
International Journal of
Environmental Research
and Public Health
Article
The Effects of a Health Promotion Program Using
Urban Forests and Nursing Student Mentors on the
Perceived and Psychological Health of Elementary
School Children in Vulnerable Populations
Kyung-Sook Bang 1 , Sungjae Kim 1, Min Kyung Song 2,* , Kyung Im Kang 2 and
Yeaseul Jeong 2
1 Faculty of College of Nursing, The Research Institute of Nursing Science, Seoul National University,
Seoul 03080, Korea; ksbang@snu.ac.kr (K.-S.B.); sungjae@snu.ac.kr (S.K.)
2 College of Nursing, Seoul National University, Seoul 03080, Korea; fattokki@snu.ac.kr (K.I.K.);
Jeongfm1@snu.ac.kr (Y.J.)
* Correspondence: mk0408@snu.ac.kr; Tel.: +82-2-740-8467
Received: 3 July 2018; Accepted: 9 September 2018; Published: 11 September 2018
Abstract: As problems relating to children’s health increase, forest therapy has been proposed
as an alternative. This study examined the effects of a combined health promotion program,
using urban forests and nursing student mentors, on the perceived and psychosocial health of
upper-grade elementary students. The quasi-experimental study ran from June to August 2017,
with 52 upper-grade elementary students from five community after-school centers. With a purposive
sampling, they were assigned to either an experimental group (n = 24), who received a 10-session
health promotion program, or to a control group (n = 28). Seven undergraduate nursing students
participated as mentors. Running over 10 weeks, each weekly session consisted of 30 min of
health education and 60 min of urban forest activities. Data were analyzed by independent t-test,
Mann-Whitney U-test, paired t-test, or Wilcoxon signed rank test. General characteristics and
outcome variables of both groups were homogeneous. The experimental group showed significant
improvement in self-esteem (p = 0.030) and a significant decrease in depressive symptoms (p = 0.020)
after the intervention, compared to the control group. These results suggest that forest healing
programs may contribute to the spread of health promotion programs that make use of nature.
Keywords: forests; mentors; health promotion; school-aged children
1. Introduction
In Korea, even school-aged children experience a high level of stress, anxiety, depression,
and mental health problems [1]. In addition, the lack of physical activity due to sedentary lifestyles
causes physical health problems such as an increase in obesity and decrease of physical strength [2].
Meanwhile, school violence has been increasing annually, and one possible cause of this problem is
the lack of social interaction and emotional connection in modern society, caused by the increase in
individualistic activities and computer use, and the decrease of contact and interaction with nature [3].
Kaplan and Kaplan [4] emphasized that the natural environment may be the best place to regain
our attention and focus, and these benefits have also been shown to occur in children. Nature helps
children to improve their psychological functioning [5], to cope with their problems, to think clearly,
and to feel free and relaxed [6].
Recently, there has been considerable and increasing global attention towards using the forest
environment as a place for recreation and health promotion. It has been noted that activities in the
Int. J. Environ. Res. Public Health 2018, 15, 1977; doi:10.3390/ijerph15091977
www.mdpi.com/journal/ijerph

Int. J. Environ. Res. Public Health 2018, 15, 1977
2 of 11
forest contribute to promoting physical and emotional well-being [7]. Forest healing refers to actions
that enhance the health of the human body by utilizing various elements of the forest such as the
landscape, phytoncide, water, wind, scent, and sound [8].
Countries such as the United Kingdom, Denmark, Sweden, and Finland are highly interested
in situating children’s education in nature. Learning outside the classroom takes place in a variety
of forms, including Forest School programs, outdoor sports, activities on school grounds, and visits
to beaches and parks in the local community. The purpose and benefits of these experiences are
also varied. Some focus on raising self-esteem and confidence; some on social skills, communication,
and teamwork; and others on physical development and health [9,10]. Based on a systematic review,
McCormick [11] reported that access to green space was associated with improved mental well-being,
overall health, and cognitive development in children. Although some previous studies have reported
positive effects of forest therapy on children’s mental health [12,13], nature-based intervention or
education in Korea is still very limited.
