analysis 21.2.
Mullan, H., & Sangiuliano, I. (1964). The therapists contribution to the treatment process.
Springfield, IL: Charles C. Thomas.
72

O’Connor,, T.J., Meakes, E., Pickering, R., Schuman, M. (1997). On the Right Track: Client
Experience of Narrative Therapy. Contemporary Family Therapy, 19(4), 479-494.
Osborn, M. and Smith, JA (1998) The personal experience of chronic benign lower back pain:
An interpretative phenomenological analysis. British Journal of Health Psychology 3, pp.
65-83.
Rowland, N. & Goss, S. (2000). Evidence-based Counselling and Psychological Therapies:
Research and Applications. London: Routledge.
Sartre, J. P. (1956). Being and nothingness. New York: Philosophical Library.
Schneider, K. J., & May, R. (1995). The psychology of existence: An integrative, clinical
perspective. New York: McGraw-Hill.
Smith, J. A. (1996) Beyond the divide between cognition and discourse: using interpretative
phenomenological analysis in health psychology. Psychology & Health, 11, 261-71.
Smith, J. A. (2008). Qualitative Psychology: A practical guide to research methods. London:
Sage.
Smith, J.A. and Eatough, V. (2006) ‘Interpretative phenomenological analysis’, in G. Breakwell,
C. Fife-Schaw, S. Hammond and J.A. Smith (eds) Research Methods in Psychology, (3rd
edn). London: Sage.
Smith, J.A., Flowers, P. & Larkin, M. (2009). Interpretative phenomenological analysis: Theory,
method and research. London: Sage.
Smith, J.A., Flowers, P. and Osborn, M. (1997) ‘Interpretative phenomenological analysis and
health psychology’, in L. Yardley (ed.), Material Discourses and Health (pp. 68–91).
London: Routledge.
Smith, J.A., Jarman, M., & Osborn, M. (1999). Doing interpretative phenomenological analysis.
In M. Murray & K. Chamberlain (Eds), Qualitative health psychology: theories and
methods (pp.218-240). London: Sage.
Smith, J.A. & Osborn, M. (2003). Interpretative phenomenological analysis. In J.A. Smith (Ed),
73

Qualitative psychology: A practical guide to methods (pp. 51-80). London: Sage.
Smith, JA (2004) Reflecting on the development of interpretative phenomenological analysis
and its contribution to qualitative research in psychology. Qualitative Research in
Psychology 1, 39-54.
Sonneman, U. (1954). Existence and therapy. New York: Grune and Stratton.
Spinelli, E. (1989). The Interpreted World: An introduction to phenomenological psychology.
London: Sage.
Uhlmann, E.L. & Cohen, G.L. (2007). “I think it, therefore it’s true”: Effects of self-perceived
objectivity on hiring discrimination. Organisational Behaviour and Human Decision
Processes, 104(2), 207-223.
Whitaker, C. (1976). The hindrance of theory in clinical work. In P. Guerin (Ed.), Family therapy.
(pp. 154–164). New York.
Wilkes, R.S., & Milton, M. (2006). ‘Being an existential therapist’: an IPA study of existential
therapists’ experiences. Existential Analysis, 17(1), 71-82.
Willig, C. (2008). Introducing Qualitative Research in Psychology (2nd ed.). Berkshire: Open
University Press.
Yalom, I. (1980). Existential psychotherapy. New York: Basic Books.
Yalom, I. D. & Elkin, G. (1990). Every day gets a little closer: A twice told therapy. New York:
Basic Books.
74
Table of Appendices
A. Ethical Approval Form
B. Participant Information Sheet
C. Consent Form
D. Interview Prompts
E. Risk Assessment
F. Web Request
Appendix A: Ethical Approval Form
ETHICAL APPROVAL FORM
1.
Title of Proposed Research:
An Investigation into the Experience of Existential Therapy for a Client using Interpretative
Phenomenological Analysis
2.
Name of Investigator:
Lisa Corbett
3.
Organisation in which the research will be conducted:
University of Surrey.....................................................................…………………………………..
4.
Do you need permission from the organisation in which the research will be conducted and
how do you intend to secure this?
None
5.
Do you need to gain consent from an Ethical Committee within the organisation or external to
the organisation?
75
University of Surrey approval
6.
How are you going to recruit your participants?
The participants will opt in to the study by means of a poster campaign and online publicity
through forums with an existential interest
7.
How will you ensure that your participants are able to give their informed consent to
participate in your study?
A participant information sheet, including risk assessment, will be provided in advance of the
study.
8.
What opportunities will your participants have to withdraw at any time from the study and how
will you inform them of these?
The participant will be informed in advance via the participant information sheet (including an
informed participant risk assessment) that they can withdraw at any time from the study. At the
interview they will be advised that they can withdraw from the interview at point without
reason.
9.
What data gathering procedures are you intending to use in your study?
Participant semi-structured interviews
10. Could any aspect of your study cause distress, anxiety, guilt, offence or pain to your
participants?
Yes
11. If yes, how do you justify this and what may be done to minimise these consequences?
This research is justified by increasing the knowledge and understanding of the client
experience of existential therapy. Distress will be minimised by participants opting in to the
study; informed consent including risk assessment and applying the principles of person-
centred counselling including empathy, genuineness and unconditional positive regard in
76
conducting interviews.
12. Is there any deception involved in your study? If yes, how do you justify this?
No
13. What feedback will you give to your participants and when?
A summary of results of the study will be offered to participants on submission of the study to
the University of Surrey PsychD Programme.
14. How will you ensure confidentiality of the information you obtain during your study?
Transcripts will be made anonymous, and all reasonable steps will be taken to safeguard the
security of interview audio-tapes until the end of the data analysis procedure at which point
they will be destroyed
15. Do you foresee any other ethical problems and how will you address these?
None
_________________________________________________________________________________
___
This sector to be completed by Research Supervisor and a copy retained in the trainee's personal file:
I foresee no ethical problems with this research
Signed .................................................... Date ....................................
I advise that this trainee should seek ethical approval from the Faculty Ethics Committee (and, where
necessary, another relevant ethics committee) (in the event of potential difficulties)
Signed .................................................... Date .....................................
77
Appendix B
Participant Information Sheet
University of
Surrey
Guildford
GU2 7XH
Title of Research Project:
The Client Experience of Existential Therapy
Brief description of the Research:
My name is Lisa Corbett and I am a second year student on the PsychD Counselling
Psychology doctoral programme at Surrey University.
This study is designed to explore the ways in which clients have experienced existential therapy.
There are a number of studies which have looked at existential therapy; however these studies
have focused on the therapists’ experience. This research proposes to explore how clients
experience this therapeutic approach.
It is hoped that the information which is gathered from interviewing a small number of
participants will provide a client-led perspective to emerge within the existential literature and
may provide insights into the perception of existential therapy.
Thank you for expressing an interest in participating in this research. If you do decide to
participate in this study the following information will inform you of what the process will involve.
This study has received a favourable ethical opinion from the Ethics Committee of the Faculty of
Arts and Human Sciences at the University of Surrey.
What will be expected from you as a research participant?
Participation in this research will involve meeting with the researcher for a semi-structured
interview, at a time and place convenient for you.
The interview will normally last somewhere between 30 minutes and one hour – and will be
audio recorded. This recording will be deleted once the interview has been analysed,
You have the right to withdraw from the study at any time without giving a reason up until the
point of data analysis. All data will be handled in accordance with the Data Protection Act
(1988).
78
Your confidentiality will be maintained provided the information you provide falls within the
British Psychological Society’s (BPS) and the Health Professions Council’s (HPC) ethical
guidelines.
The interview will be transcribed and your name and any other identifying information will be
removed. You will be given the opportunity to read the transcript and to alter any information
which you feel is inaccurate.
You will be required to sign consent forms before the interviews; you will be given copies of
these.
What will be covered in the interview:
1) You will be invited to give a general account of your experience of existential therapy.
2) You will be invited to contribute any other information which you think is relevant to this
research.
Risks
Since you will be discussing your therapeutic experience, there is a risk that you could
talk about sensitive material. If this is the case, you can stop the interview at any time,
request a break, and have the opportunity for a full de-briefing following the interview.
If you need any further clarification or have additional questions, please do not hesitate to
contact me.
Yours sincerely,
Lisa Corbett (Trainee Counselling Psychologist, University of Surrey)
Researcher contact details:
Lisa Corbett
Trainee Counselling Psychologist
University of Surrey
Guildford
GU2 7XH
Email: l.corbett@surrey.ac.uk
If you are unhappy with any aspect of how you have been treated in the research, please
contact my supervisor:
Dr Martin Milton
University of Surrey
Guildford
GU2 7XH, Email: m.milton@surrey.ac.uk
79