In another aspect, a global trend shows differences in health status according to socioeconomic
level, and various policies are being tried to reduce the gap. In Korea, one of the child welfare policies
provides after-school care-giving at public “community centers for children” for low-income families
with elementary- or middle-school students. However, the main services provided to children in
these centers focus on educational or nutritional support, which does not provide integrated care
in terms of the child’s physical, mental, and social aspects. In particular, there are no professional
health-related services.
Therefore, in this study, we developed an integrated health promotion program including outdoor
activities in a forest or urban park for the children attending community centers. The program was also
expected to promote perceived health status and self-esteem, to reduce the symptoms of depression,
to improve concentration through exposure to various resources of nature, and to enhance sociality
through the use of group activities.
In addition, a special component of this study was that nursing students participated as mentors.
When considering the developmental characteristics of school-aged children, it is possible to promote
more active participation through forming relationships with college student mentors, who are more
likely to encourage friendship and admiration. For the nursing students, participating in health
promotion programs for children in vulnerable populations will be an opportunity to enhance their
understanding of children’s developmental characteristics, and to form therapeutic relationships.
Purpose of Study and Hypotheses
The purpose of this study was to develop a combined health promotion program using urban
forests and nursing student mentors for vulnerable school-aged children and to evaluate the effects of
this program on the perceived and psychological health of elementary school students in vulnerable
populations. Specific hypotheses in this study were as follows:
1. The improvement in the perceived health status of children between pre- and post-program
will be greater in the experimental group than in the control group.
2. Gains in self-esteem, peer relationships, and of sympathetic to parasympathetic autonomic
balance and reductions in depression, attention deficit, and hyperactivity (ADHD) between pre- and
post-program will be greater in the experimental group than in the control group.
2. Materials and Methods
2.1. Study Design and Participants
This quasi-experimental study, based on a control group pre-test–post-test design, was planned to