Appendix C
The Client Experience of Existential Therapy
Consent Form
1) I the undersigned voluntarily agree to take part in the study on the Client Experience
of Existential Therapy
2) have read and understood the Information Sheet provided. I have been given a full
explanation by the investigators of the nature, purpose, location and likely duration of
the study, and of what I will be expected to do. I have been advised about any
discomfort and possible ill-effects on my health and well-being which may result. I
have been given the opportunity to ask questions on all aspects of the study and have
understood the advice and information given as a result.
3) I agree to comply with any instruction given to me during the study and to co-operate
fully with the investigators. I shall inform them immediately if I suffer any deterioration
of any kind in my health or well-being.
4) I consent to my personal data, as outlined in the accompanying information sheet,
being used for this study and other research. I understand that all personal data
relating to volunteers is held and processed in the strictest confidence, and in
accordance with the Data Protection Act (1998).
5) I understand that I am free to withdraw from the study at any time without needing to
justify my decision and without prejudice.
6) I confirm that I have read and understood the above and freely consent to
participating in this study. I have been given adequate time to consider my participation
and agree to comply with the instructions and restrictions of the study.
Name of volunteer (BLOCK CAPITALS)
........................................................
80

Signed
Date
........................................................
......................................
Name of researcher/person taking consent (BLOCK CAPITALS)
Signed
........................................................
Date
......................................
Researcher contact details:
Lisa Corbett
Trainee Counselling Psychologist
University of Surrey
Guildford
GU2 7XH
Email: l.corbett@surrey.ac.uk
Appendix D: Interview Prompts
Could you give an example?
Could you elaborate on that?
How do you experience that?
Why was that?
What are your thoughts on that?
Participants were given the opportunity at the end to say anything further on the subject that had
not been talked about and whether they had any questions for the interviewer.
81

Appendix E
Risk Assessment – The Client Experience of Existential Therapy
Risks and potential hazards for the participants and the researcher.
Every attempt will be made to provide a safe environment for all involved in the research
project.
The research data collection will either take place in a public centre or in a place agreed by
both parties.
In the event that the research is carried out in a public centre the researcher will check the
health and safety credentials of that centre before undertaking meetings with participants
and to make adequate checks of rooms in which the data collection is to take place in order
to minimize any risk or hazard to both parties.
In the event that the research is carried out in another place this will be the home of the
participants. Prior arrangements will be made by the researcher for a reliable person who
will act as a contact in the event of an emergency; this nominated person will be contacted
before and after entering and leaving the premises by mobile phone which will be
adequately charged.
The participant will be informed before the data collection that it is a matter of university
protocol to log the time of arrival and departure from any address.
Should sensitive material arise, the participant will be given the opportunity for a debriefing
after the interview data collection in order to minimize any risks or hazards to the well being
of the participant.
82
Appendix F: Web Request
I am a doctoral student on the PsychD programme at Surrey University seeking participants for
my research project titled:
The Client Experience of Existential Therapy.
This
research
proposes
to
explore
how
clients
experience
an existential therapeutic approach. Have you received personal therapy for from a therapist
who practises existentially and would you be willing to talk about your experience?
Participation in this research will involve meeting for an interview, at a time and place
convenient for you or a conversation on skype with a webcam if this is more convenient. Your
confidentiality will be maintained and all data will be handled in accordance with the Data
Protection Act (1988).
If you are interested in participating, or in learning more about the research,
please contact me at l.corbett@surrey.ac.uk.
83

The final chapter in the book of growing up: a content analysis of motherhood
experiences
Lisa Corbett
Supervised by Dora Brown
Abstract
This study explored the ways in which the existential dimensions appear in accounts of
individuals who have experienced motherhood for the first time. The research is guided by the
question ‘how do the existential dimensions manifest when women talk about becoming
mothers for the first time?’ Sixteen participants were interviewed, and data was analysed using
Content Analysis (CA). It was discovered that data with the highest frequencies was attributed to
the physical, social, psychological and then spiritual dimensions respectively. Categories
emerged within these domains, which are presented and discussed. Speculative practical and
therapeutic implications for counselling psychology are identified and relevant future research is
suggested.
Key words: motherhood; existential dimensions
84

The final chapter in the book of growing up: a content analysis of motherhood
experiences
Introduction
Motherhood undoubtably represents a crucial transition for women, since a number of
significant personal, social and biological changes coincide (Smith, 1999), making pregnancy,
childbirth and motherhood times of enormous upheaval (Blehar, 2006; Dennerstein, Astbury, &
Morse, 1993). Indeed, motherhood has been identified in the literature as a critical life event that
can bring about many challenges (Barclay et al., 1997; Weaver and Usher, 1997; Nicolson,
1998; Nelson, 2003).
Several studies have documented the stressful aspects of initial motherhood, including parental
fatigue (e.g. Petch & Halford, 2008), increased role-overload (e.g. Perry-Jenkins et al., 2007)
and sudden declines in relationship satisfaction (e.g. Doss et al., 2009). However, Darvill and
colleagues (2008) acknowledge that while a much of the literature depicts particular aspects of
childbirth, there is comparatively less work relating to the transition to motherhood from the
woman’s perspective (Barlow and Cairns, 1997). Of these, Nelson (2003) conducted an
amalgamation of nine qualitative studies concerned with the maternal transition, and
recommended that the primary processes to emerge were ‘engagement’, or being actively
involved and experiencing the presence of the baby (Noblit and Hare, 1988) and ‘growth and
transformation’. Another finding was that women were broadly unprepared to handle
motherhood: the initial postpartum months are described as physically and mentally exhausting;
a time of uncertainty and emotional flux for the mother (Nelson, 2003). A grounded theory study
by Barclay and colleagues (1997) also noticed this theme, and described mothers’
overwhelming feelings, both physically and emotionally, in the early postpartum weeks and
months. Another qualitative study observed that the mothers in the study felt socially isolated
after childbirth (Sethi 1995), while Weaver and Usher (1997) used discourse analysis to
consider aspects of motherhood, and noticed that while the women felt overwhelming love for
their babies, they also found the reality of motherhood significantly different from their
expectations, were overcome by the tedium of caring for infants, and felt that they had sacrificed
part of their identity.
85