develop a 10-session health promotion program using urban forests and nursing student mentors and
to investigate its effects on elementary-school students in grades 4 to 6 at five community centers for
children in Seoul. These community centers for children are public social welfare facilities that provide
Int. J. Environ. Res. Public Health 2018, 15, 1977
3 of 11
cInatr.eJ.sEenrvviriocne.sRfeos.rPvubulilcnHeeraaltbhle20c1h8,i1ld5,rxen. The children who use these centers are mostly from low-inc3oomf 1e1
families. Community child centers for children perform various important roles in community welfare,
iinncclluuddiinngg ooffffeerriinngg pprrootteeccttiioonn aanndd aafftteerr--sscchhooooll eedduuccaattiioonn pprrooggrraammss,, pprroovviiddiinngg hheeaalltthhyy rreeccrreeaattiioonnaall aanndd
ffrreeee--ttime programs, and linking chhiillddrreenn’’ssppaarreennttsswwiitthhtthheeccoommmmuunnitiyty[1[144].].
TThhee ssttuuddyy wwaass aapppprroovveedd bbyy tthhee EEtthhiiccss CCoommmmiitttteeee ooff tthhee IInnssttiittuuttiioonnaall RReevviieeww BBooaarrdd aatt SSeeoouull
NNaattiioonnal UUnniivveerrssiittyy ((IIRRBB NNoo.. 11770077//000033--000011)).. BBeefoforerebbeeggininnniningg tthhee ssttuuddyy, participants and tthheeiirr
ppaarreennttsswweerreepprroovviiddeeddwwiitthhaa thoroouugghh descripttiioonn of the study’s objectives, experimental procedure,
aanndd measuremenntt ttoooollss..OfOtfhethcehiclhdirlednreanndanpdarpenatrsenwtshowdheocidecdidtoedpatroticpiaprattieciipnatehisinsttuhdisy,sthuodsye,
twhohsoe swuhbomsiuttbedmithteedirthweriirttwenritcteonnsceonntsewnetrwe eirnecilnucdleuddeidn itnhtehestsutduyd.y.CChhilidldrerennwwhhoo had mmeeddiiccaall
ccoonnttrraaiinnddiiccaattiioonnsstotoexeexrecricsiesebybyselsfe-rlfe-preoprto(ret.g(e.,.ga.s,thamstha,mpaa,inpfauilnofustleosatrethorairttihs)riwties)reweexrceluedxecdlu. dAetdo.taAl
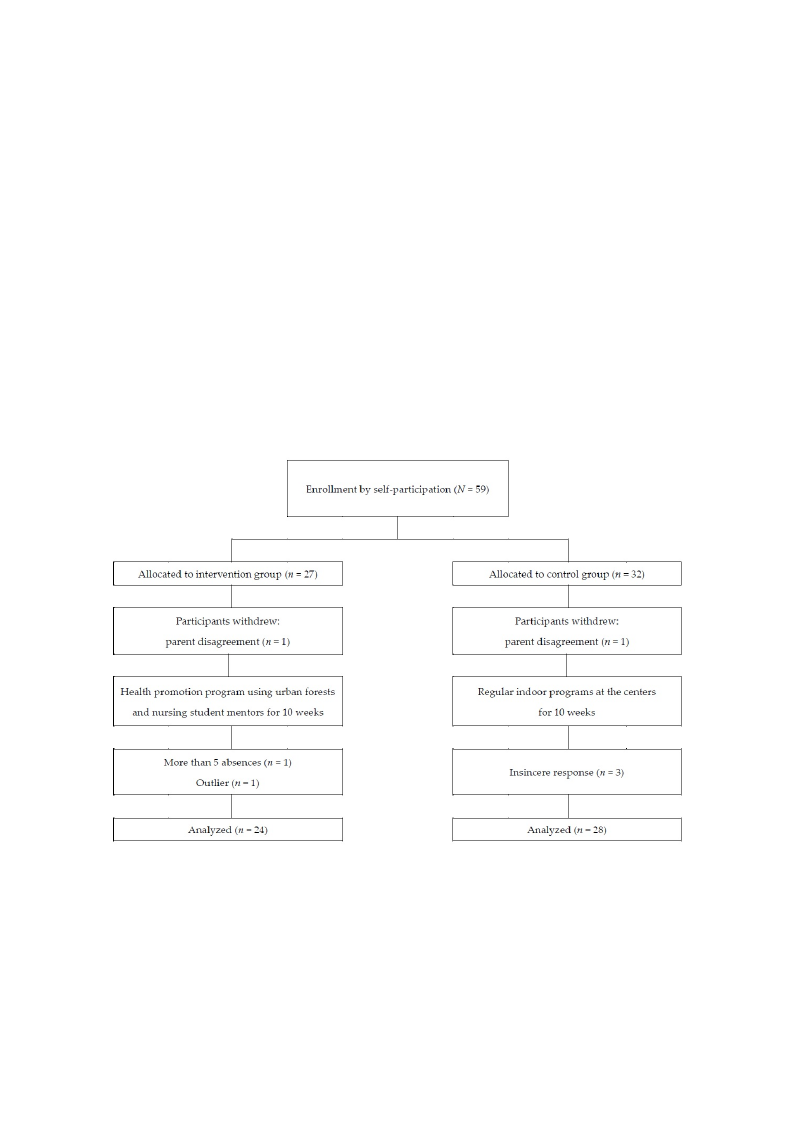
otof t5a9l sotfud59ensttsuidnegnrtasdiensg4rtaod6esat4fitvoe6coamt fmivuencitoymcmenutenristypacertnicteiprsatpeadritnicitphaistesdtuidny.thWisitshtuadpyu.rWpoistihvea
spaumrppolisnivge, tshaemypwlinerge, tahsesyigwnedretaosesigthneerdatno exitpheriamneenxtpalergirmouenptathl gatrowuapstphraotvwidasedprwovitihdead1w0-istehsasi1o0n-
hsesaslitohnphroeamltohtipornomprootgiornamprwogitrhamnuwrsitihngnustrusidnegnsttmudeennttomrse(nnto=r2s7(n) o=r2a7)corntarocol ngtrrooul pgr(onu=p3(n2)=. O32f).thOef
5th9ech5i9ldcrheinldirnengriandgesra4dteos64attot6heatcothmemcoumnimtyucneinttyercsenfoterrcshfioldrrcehni,ld57reang,r5e7edagtorepeadrtiocippaartteiciniptahte sintutdhye.
Tsthueddya. tTahoefd5a2tachoifld5r2ecnhwilderenfiwnaelrley fainallyyzeadn,alwyzitehdt,hweitehxctehpeteioxnceopftionnsinofceinresirnecseproenrseesspothnasteswtehraet
iwdeenretifiidedenbtyifibeedinbgymbaeriknegdmwaitrhkethdewsaimthetnhuemsbamerse onnuamllbieterms os nofatlhleitqeumestioofnnthaeirequeveestniothnonuagirhe tehveeren
wtheoruegrhevtehresree qwueersetiroenvser(sne=qu3e),sptiaorntsic(inpa=t3io),npianrtfiecwipeartitohnainnfifevwe eserstshiaonnsfiv(ne =se1s)s,ioannsd(nth=o1se), tahnadt twheorsee
othuatltiewrseraenoduptlrieesresnatned pasreasnenetxetdreamseavnaelxutereomn ethveadluaetaodnitshtreibduattiaondi(sntr=ib1u;tFioignu(rne=1)1.; Figure 1).
FFiigguurree 11.. RReeccrruuiittmmeenntt ooff ppaarrttiicciippaannttss..
22..22.. IInntteerrvveennttiioonn
tocoloc3heonno0necmmmtpaluamehmAiArcsnyseutyuysucscnfsinosoroctoitiemtreametnymyltambhbacpnaieaeincndhntntedlieyieenc6tcdsdecp0tirrtercsh.huemreyaeTv.ervlciaeaihnihTaeleleatontwhwfhhnso1deodp0rp[[cp-1r1t16rsihos5o0a05eyme]-lm]smscshfaeoahiooeniostnontraisndiedosloifstoonhonhtancarepaipaanatcnrnhhrlletotoeideehehgvegadferidfprlotoaastaisrhrmrelmoeteasahmssspsuittusnasrosaeeseontisctxisnimhdnstopsigmegmnveofouirutuepetiirrrnieronreebbbnotntssaaacgt[nin[ne1rnpe1a6ffax6rftmoo]oocph]rrtrgweeeeiweuvrrssusaasititatetirsssmssninb,eagadwacsdnnenu.euehddsEsasfriiioicbancgnnghtrcaunguinehnvrwersesidssutfdtieseioinrnr,esrfbegfwsgsoeoa.is1rsorhnstE0ttsnicuucacmhfchdachdooihlieilrellwnndnoednssrstcearetietasermwsmsntetnseeaeie1cddoaynano0nttto3nttfmtoeor0feasronrnillismsmselnddotcbbieiacitnnaenaduawsagsgtrfeceeaoeodhaddysraf
cforommmeuancihtyccoemnmterunfoitrychceilndtreernf.oTrhcehsiltdurdeyn.dTevheelostpueddyadwevrietltoenpepdroagwrarmittmenanpuroagl rfoamr thmeainnutearlvfeonrtitohne
pinrotevrivdeenrstitoonenpsruorveitdheersadthoereennscue rteo tthheeinatedrhveernetniocne ptroottohceol ianntdercvoennstiisotenncpyrothtorocuolghaonudt thcoenpsriosgternamcy
throughout the program implementation. The program was provided once a week for 10 weeks, from
June to August 2017. The control groups attended only the routine programs (e.g., supplementary
learning such as math or English, reading, art) at their community center for children.
Int. J. Environ. Res. Public Health 2018, 15, 1977
4 of 11
implementation. The program was provided once a week for 10 weeks, from June to August 2017.
The control groups attended only the routine programs (e.g., supplementary learning such as math or
English, reading, art) at their community center for children.