Motherhood: a time of growth and transformation
Darvill and colleagues (2008) identified work on the transition of motherhood that discussed the
time as a period of maturational growth. The parenthood transition has been described in some
psychoanalytical literature as a means of providing an opportunity for growth (Parens, 1975),
and Rubin (1961, 1967, 1984) described the cultivation of a mother’s identity as a part of the
maturational process of developing a female identity. Additionally the findings of Pancer et al.
(2000) recorded a growth in complexity of thinking before and after birth and suggested that
parental transition was a time of maturational growth for both parents. Darvill and colleagues
(2008) used grounded theory to explore the transition of motherhood, and identified three main
themes (control, support and forming a family) which all contributed to the core category:
‘changes in the woman’s self-concept’. Women in their study felt that they had lost some control
over their lives in the early stages of pregnancy and after the birth. The unfamiliar process of
early motherhood created a need to seek out others to help guide them and to normalise their
feelings and experiences. Finally, the women acknowledged having their first baby
fundamentally transformed them and their partners from individuals or a couple into founding
members of a new family.
Existential Research and the Existential Dimensions
Existential research is one of the most under-researched approaches in counselling and
psychotherapy (Cooper, 2004). However a small amount of research has been done to explore
motherhood from an existential perspective. Adams and colleages (2006) applied key concepts
from existentialism as a theoretical framework to address sexual intimacy for new mothers and
considered the issue from natural, personal, social, and spiritual dimensions of being. This study
will also consider these dimensions in order to explore the experience of first time mothers.
van Deurzen’s developed her existential dimensions (1997) based on Binswanger’s (1958)
work, and they offer a framework for conceptualising clients. van Deurzen (1997) claimed that
‘as human beings we are complex bio-socio-psycho-spiritual organisms, joined to the world
around us in everything we are and do’ (p.94). Essentially, the author describes a four-
dimensional forcefield that we are constantly concerned with: physical, social, psychological and
spiritual. The dimensions begin with the relationship between ourselves as a physical body and
the natural environment: the biological forces that regulate us within the physical dimension.
Secondly, the author describes the social dimension: our social and cultural network through
which we relate to others. We are thirdly modulated by the psychological dimension which
concerns our personality, character and mental processes, and finally by our relationship to the
framework of meaning through which we experience and conceive the world on a spiritual
dimension (van Deurzen, 1997). The four dimensions within which existence takes place span
polar opposites manifesting as paradoxes, dilemmas, contradictions and conflicts; each with
86
connections and overlaps which may prevail when considering their implications in relation to
experiences of motherhood.
While the impact of motherhood has been of great interest among researchers, limitations have
been noticed. Smith (1999) highlighted reviews of research on the psychology of motherhood
(e.g. Entwisle & Doering, 1981; Ussher, 1989; Scott & Niven, 1996) which revealed that most
followed prescriptive or obvious routes defined by the parameters of particular subject
disciplines. Smith (1999) observed that typically the pathological is stressed, at the expense of
the ‘normal’ so that typical studies concentrate on ‘maladaption’ to mothering, with an emphasis
on illness or pathology, neglecting the range of possible experiences undergone by first time
mothers. This study explores experiences of motherhood, not in relation to any underlying
pathology or psychological difficulty, but in order to discover how this life change might affect a
mother in terms of the existential dimensions.
Research Question
This study explores how women talk about their experience of motherhood in terms of the
existential dimensions, in order to enhance practitioner awareness in this under researched
area and potentially inform those considering an existential approach. Such an exploration could
challenge assumptions and add to our understanding of individual experiences and perceptions
of motherhood. This could in turn help trainees and therapists reflect upon and evaluate their
therapeutic style when they have a client who has experienced motherhood – an important
focus for counselling psychology. With these principles in mind, the research was guided by the
question ‘How do the existential dimensions manifest when women talk about becoming
mothers for the first time?”
Method
Sample
Sixteen participants in total opted into the study, all of whom had experienced childbirth within
the last three years. By limiting the sample this way, it was hoped that the experience would be
relatively fresh in their mind and hopefully ensuring that they will be able discuss the experience
in some depth, promoting the likelihood of securing a relatively homogeneous sample and
thereby increasing the likelihood of being able to discern commonalities of viewpoint and
reported experience. The participants babies’ ranged in age from 2 weeks to 2 years and 9
months, and the average age of the babies across all participants was 17 months.
The study was publicised in two ways - by posters placed in postnatal class venues and on
website forums that held an interest for new mothers (appendix A). Postnatal groups were also
87
contacted and requested to publicise the study. Participants who expressed an interest were
given an information sheet containing the title and brief description of the research (appendix B).
If they agreed to participate, a consent form was signed (appendix C).
Data Collection
Interviews followed a semi-structured schedule designed to elicit different aspects of
participants’ experiences of motherhood. The interview schedule consisted of a set of questions
which were initially generated from the literature describing the existential dimensions (van
Deurzen, 1997) and discussed in supervision to ensure the likelihood that they represented the
relevant dimensions without enforcing any assumptions and allowing the participant room for
interpretation. These are presented below in Table 1.
Table 1: Sample interview questions
1- How did you find becoming a mother in terms of your body?
2- How did you find looking after your first baby in the initial weeks?
3- How did you look after yourself and attend to your needs after having your first baby? (if at
all?)
4- How was the experience of becoming a mother on your social life (if so, how?)
5- Were your close relationships / family affected when you became a mother (if so, how?)
6- After becoming a mother yourself, how did you relate to other mums?
7- How did you see yourself after becoming a mother?
8- How does this compare with how you saw yourself before becoming a mother?
9- How do you see yourself in the future?
10- Would you say that becoming a mother plays a role on your outlook on life (if so, how?)
11- on your beliefs (if so, how?)
12- on your values in any way (if so, how?)
The questions themselves were designed to focus on the physical, social, psychological and
spiritual dimensions, and each dimension was assigned three related interview questions
although analysis explored if and how these themes present themselves across all the
questions. . The questions were non directive and avoided assumptions, and were discussed in
supervision to ensure they were checked for fairness and open-endedness. Participants were
informed that they did not have to answer any questions if they did not feel that they related to
them. Interviews lasted approximately twenty minutes. At the beginning of sessions, it was
explained to participants that the research was confidential and that they could end the interview
at any time should they wish. Participants were advised that they did not have to answer a
question if they did not feel it was relevant to them. Each interview took place in a quiet meeting
88
place at a time and place convenient for the participant, digitally-recorded with consent and then
transcribed verbatim. The recordings were then deleted. Since Prior (2003) had argued that any
form of written material could be used in research to investigate and understand ideas which
influence human behaviour, participants were also given the option of completing the questions
electronically, hopefully to facilitate the process for first time mothers who might struggle for time
otherwise. In such instances, the interview questions were emailed to participants so that they
could complete them at a convenient time and return them to the researcher.
Data Analysis
The emphasis of the study was to offer insights into experiences of first time motherhood and
therefore a qualitative research method is adopted. CA was selected as the favoured method to
analyse the interview transcripts and written material. CA has been described as a systematic,
replicable method that allows the analysis of larger quantities of text to be compressed into
content categories based on explicit rules of coding (Holsti, 1969; Krippendorff, 1980; Weber,
1990). Holsti (1969) has provided an overall definition of CA as “any technique for making
inferences by objectively and systematically identifying specified characteristics of messages”
(p.21). The premise is that words, phrases and sentences (coding units) that reappear
frequently in the material are those reflecting important concerns in every communication
(Weber, 1990).
The method of using CA for this study was informed by Brown and colleagues (2009). Using CA
typically requires a frequency count, and the technique relies on categorisation and coding of
data so initially the unit of analysis had to be defined. A category is understood to be a group of
words with similar meaning and coding units are generally words, sentences or paragraphs
(Weber, 1990). Categories in this study were not mutually exclusive or exhaustive, and coding
units were notional sentences in that they represented a thought or expression of an idea.
Coding was done by repeatedly reading through the data sources and assigning coding units to
a category. Primary categories were already pre-established as the existential dimensions
(physical, social, psychological and spiritual), but additionally sub-ordinate categories were
generated from the data. The organising principle in the selection of themes was that of
counting frequencies. Prior to analysis, to promote consistency of coding, emerging coding was
carried out to explore and identify sub-ordinate themes and to verify inter-rater reliability. In the
first instance, the principal researcher and supervisor reviewed and independently coded two
randomly selected transcripts. The researchers then compared notes, discussed differences
and reached agreement on initial category and domain assignment. They then repeated the
process with another transcript. An inter-rater reliability of 0.93 was achieved which is above the
0.90 level recommended by Miles and Huberman (1994). The researcher then analysed the
89
remaining data sources accordingly and further categories were developed, which were shared
with the supervisor to check for credibility and consistency throughout. During this time the
researcher was careful to bracket any personal thoughts or assumptions about the data in
order to mindfully create space so that the participants' experience could be highlighted.
Evaluative Criteria
Qualitative research is embedded in a philosophy of knowledge development distinct from the
positivist tradition. Whilst positivist research attempts to establish objective knowledge
‘represented as regularities, even laws’ (Elliott et al., 1999, p.217), qualitative research
relativises the knowledge gained to the participants, the situation studied and the researcher.
Therefore traditional evaluative criteria such as validity and reliability become inappropriate.
However, measures were taken to address inter-rater reliability, and the study adhered to the
inter-rater reliability level recommended by Miles and Huberman (1994).
Ethical Issues
Ethical issues were unequivocally considered throughout this study. Participants opted into the
study, and the questions posed were unlikely to cause distress. Therefore the project was not
submitted for academic ethical approval, in line with the guidelines of the ethics flowchart
(appendix D). Participants’ welfare was considered: participants were told they could withdraw
from the sessions for any reason whatsoever, and copies of the written report and transcripts
were available to any participant who requested them. Participants were told they could
withdraw from the research up until the point of data analysis. Pseudonyms have been adopted
to preserve participants’ anonymity and situations that might disclose personal details were
omitted and/or changed with a fictitious equivalent.
Results
Key findings are reported here from the fourteen categories which had the highest frequencies
within each domain. These are supported by verbatim quotes to illustrate statements that
support the identified category. The total frequencies for each are reported in Table 2.
90
Table 2. Domains, categories and frequencies
Domain
Physical
Social
Psychological
Spiritual
Total
Frequencies
479
Categories
Body Image
Body Responsibility
Recovery
Sleep / Tiredness
376
Change
Connection / Disconnection
Impact
Support Networks
296
Emotions
Personality
Identity
102
Prioritisation
Outlook
Hierarchy
Frequencies
81
36
115
58
74
80
96
76
116
51
75
35
34
17
While many areas were discussed by the participants, due to space limitations, the study will
outline and give examples from key categories within each domain that had higher frequencies.
In many cases the categories could easily have applied to more than one domain, but they have
been allotted to the domain that appeared to be immediately paramount to the researcher.
Physical Dimension
The highest frequencies from the data sources appeared to resign within the physical dimension
(459). Within this domain, twelve categories were developed including physical safety,
breastfeeding and sex lives. The categories that emerged with the highest frequencies
concerned body image, body responsibility, recovery and sleep. These are presented here:
Body image
Thirteen participants talked about a change in body image after childbirth, including weight gain,
stretch marks, and changes to the appearance of their breasts. These changes appeared to be
both perceived as positive and negative.
“Pregnancy and childbirth has ruined it, I have skin I don’t think I will ever get rid of” (Annalise)
“I was surprised how much it changed my body, I think it’s better after having Ben. I’m slimmer
91

and generally in better shape.”(Lucy)
Two participants disclosed that their new body image had not concerned them at the time,
because the functionality of their body had taken precedence:
“There was no time to think about appearance, just function” (Mina).
Body Responsibility
Three participants talked about their body in terms of its function and responsibility. One
example highlighted here by Fiona was how she was both intrigued by the way her body was
working for her, but also let down by her body after she had struggled with labour and
breastfeeding:
“I was fascinated by how my body was looking after my baby for me” (Fiona)
“I felt hugely disappointed that my body had failed me when I really needed it as well as at
myself for not having been better able to cope with the labour emotionally too” (Fiona)
In this example, Fiona has described her body as if it is a different entity. Likewise, three
participants admitted a sense that they felt their body was no longer their own:
“During the later months of my pregnancy my body seemed to cease to be my own. Rather a
vessel to house and maintain another. In the early weeks this feeling continued and the sole
purpose of my body seemed to be to nourish and care for another.” (Janet)
Recovery
Nine participants talked about their initial recovery, and discussed pain or discomfort in terms of
the sensations initially after childbirth:
“I’m in bits, my body is so sore. I’m on painkillers but I had second degree tearing and stitches
so it’s hard to walk.” (Zoe)
Five participants talked about neglecting their body to an extent, because there were other
priorities:
“I didn’t feel I neglected my needs as such, just that it wasn’t the right time to have any”
(Melissa)
92
“I wasn’t eating properly – just shovelling food into my mouth now and again to keep going
because everything was about looking after Jessica” (Mina)
However ten participants talked about taking measures to look after their body just after
childbirth:
“I used sleep times well. I didn’t sleep when Tobias slept but I did things like have a nice bath,
paint my nails. Looking after myself like that was important” (Lola)
Sleep/Tiredness
Twelve participants talked about lack of sleep, tiredness or exhaustion:
“The lack of sleep or disturbed sleep was a real shock to the system which took a while to
adjust to… but you do” (Molly)
“Your body runs on adrenaline, and although my body was physically exhausted, to some
extent the sleep deprivation wasn't even noticed” (Frances)
Four participants talked about their babies’ early sleep patterns:
“He sleeps through the night has done since he was 11 weeks” (Helen)
Social Dimension
The second largest number of frequencies was located within the social domain (376). Seven
categories were developed, including areas such as the adaption of social lives, work lives and
support networks. The categories with the highest frequencies related to the change
experienced to social lives, a sense of connection and disconnection to friends, support
networks, and the impact of motherhood on close relationships. These are presented here.
Change
Eleven participants talked about a complete social change following the birth of their first child,
all of whom revealed that their social lives had diminished:
“It definitely changed my social life, I don’t have one now” (Helen)
On the other hand, three participants described how their social life adapted when they were
mothers:
93
“We still meet friends, but the event has to be adapted” (Annalise)
“Instead of going out for cocktails we go to kid friendly places” (Dirona)
Three participants talked about required planning and lack of spontaneity:
“It does however, now mean I can't be spontaneous. I have had to say no to a lot of things, but
planning in advance is the key and a cheap babysitter!” (Frances)
Connection/Disconnection
Ten participants talked about a connection with other mothers, some in a new found empathy for
other mothers, while others talked about more immediate intimacy with other mothers in terms
of conversations and disclosures:
“So if there’s a baby crying in a coffee shop, you look at the mum and know what’s going on for
her. Before I would have just been a bit annoyed probably” (Claire)
“I found myself having intimate discussions about chapped nipples and the energy to have sex
and all sorts of personal things with girls I didn’t know all that long, and the friendships became
real in a way they weren’t before” (Fiona)
However, seven participants also described a sense of disconnection from friends of theirs who
did not have children in that they saw them less or felt as if they did not understand them in the
same way now:
“Everybody says I don't have time for them now” (Dirona)
“I have lost some close friends who don’t have children” (Sam)
Impact
Seven participants talked about the impact that motherhood had on their family relationships
and commented that it had progressed the relationship in some way:
“I’ve always got on well with my inlaws but it was a polite and friendly relationship. Now we have
moved things up a gear since having a baby.” (Fiona)
Six participants also described how motherhood had developed their relationship with their own
mother, in terms of increased understanding or mutual respect:
94

“Having a child has strengthened the bond with my own mother even more, because I
understand what she went through. (Annalise)
Nine participants talked about their relationship with their partner. Of these some described a
stronger bond after they had their first baby, some talked about a sense of becoming a team or
unit now they had become parents, while others described deterioration in the relationship:
“I now have an even closer relationship with my husband” (Sam)
“My relationship with my husband has changed. We're now less lovebirds, in fact barely love
birds at all, and more “team baby” (Tess)
“Daniel and I split up as a result, he left when Tobias was 8 weeks old, I think we realised more
than ever when we became parents that we were never going to make it work” (Lola).
“I think I became very focussed on Stuart and this meant I neglected him and our relationship.
(Bryony)
Support networks:
Eight participants talked about the support they had received from friends and family as a
valuable resource:
“When Adam went to work I made sure my mum came round to help me. Looking back this was
probably vital emotional support as well” (Annalise)
However four participants described this support as a hindrance at times, in terms of conflicting
advice and interference:
“I was given conflicting advice – some told me I should let him sleep. others said I should wake
him” (Bryony)
“I also feel a bit overwhelmed at times with everyone giving advice or opinions on how I should
and shouldn’t do things for my child” (Michelle)
Five participants talked about new support networks in the form of other mothers that they had
discovered since becoming a mother:
95
“My NCT group of other mums made an amazing difference to me. We became and still are a
close group of friends and that was invaluable.“ (Fiona).
Psychological Dimension
Ten categories were developed, including aspirations for the future, expectations, and a new
found sense of responsibility or vulnerability. Categories which had the highest frequencies
emerged relating to the range of emotions experienced by first time mothers, perceived changes
in personality for new mothers, and perceptions regarding identity. These are presented here.
Emotions
All sixteen participants described their emotions on becoming a mother. Of these, nine
participants described motherhood as generally an emotional time:
“it was a tough time emotionally to adjust to all that as well as the new experience of being
pregnant and expecting a new baby” (Michelle)
Some participants talked about specific emotions, for instance six participants talked specifically
about feelings of worry or anxiety, four participants described feelings of anger, five participants
talked about feelings of happiness or contentment, and two participants mentioned feelings of
guilt:
“I’m so worried – I have to keep checking him to see if he’s ok – I’m always alert” (Zoe)
“After becoming a mother I think I have become a bit more irritable with others” (Michelle)
“As a mother I am much happier and more content now” (Bryony)
“These feelings of guilt stayed with me for months after the birth, although after the first week
or two it was put to the background a bit as dealing with a new baby took over.” (Fiona)
Personality
Twelve participants talked about how becoming a mother had impacted upon their personality in
some ways. In particular, seven participants talked about the impact of motherhood on their
confidence both in terms of gains and losses:
“I fell off a cliff in terms of both the day to day stress of making decisions way outside my
96
comfort zone and on my lack of confidence with the simplest tasks (changing, going out in pram
etc)” (Melissa)
“I have grown in confidence as I can’t believe I have managed to be a mum without falling at
the first hurdle!” (Molly)
“I think my confidence has grown – it’s either that or I’ve stopped caring so much about what
people think of me” (Claire)
Additionally, three participants described themselves as being less selfish since becoming a
mother, while three participants talked about becoming more patient since becoming a mother:
“I have become more aware of what others are going through, and therefore maybe more
patient. Patient with myself and others” (Frances)
“I'm much more patient and am learning to enjoy the immediate rather than being impatient for
what's next” (Bryony).
Identity
Ten participants talked about their identity as a mother. Some accepted their new found identity
readily, whereas others describe this as more of an adjustment. Some also mentioned identity in
terms of how motherhood defined them:
“When I am with my child I am see myself as a mother only and nothing else. When I am at
work or out without my child then I am myself with a mother overlay” (Janet).
“It took a while before I started to think of myself as a mum, it was almost a struggle in a way
because it didn’t like the implication that I was just a mum and nothing else.” (Claire)
“Becoming a mother seemed a death sentence to all the things I identified with and to some
extent it was because my definition of who I thought I was was pretty narrow.” (Tess)
Seven participants particularly talked about their identity in terms of the transition from being a
woman without children to becoming a mother. Some talked about being perceived differently by
other people, and others noticed that they were noticeably looked at less in terms of desirability.
“It’s like the way strangers look at you, maybe once you could walk into a room and people
would check you out, or look at what you were wearing, or something like that, but now you get
97
two different looks. They either look at you in that “ohhh how lovely a mum and a cute baby”
look, or they give you the “oh god not another mum and a screaming baby” look” (Claire)
“When I bent over to pick something up in public I would hope my bum might look vaguely nice
in case anyone might notice it. Nowadays I buy high waist jeans, belts and extremely long vest
tops because I spend a disproportionate amount of my time bending over and while I don’t
imagine for a second that anyone might notice my behind, I don’t want to take someone’s eye
out with my builders bum” (Fiona)
While talking about identity, six participants acknowledged that this was difficult to articulate and
put into words:
“I’m just getting used to that- being a mummy. It’s going to take time to get used to and I’m not
sure I can put it even into words” (Zoe)
“It’s hard to say, I think the way I see myself is still changing” (Tess)
Spiritual Dimension
The least number of frequencies were assigned within the spiritual dimension (102). Seven
categories arose including values, beliefs and a sense of the unknown. Categories with the
highest number of frequencies were a sense of prioritisation and hierarchy, and a new outlook
for first time mothers. These are presented here.
Prioritisation
10 participants talked about a sense of prioritisation in their lives now as a result of motherhood:
“The needs of the baby came first.” (Sam)
“Before having maisie all my energy went in to keeping my husband happy and keeping on top
of work but now maisie comes first and having to splash kisses and affection on two people now
is something they don’t teach you at ante-natal classes!” (Molly)
“Finn is just 2, so he can have whatever he needs from me, and Nick can have what’s left over.
The rest can wait, including the housework.” (Fiona)
Hierarchy
6 participants talked in terms of a perceived hierarchy, identifying the place they took in this new
98