The program was conducted by the research team, all of whom were registered nurses whose
majors were either child health or psychiatric nursing. One of them was a certified forest therapist,
and one had completed the approved training course for forest therapy. During the sessions, two forest
day camps were included; those were run by an external forest therapist. A total of seven nursing
student mentors were involved in activities to facilitate the program and to promote the participation of
children. The orientation was conducted before the start of the health promotion program to minimize
any differences between the mentors. The major content of the orientation included an introduction of
forest therapy, the specific contents and activities of the program, and the roles of mentors. Each mentor
was responsible for three to four children, and two research team members supervised the mentors. In
addition, the mentors shared significant matters that occurred during the program through the closed
social network service (Kakao group talk), and their activities, feelings, and opinions were submitted
anonymously through the Google questionnaire. The feedback from the forest therapist of the research
team was provided and shared with all mentors. A social worker working at the community center for
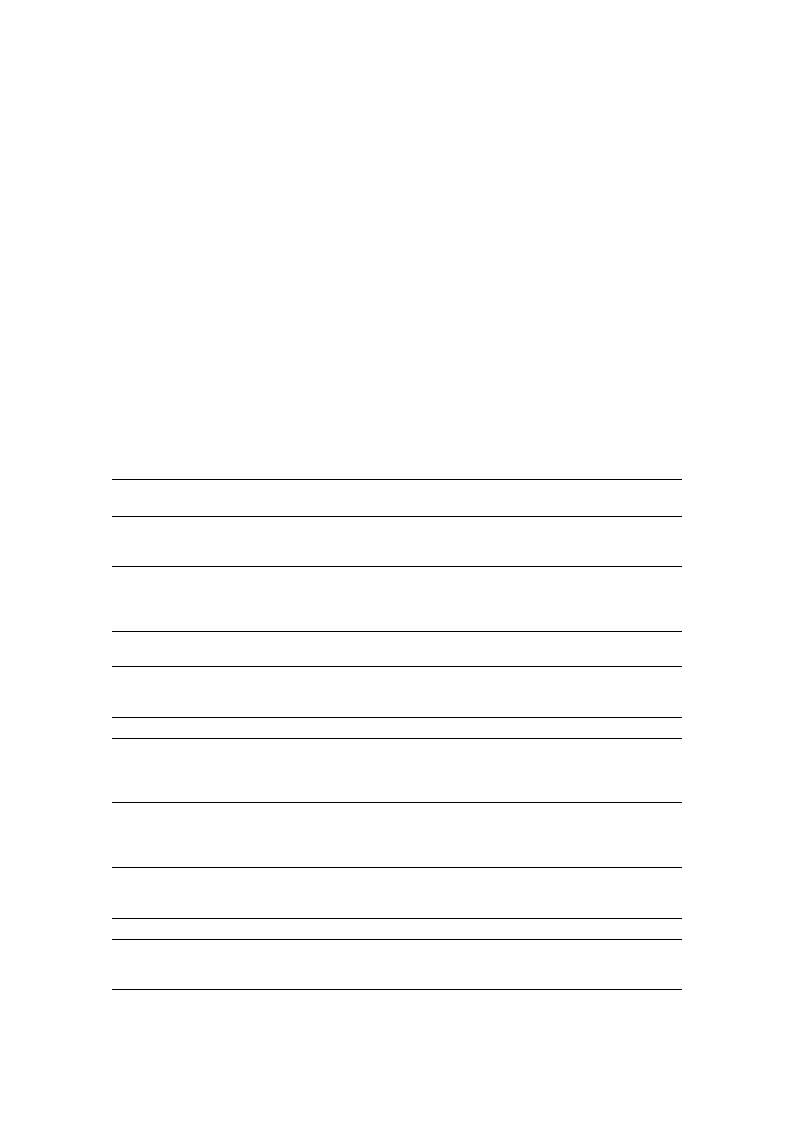
children accompanied the activities as an assistant for child safety. Table 1 shows the topics, contents,
and time duration of each session.
Table 1. The topics of program sessions.