hierarchical order.
“Initially though, the baby was my priority to take care of, and I was his priority to take care of,
and he did it well” (Fiona)
“My daughter came first, then my business, then my husband, then me” (Molly)
“All I remember is that no one was asking how I was anymore, they were coming in to check on
my baby. I had suddenly gone from being a priority to being what felt like last in the pecking
order” (Claire)
Outlook
4 participants described a change in their outlook since becoming a mother, and 2 participants
talked about their new outlook in terms of how they saw the world around them now:
“How I look at life going forward will be different for sure now with her” (Michelle)
“I get slightly more anxious about the world’s future e.g. when I read or see things about
war/terrorism and the environment/global warming and wonder if there is more I could do”
(Annalise)
“I see the world as a big place for my children to navigate, but I don’t think I’m cynical or
negative or feeling threatened by any of it for them”. (Fiona)
3 participants described this shift in outlook in terms of seeing a bigger picture, or completing a
piece in a jigsaw:
“I guess before having Amanda I didn’t realise something was missing but now I feel complete.”
(Molly)
“I suppose on one level it feels a bit like my life has been working towards this somehow.”
(Claire)
5 participants talked about a new appreciation of the simple things in life:
“The small things have become much more important” (Bryony)
“You also appreciate the simpler things. A nice day becomes a big deal because you see it
through the eyes of your child and also because you're not freezing at the playground. In a
99

weird symmetry, things that seemed very important such as work related things, become less
important” (Tess)
Summary of Results:
Notional sentences from the data sources could be assigned to each of the existential
dimensions
In many cases there was overlap, and a degree of interpretation was required in order to
select which dimension was the most appropriate category
The domain with the highest frequencies was the physical dimension, followed by the
social, then the psychological and then the spiritual dimension
Within each domain, key categories were also identified. Some of these will now be
considered further in the discussion.
Discussion
The goal of CA is “to provide knowledge and understanding of the phenomenon under study”
(Downe-Wamboldt, 1992, p.314), and this study aimed to explore the experiences of first time
mothers to see how the existential dimensions manifested. CA of sixteen participant transcripts
revealed domains and categories that could fall within the existential dimensions. The highest
frequency recorded in this study was for the first domain: the physical dimension, which
suggested that participants felt that motherhood affected them primarily on a physical level. This
was followed by the second domain which was the social dimension, and then the psychological
and spiritual dimension respectively. This appeared to reflect the order the dimensions are
presented (e.g. van Deurzen, 1997). Indeed, van Deurzen (2002) notes that therapeutically
there is no point in working with a client on the other dimensions unless they can come to terms
with a basic sense of being able to manage their physical existence, which suggests that one
can begin exploring the physical dimension, and work inwards through the remaining domains.
Word limitations prevent a detailed consideration of all results, but aspects from each dimension
will now be discussed, limitations to the study will be presented, and implications for
practitioners and counselling psychology will be considered.
Participants discussed a range of physical demands and in particular the impact that becoming
a mother had on their body. Some described the change as a destruction of their former body,
some experienced the changes positively, and others expressed a fascination with the function
100

of their body. Three participants talked about their body in terms of its function and
responsibility, but perhaps strikingly, they appeared to be describing a sense of body ownership
without necessarily a sense of agency. While these participants appeared to acknowledge that
their body was working for them, they did not seem to have a sense of agency for what their
body does e.g. “I was fascinated by how my body was looking after my baby for me” (Fiona) .
Perhaps this illustrates a diminishing impression of bodily control, disconnection or reduced
sense of agency for some new mothers (see Gallagher, 2000a, 2000b; Marcel, 2003). Walsh
(2009) discussed childbirth in terms of Cartesian Dualism (Davis and Walker, 2008), with the
body becoming the object of dissection and examination. He pointed out that an effect of this
was that the understanding of childbirth became reductionist with women’s bodies becoming
comparable to a machine (Garcia et al. 1990), reflective in diagnostic terms such as “failure to
progress”. Perhaps such reductionism extends to the experiences and perceptions of new
mothers, in some of their attempts to make sense of what is happening to their body while
managing some of the overwhelming feelings and changes during this critical time.
Participants also discussed physical pain, and again at times the body was seemingly described
as a separate entity: e.g. “I’m in bits, my body is so sore” (Zoe). Akrich and Pasveer (2004)
observed that some women dissociated from their physical experience of pain during childbirth,
and such experiences were perceived both positively and as negatively alienating. Walsh (2009)
argued that this illustrates how agency can mean embracing physicality which paradoxically can
be giving in to the body’s primal power (Anderson, 2000) or dissociating as a way of coping with
labour pain. Feelings of alienation however negates agency leaving the new mother in limbo
until she can ground herself with a more meaningful subjective experience (Walsh, 2009). Not
all mothers in this study experienced this alienation or lack of agency, but perhaps for some this
disconnection could reflect potential disorientating feelings that arise after childbirth for new
mothers, and a need for some to find something to re-centre or re-connect with oneself as soon
as possible. When considering therapeutic techniques that might be adopted by counselling
psychologists, mindfulness meditation could be explored, where conscious attention and
awareness are actively cultivated (Brown & Ryan, 2003). Mindfulness involves the use of
focused attention to promote calmness and stability and the first foundation is attention to the
body (Kabat-Zinn, 1990). Such techniques could potentially help a new mother re-centre herself
after childbirth, while possibly also alleviating physical pain, since mindfulness techniques are
recommended as positive pain management techniques in pregnancy and labour (Hughes et
al., 2009).
Within categories that were identified residing within the social dimension, women described big
changes to their social lives, in terms of friends drifting away and new relationships forming.
One emerging category addressed this: disconnection from some friends and a new found
101

connection with others. van Deurzen (1997) writes that we learn to relate to others as a
hierarchy: one way we divide others into categories is by generation and position relative to
oneself, so when adults have children of their own, they find themselves inserted into a new
class of parents, and thus the social dimension is affected. Some participants spoke of the
importance of new support networks experienced after becoming a mother, perhaps in part
because they reinforce this social adjustment and potentially give a new mother a space to
discover their new place within this new hierarchy.
Smith (1999) described the movement from the public to a more personal world and suggested
a shift in focus from the wider circle to the immediate family. Similarly, emphasis for some
participants appears to shift from broader circles of friends to a more intimate world, although
the individuals that make up that personal world vary for each person. Some describe turning to
their partner for support, while others discover a new found bond with family members, or other
mothers (also evidenced in studies by Phoenix (1991) and McLaughlin (1993)). Some
participants described a renewed bond with their own mother, also observed by a Mitchell and
Green (2002) study in which over half of the participants highlighted that becoming a mother
had cemented mother/daughter relations.
Bailey (1999) observed that new mothers described entering into a new network or community
of mothers, and hypothesised that perhaps the process of individuation that dominates womens’
lives recedes to an extent with the onset of motherhood. She notes, however that these
changes were not reported invariably or necessarily described as desirable. Similarly
participants in this study sometimes found their new found support networks a hindrance and an
imposition at times. It could be useful for a therapist to consider the shifting social dynamics
impacting clients, since the changes may reflect more than just an increase or decrease in
social support, but an adjustment to a new role and a new place in one’s social surroundings,
which may bring with it a range of associated challenges for a new mother to manage. This is
possibly a new balance that a first time mother must learn to manage: acclimatising and
integrating herself within new social networks while creating the necessary space around her
new family.
Williamson (2004) wrote “when a woman gives birth, two are born: a baby is born from the
womb of its mother, and a woman is born from the womb of her former existence” (p.235).
Ten participants talked about their identity as a mother, and for some motherhood appeared to
increase their sense of what defined them as a person, while others described a struggle in
adjusting to their identity as a mother. The literature also appears to acknowledge the impact
motherhood can have on a woman’s identity. Raphael (1976) described "matrescence": the
period of change in which a new mother takes on the full responsibility of mothering in the face
102

of numerous changes to her identity and various adjustments in her changing sense of self.
Spier (2001) also discussed the struggles a new mother can face when confronting their new
identity, particularly in terms of work, since her perception of herself as an employed individual
receiving acknowledgement and recognition in the world may be temporarily sacrificed to the
demands of a needy baby on a 24-hour schedule. Some participants talked about their
transition from being a woman without children to a mother, and appeared to believe this
equated to being less desireable. Spier (2001) also commented on a new mother’s sexual
identity as a woman, commenting that there is a dampening effect on feeling sexy and aroused
when children can be heard in the next room.
van Deurzen (1997) writes that out of our experiences on the physical and social dimensions,
we gradually draw a circle around ourselves to protect ourselves as an entity in our own right.
This personal self concept is initially “not well articulated, but it is out of an increasing self-
reflection and definition that we begin to create a private space in our inner world, where a more
circumscribed notion of self can be cultivated” (p.118). Some participants also disclosed that it
was difficult to find the words to describe the change to their identity. Perhaps this reflects the
evolving nature of this period, or illustrates the deeply personal nature of something so
individualised, that is connected with the ongoing developments and challenges within the
physical and social dimensions. Perhaps this suggests an opportunity for therapists to consider
the implications that motherhood could have on their clients’ perceived role or sense of identity.
In this way part of the work may be bringing about an awareness of the impact parenthood may
have on an individual’s sense of self, or integration, so that a new mother does not need to
sacrifice one part of their identity while embracing another all-encompassing one.
van Deurzen (1997) writes that it is on the spiritual dimension “we really come into the true
complexity of being human, as we organise our overall views on the world, physical, social and
personal and generate or are inserted into an overall philosophy of life” (p.123). Few
participants mentioned religious beliefs, and those that did advised that they remained
unchanged. But van Deurzen (1997) notes that this dimension is broadly determined by the
dominant ideology in society, which may or not mean religion: “as we encounter different beliefs
and broaden our minds, we find some of our original convictions to be flawed and begin to alter
our views, adding new beliefs and values to the old ones” (p.123).
Participants discussed a shift in outlook, and five in particular described a new found
appreciation of simplicity. When talking about the spiritual dimension, van Deurzen (1997)
commented that many crave a new sense of meaning that extends beyond the enjoyment of
commodities and the pursuit of health, wealth and self. Likewise, one participant described an
appreciation of the simplest things like a nice day, and accordingly the things that were once
103

important seem less so. Some participants talked about a sense of prioritisation: as their outlook
had shifted, their perception of what seemed important had changed, suggesting that
motherhood does indeed provoke an altered philosophy of life for some. The participants in this
study had all recently become mothers within the last three years, but perhaps it could be
beneficial to also interview mothers some time after the birth of their child, as maybe such shifts
in views occur over a longer period of time and may take longer to become apparent.
As well as prioritisation, participants talked about their place in a perceived hierarchy. The
themes of prioritisation and hierarchy bore perceived resemblances to the hierarchy of human
needs outlined by Maslow (1943,1954): a perspective that considers biological, psychological,
social and environmental domains, proposing that human needs are arranged in a hierarchy
beginning with physiological needs and culminating in self actualisation. Koltko-Rivera (2006)
cited that Maslow (1969) amended his model, placing self-transcendence as a motivational step
beyond self-actualisation, and commented that such individuals seek a benefit beyond the
purely personal and seek communion with the transcendent, perhaps through transpersonal
experiences. Koltko-Rivera (2006) discussed the implications of this further hierarchy: at the
level of self-actualisation, the individual works to actualise their potential, whereas at the level of
self-transcendence, the individual’s own needs are put aside in favour of service to others or to
some higher force or cause conceived as being outside the personal self. Perhaps this is
reflective of the experience of becoming a parent: the dimensions working together in the sense
of a hierarchy, with the physical needs of most immediate importance culminating in a more
spiritual awakening for some co-inciding with the displacement of their own personal needs as
they care for their child.
While the dimensions have been presented independently for the purpose of analysis, they work
together and have connections and overlaps. It was noted that there was overlap during
analysis, for instance aspects concerning identity that were seen initially as psychological, could
also be seen to reside in the social dimension, though this may not be surprising since as
humans we are “complex bio-social-psycho-spiritual organisms” (van Deurzen, 1997 p.94).
Additionally Smith (1999) asserts that it is the change in interpersonal contact that can lead to a
change in the conception of self as related to others: that we are inextricably linked to our social
relationships. In this way a new mother’s increased social contact with significant others helps
to facilitate an increased awareness of their sense of personal identity, which underlines the
interrelation between these dimensions. Furthermore, each dimension contains paradoxes and
tensions, for instance within the physical dimension there is both life and death, and within the
social dimension there is both a sense of belonging and isolation (van Deurzen, 1997). Similarly,
paradoxes were observed within the experiences of first time mothers. For instance, participants
talked about a new sense of belonging to a new network of mothers, while describing alienation
104

from other circles of friends; or talked about experiencing a new sense of confidence in their role
as well as overwhelming doubt. These paradoxes and overlaps may have implications for
practitioners working therapeutically with new mothers, by potentially suggesting a requirement
for a therapist to engage the client with these complexities and understand where contradictions
exist and how they are negotiated, while considering how paradoxes are tolerated. The
dimensions provide a framework in order to conceptualise where a client is experiencing
difficulty, yet as van Duerzen (1988) notes, it is vital to maintain tentative portrayals of a client’s
world, and not be drawn into reductionistic models of the mind or person. It also suggests a
need for practitioners to consider how the dimensions relate to them, and how they struggle with
their own paradoxes, since van Deurzen (1988) writes that there are no short cuts for
understanding clients: practitioners have to be able to allow themselves and their clients to be
exposed at times, and know how to make them safe again.
There are some limitations to this study. Firstly, any generalisation to other groups of mothers
needs to be used with caution, since this study is based on a small sample of new mothers.
Though the demographic information revealed that participants from different ethnicities took
part, there was also a level of homogeneity in that all participants were heterosexual, had
become mothers within the last three years, and the age range across all participants was ten
years. This could further limit the generalisability of the findings, though future research with a
wider sample could reveal similar themes across multiple contexts. Only women were sampled
in this study, thereby limiting the study to one gender. It could be interesting to apply the same
questions to new fathers and consider how (if at all) the existential dimensions manifest in their
accounts of parenthood and how these potentially differ from their female counterparts. This
could potentially reveal subtle differences in the experiences of childbirth which would add
richness and depth to the results already outlined.
Qualitative CA is a research method for the subjective interpretation of the content of text data
through the systematic classification process of coding and identifying themes or patterns
(Hsieh & Shannon, 2005). Therefore this is ultimately the researcher’s impression of the findings
and any inferences drawn should note this limitation. Also the researcher’s own bias could have
affected analysis, since the researcher has read about the existential dimensions and potentially
formed assumptions. There was an attempt to minimise this limitation with supervision during
the analysis, which offered an alternative perspective of the analysis of transcripts.
Since within western society motherhood is frequently romanticised and idealised as the
ultimate physical and emotional achievement (Phoenix and Woollett, 1991), it is always possible
that, in conducting research interviews, there was an element of social desirability in the ways
that women talked about becoming a mother. Furthermore, some of the participants recruited
105

were from the researchers social network, which could have elicited a degree of compliance in
interviews or discouraged a participant from sharing openly. Finally, while participants were
given the option of a face to face interview, the majority preferred the option of electronic
completion of the questions. While CA can be used effectively with more that one data source
(White & Marsh, 2006) this did mean that there was a degree of inconsistency in the way the
data was collected. On one hand this enabled some participants, particularly those who were
new to motherhood and could not set aside time for an interview, to take part. However, these
instances lacked the verbal exchange of an interview, and the opportunities to pause or probe
further as required.
These limitations aside, this study aimed to explore how the existential dimensions manifested
in accounts of new motherhood, to provoke questions and generate further understanding that
could benefit the field of counselling psychology. Motherhood appears to be an experience
unique to each woman, with a range of associated changes, feelings and issues which could be
considered in physical, social, psychological and spiritual terms. While discussions around
motherhood may not be uncommon for practitioners, counselling psychology draws upon and
seeks to develop phenomenological models of practice and enquiry in addition to that of
traditional psychology (BPS, 2005). It is hoped that presenting the experience of motherhood in
terms of the existential dimensions could deepen the existing understanding of a practitioner
working with a client who has recently become a mother, and potentially add a richer layer to
conceptualisation and formulation.
106

References
Adams, L.G., Harper, A.J., Johnson, E.P., Coia, D.C. (2006). New Mothers and Sexual Intimacy:
An Existential Framework for Counseling. The Family Journal, 14: 424.
Akrich, M. and Pasveer, P. (2004) Embodiment and disembodiment in childbirth
narratives, Body and Society, 10, 2–3, 63–84.
Antonuccti,. C. & Mikusk. (1988). The power of parenthood personality and attitudinal change
during the transition to parenthood. In: G. Michaels & W. Goldberg (Eds), The transition
to parenthood: current theory and research. Cambridge: Cambridge University Press.
Barlow, C.A., Cairns, K.V.,(1997). Mothering as a psychological experience: a grounded theory
exploration. Canadian Journal of Counselling 31, 232–247.
Barclay, L., Everitt, L., Rogan, F., Schmied, V., Wyllie, A.,(1997). Becoming a mother: an
analysis of women’s experience of early motherhood. Journal of Advanced Nursing 25,
719–728.
Binswanger, L., 1958. The case of Ellen West. In: May, R., (Ed)., 1958. Existence, Simon and
Schuster, New York, pp. 237–364.
Blehar, M.C. (2006). Women’s mental health research: The emergence of a biomedical field.
Annual Review of Clinical Psychology, 2, 135–160.
Bowlby, J. (1951). Maternal care and mental health. World Health Organization Monograph
(Serial No. 2).
Brach, T., (2003). Radical acceptance. New York: Bantam Books.
British Psychological Society (2005). Professional practice guidelines for counselling
psychologists. Retrieved 16th June 2010 from: http://www.bps.org.uk/publications/prof-
pract/prof-pract_home.cfm.
Brown, D., Rose, D., Lyons, E. (2009). Self-generated expressions of residual complaints
following brain injury. NeuroRehabilitation, 24, 175-183.
107

Chodorow, Nancy J. and Susan Contratto. 1989. "The Fantasy of the Perfect Mother." Feminism
and Psychoanalytic Theo y. Ed. Nancy J. Chodorow. New Haven: Yale University Press.
79-96.
Darvill, R., Skirton, H., Farrand, P. (2008). Psychological factors that impact on women’s
experiences of first-time motherhood: a qualitative study of the transition. Midwifery 26,
357–366.
Davis, D. and Walker, K. (2008) Re-discovering the maternal body in midwifery through an
exploration of theories of embodiment, Midwifery.
Dennerstein, L., Astbury, J., & Morse, C. (1993). Psychosocial and mental health aspects of
women’s health. Geneva: Division of Family Health, Division of Mental Health, World
Health Organization.
Deurzen E., van (1988). Paradox and Passion in Psychotherapy : An Existential Approach to
Therapy and Counselling. Wiley.
Deurzen, E., van (1997). Everyday Mysteries: Existential dimensions of psychotherapy. London:
Routledge.
Deurzen, E., van (2002). Existential Counseling & Psychotherapy in Practice (Second Edition).
London: SAGE Publications Inc.
Doss, B.D., Rhoades, G.K., Stanley, S.M., & Markman, H.J. (2009). The effect of the transition
to parenthood on relationship quality: An 8-year prospective study. Journal of Personality
and Social Psychology, 96(3), 601–619.
Doyal, L. (1995) What Makes Women Sick: Gender and the Political Economy of Health.
Macmillan, Houndmills.
Enteisled,. R. & Doerings,. G. (1981). The first birth: a family turning point. Baltimore: Johns
Hopkins University.
Gallagher, S. (2000a). Philosophical conceptions of the self: Implications for cognitive science.
Trends in Cognitive Sciences, 4(1), 14–21.
Gallagher, S. (2000b). Self-reference and schizophrenia: A cognitive model of immunity to error
108

through misidentification. In D. Zahavi (Ed.), Exploring the self: Philosophical and
psychopathological perspectives on self-experience (pp. 203–239). Amsterdam &
Philadelphia: John Benjamins.
Garcia, J., Kirkpatrick, R. and Richards, M. (1990) The Politics of Maternity Care. Oxford:
Clarendon Press.
Grace, Marty. 1998. "The Work of Caring for Young Children: Priceless or Worthless?" Women's
Studies International Forum 21(4): 401-413.
Hickey, G., & Kipping, C. (1996). Issues in research. A multi-stage approach to the coding of
data from open-ended questions. Nurse Researcher, 4, 81-91.
Holsti, O. R. (1969). Content Analysis for the Social Sciences and Humanities. Reading, MA:
Addison-Wesley.
Hsieh, H., Shannon, S.E. (2005). Three Approaches to Qualitative Content Analysis. Qualitative
Health Research, Vol. 15 No. 9, 1277-1288.
Hughes, A., Williams, M., Bardacke, N., Duncan, L. G., Dimidjian, S., Goodman, S.H. (2009).
Mindfulness approaches to childbirth and parenting. British Journal of Midwifery, 17(10)
630-635.
Kabat-Zinn J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face
stress, pain, and illness. New York, Dell Publishing
Koltko-Rivera, M.E. (2006). Rediscovering the Later Version of Maslow’s Hierarchy of Needs:
Self-Transcendence and Opportunities for Theory, Research, and Unification. Review of
General Psychology. Vol. 10, No. 4, 302–317.
Krippendorff, K. (1980). Content Analysis: An Introduction to Its Methodology. Newbury Park,
CA: Sage.
Lazaro, R. (1986). Feminism and Motherhood: O'Brien vs Beauvoir. Hypatia 1 (2): 87-102.
Lewis, S.E. (1995). A search for meaning: making sense of depression. Journal of Mental
Health, 4: 369–382.
109

Marcel, A. (2003). The sense of agency: Awareness and ownership of action. In J. Roessler &
N. Eilan (Eds.), Agency and awareness (pp. 48–93). Oxford: Oxford University Press.
Maslow, A. H. (1943). A theory of human motivation. Psychological Review, 50, 370–396.
Maslow, A. H. (1954). Motivation and personality. New York: Harper.
Maslow, A. H. (1969a). The farther reaches of human nature. Journal of Transpersonal
Psychology, 1(1), 1–9.
McLaughlin, E., (1993), ‘Women and the family in Northern Ireland’, Women’s Studies
International Forum, 16 (6): 553–568.
Miles, M.B. & Huberman, A. M. (1994). Qualitative data analysis: an expanded sourcebook.
London: Sage.
Mitchell, W., Green, E. (2002). ‘I don’t know what I’d do without our Mam’ motherhood, identity
and support networks. The Sociological Review, 50(1), 1-22.
Nelson, A.M., (2003). Transition to motherhood. Journal of Obstetric, Gynecologic and Neonatal
Nursing 32, 465–482.
Nicolson, P., (1998). Post-natal Depression: Psychology, Science and Transition to Motherhood.
Routledge, London .
Noblit, G., Hare, R., (1988). Meta-ethnography: Synthesizing Qualitative Studies. Sage,
Newbury Park.
Nomaguchi, K.M., & Milkie, M.A. (2003). Costs and rewards of children: The effects of becoming
a parent on adults’ lives. Journal of Marriage and the Family, 65(2), 356–374.
Oakley A. (1979) Becoming a Mother. Martin Robertson. Oxford.
Oakley A. (1980) Women Confined: Towards a Sociology of Childbirth. Martin Robertson.
Oxford.
O’Hara, M., & Swain, A. (1996). Rates and risk of postpartum depression – a meta-analysis.
International Review of Psychiatry, 8, 37–54.
110

Pancer, S.M., Pratt, M., Hunsberger, B., Gallant, M., (2000). Thinking ahead: complexity of
expectations and the transition to parenthood. Journal of Personality 68,253–278.
Parens, H.,1975. Parenthood as a developmental phase. Journal of the American
Psychoanalytic Association 23, 154–165.
Perry-Jenkins, M., Goldberg, A.E., Pierce, C.P., & Sayer, A.G. (2007). Shift work, role overload,
and the transition to parenthood. Journal of Marriage and Family, 69(1), 123–138.
Petch, J., & Halford, W.K. (2008). Psycho-education to enhance couples’ transition to
parenthood. Clinical Psychology Review, 28(7), 1125–1137.
Phoenix, A., (1991a), Young Mothers? Cambridge: Polity Press.
Phoenix, A. and Woollett, A., (1991), ‘Motherhood: social construction, politics and psychology’,
in Phoenix, A., Woollett, A. and Lloyd, E. (eds.) Motherhood, Meanings, Practices and
Ideologies, London: Sage: 13–27.
Pope, S. (2000). Postnatal depression: A systematic review of published scientific literature to
1999: An information paper. Canberra: National Health and Medical Research Council.
Prior, L. (2003). Using Documents in Social Research. Sage.
Raphael, Dana. 1976. The Tender G$: Breastfeeding. New York: Schocken Books.
Rejeski, W.J. (2008). Mindfulness: Reconnecting the Body and Mind in Geriatric Medicine and
Gerontology. Gerontologist; 48(2): 135–141.
Richardson, D. (1993). Women, Motherhood and Childrearing. London, Macmillan.
Robertson, E., Celasun, N., & Stewart, D.E. (2003). Risk factors for postpartum depression. In
D.E. Stewart, E. Robertson, C.-L. Dennis, S.L. Grace, & T. Wallington (Eds.), Postpartum
depression: Literature review of risk factors and interventions. Toronto: University Health
Network Women’s Health Program.
Rubin, R., (1961). Puerperal change. Nursing Outlook 9, 753–755.
Rubin, R., (1967). Attainment of the maternal role. Part1. Processes. Nursing Research 16,
111
237–245.
Rubin, R., (1984). Maternal Identity and the Maternal Experience. Springer,NewYork.
Scott, G. & Niven, C. (1996). Pregnancy: a bio-psycho-social event. In: C. "E.N. & A. Walker
(Eds), Conception, pregnancy and birth. Oxford: Butterworth-Heinmann.
Sethi, S.,(1995). The dialectic in becoming a mother: experiencing postpartum phenomenon.
Scandinavian Journal of Caring Sciences 9, 235–244.
Smith, J.A. (1999): Identity development during the transition to motherhood: An interpretative
phenomenological analysis, Journal of Reproductive and Infant Psychology, 17:3, 281-
299.
Sofaer, S. (1999). Qualitative Methods: What Are They and Why Use Them? HSR Health
Services Research 34(5)1101-1118.
Spier, D. (2001). Becoming a Mother. Journal of the Association for Research on Mothering,
3(1), 1-17.
Stern G. & Kruckman L. (1983) Multi disciplinary perspectives on postpartum depression: an
anthropological critique. Journal of Social Science an Medicine 17, 1027-1983.
Tsakiris, M., Schutz-Bosbach, S., Gallagher, S. (2007). On agency and body-ownership:
Phenomenological and neurocognitive reflections. Consciousness and Cognition, 16,
645–660.
Ussher J, .M. (1989). The psychology of the female body. London: Routledge.
Walsh, D.J. (2009). Childbirth embodiment: problematic aspects of current understandings.
Sociology of Health & Illness, 3 (3), 486–501.
Weaver,J., Usher,J., (1997).How motherhood changes life — a discourse analytic study with
mothers of young children. Journal of Reproductive and Infant Psychology 15, 51–68.
Weber, R. P. (1990). Basic Content Analysis. Newbury Park, CA: Sage.
White, M.D., Marsh, E. E. (2006). Content Analysis: A Flexible Methodology. In Library Trends
112

55 (1) 22–45.
Williamson, M. 2004. The Gift of Change: Spiritual Guidance for a Radically New Life. San
Francisco: Harper.
113

Appendix list
Appendix A
Poster
Appendix B
Information sheet
Appendix C
Consent Form
Appendix D
Ethics Flowchart
114
Appendix A – Poster
I am a doctoral student on the PsychD programme at Surrey University seeking participants for
my research project titled:
When women talk about motherhood: a content analysis of experiences
This research proposes to explore how individuals experience motherhood. Have you recently
become a mother and would you be willing to talk about your experience?
Participation in this research will involve meeting for an interview, at a time and place
convenient for you or electronic completion of questions if this is more convenient. Your
confidentiality will be maintained and all data will be handled in accordance with the Data
Protection Act (1988).
If you are interested in participating, or in learning more about the research,
please contact me at l.corbett@surrey.ac.uk
115
Appendix B – Participant Information Sheet
Participant Information Sheet
University of
Surrey
Guildford
GU2 7XH
Title of Research Project:
When women talk about motherhood: a content analysis of experiences
Brief description of the Research:
My name is Lisa Corbett and I am a third year student on the PsychD Counselling Psychology
doctoral programme at Surrey University.
Thank you for expressing an interest in participating in this research. If you do decide to
participate in this study the following information will inform you of what the process will involve.
This study is designed to explore the ways in which individuals experience becoming a mother
for the first time from an existential perspective.
It is hoped that the information which is gathered from interviewing participants will provide an
insight into how motherhood affects people existentially.
What will be expected from you as a research participant?
Participation in this research will involve either meeting with the researcher for a semi-structured
interview, at a time and place convenient for you, or completing some questions electronically.
The interview will normally last around 30 minutes and will be audio recorded. This recording
will be deleted once the interview has been analysed,
You have the right to withdraw from the study at any time without giving a reason up until the
point of data analysis. All data will be handled in accordance with the Data Protection Act
(1988).
Your confidentiality will be maintained provided the information you provide falls within the
British Psychological Society’s (BPS) and the Health Professions Council’s (HPC) ethical
guidelines.
The interview will be transcribed and your name and any other identifying information will be
116

removed. You will be given the opportunity to read the transcript and to alter any information
which you feel is inaccurate.
You will be required to sign consent forms before the interviews; you will be given copies of
these.
What will be covered in the interview:
• You will be invited to give a general account of your experience of motherhood.
• You will be invited to contribute any other information which you think is relevant to this
research.
If you need any further clarification or have additional questions, please do not hesitate to
contact me.
Yours sincerely,
Lisa Corbett (Trainee Counselling Psychologist, University of Surrey)
Researcher contact details:
Lisa Corbett
Trainee Counselling Psychologist
University of Surrey
Guildford
GU2 7XH
Email: l.corbett@surrey.ac.uk
If you are unhappy with any aspect of how you have been treated in the research, please
contact my supervisor:
Dr Dora Brown
University of Surrey
Guildford
GU2 7XH
Email: d.brown@surrey.ac.uk
117
Appendix C – Consent Form
The Existential Experience of Motherhood
Consent Form
• I the undersigned voluntarily agree to take part in the study on the Existential
Experience of Motherhood
• I have read and understood the Information Sheet provided. I have been given a full
explanation by the investigators of the nature, purpose, location and likely duration of
the study, and of what I will be expected to do. I have been given the opportunity to
ask questions on all aspects of the study and have understood the advice and
information given as a result.
• I agree to comply with any instruction given to me during the study and to co-operate
fully with the investigators. I shall inform them immediately if I suffer any deterioration
of any kind in my health or well-being.
• I consent to my personal data, as outlined in the accompanying information sheet, being
used for this study and other research. I understand that all personal data relating to
volunteers is held and processed in the strictest confidence, and in accordance with the
Data Protection Act (1998).
• I understand that I am free to withdraw from the study at any time up until the point of
data analysis without needing to justify my decision and without prejudice.
• I confirm that I have read and understood the above and freely consent to participating
in this study. I have been given adequate time to consider my participation and agree to
comply with the instructions and restrictions of the study.
Name of volunteer (BLOCK CAPITALS)
........................................................
Signed
118
........................................................

Date
......................................
Name of researcher/person taking consent (BLOCK CAPITALS) ........................................
Signed
......................................
Date
......................................
Researcher contact details:
Lisa Corbett
Trainee Counselling Psychologist
University of Surrey
Guildford
GU2 7XH
Email: l.corbett@surrey.ac.uk
119
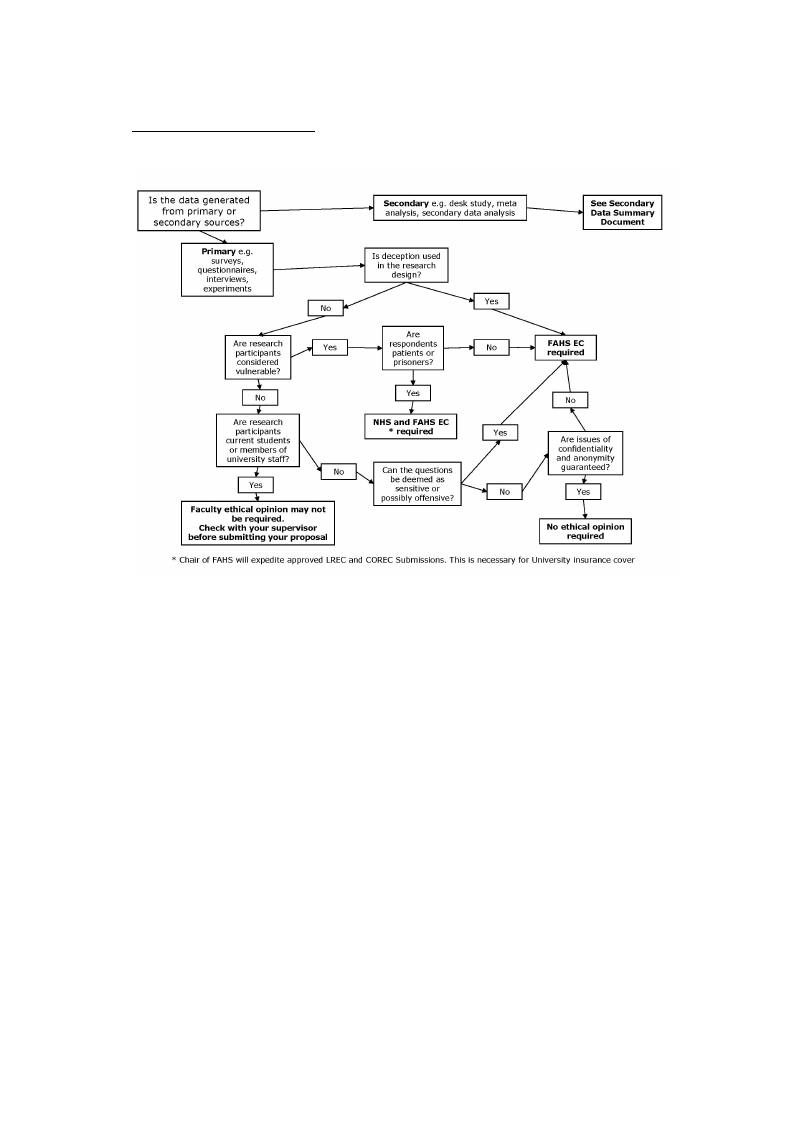
Appendix D - Ethics Flowchart
120