Session
1
2
3
4
5
6
7
8
9
10
Lecture
Forest Therapy
Program orientation
Meeting with mentors
Pre-test
Understanding the
relationship between physical
and psychosocial health
Making a nickname for natural
objects that resemble me
Five senses experience in
urban forest
Personal hygiene and
eating habits
Physical activities in forest (I)
-Forest walking and exercise
Internet overdependence
Playing with natural materials (I)
-Making a paper fan with dry
flowers and leaves
Forest day camp (I)
Self-emotion awareness and
expression
Playing with natural materials (II)
-Rock-paper-scissors game with
natural materials
-Water carrying using leaves
Self-esteem
Self-expression activities with
natural materials
Making a bracelet of
retinispora beads
Communication and peer
relationships
Physical activities in forest (II)
-Cloth volleyball
-Traditional play
Forest day camp (II)
Completion ceremony
Discussion with mentors
Post-test
Program Duration
(hours)
2
2
2
2
4
2
2
2
4
2

Int. J. Environ. Res. Public Health 2018, 15, 1977
5 of 11
2.3. Measurements
Participants’ height and weight were measured using an automatic stadiometer (BSM 370,
Inbody Co., Ltd., Seoul, Korea). Heart rate variability (HRV) was also measured using a portable
electrocardiograph (LXC3203, LAXTHA Inc., Daejoen, Korea). To minimize changes in autonomic
nerves, HRV was performed after stabilization for at least 5 min, taking 5 min to complete the
measurement. In this study, the HRV parameters were measured by a frequency domain analysis.
The ratio of low frequency to high frequency (LF/HF ratio) in HRV was used to represent a measure of
sympathetic to parasympathetic autonomic balance of the participants [17].
A pilot test using a self-report questionnaire was administered to elementary school students in
grades 4–6 who did not participate in this research. As a result, it was confirmed that the students in
upper grades did not have any difficulty in completing the questionnaire, which took about 20 min to
complete at each time point. The specific instruments provided on the questionnaire were as follows.
Perceived health status. Perceived health status of participants was assessed by a single-sentence
question: “How do you feel about your overall health condition?” It was rated as “very good (5 points),”
“good (4 points),” “moderate (3 points),” “bad (2 points),” or “very bad (1 point).”
Self-esteem. Self-esteem was measured using the Rosenberg Self-Esteem Scale (RSE) [18] which
includes 10 statements. Each statement is rated on a 4-point Likert scale with 4 = “strongly agree,”
3 = “agree,” 2 = “disagree,” and 1 = “strongly disagree.” The negative items were scored in reverse
order. All items were added together with scores ranging between 10 and 40; a higher score means a
higher level of self-esteem. At the time of tool development, the Cronbach’s alpha was reported as
0.88; the Cronbach’s alpha in this study was 0.85.
Depression. The Korean version of the Children’s Depression Inventory (CDI) [19] was selected for
assessment of the participants’ depressive symptoms. There are 27 items quantifying depressive symptoms
such as depressed mood, hedonic capacity, vegetative functions, self-evaluation, and interpersonal
behaviors. Each item has a 3-point Likert scale as 0 = “absence of symptoms,” 1 = “mild or probable
symptom,” and 2 = “definite symptom,” and a higher CDI score means a higher level of depressive
symptoms. Han and Yoo [19] reported the Cronbach’s alpha as 0.81 for CDI in elementary and middle
school students; the Cronbach’s alpha in the present study was 0.87.
Peer relationships. The peer relationship instrument [20] consisted of 20 questions for
measuring the presence and reliability of friends, persistence of and adaptation to peer relationships,
and communal life with friends. This instrument uses a 5-point Likert scale 1 = “not at all” to 5 = “very
much,” and the higher the total score, the higher the level of the peer relationships. Kim [20] reported
the Cronbach’s alpha as 0.94 for peer relationships for elementary school students, and the Cronbach’s
alpha in the present study was 0.90.
Attention deficit and hyperactivity. The Korean version of Conners-Wells Adolescents Self-Report
Scales (CASS-S, short form) [21] was used to assess the level of attention deficit and hyperactivity of the
participants. This instrument includes 27 statements that evaluate behavior and cognitive problems,
the level of hyperactivity, and ADHD indicators of respondents using a 4-point Likert scale from
1 = “not at all” to 4 = “it really is.” Higher scores indicate greater hyperactivity. As a result of the
reliability test of CASS (S), the Cronbach’s alpha was 0.77; the Cronbach’s alpha in this study was 0.88.
2.4. Statistics
After normality tests using Kolmogorov-Smirnov test and Shapiro-Wilk test, an independent
t-test or Mann-Whitney U-test was used to determine any differences in pre-test data between the
experimental and control groups. Post-test data analyses were conducted using an independent t-test
or Mann-Whitney U-test for comparison between groups, and a paired t-test or Wilcoxon signed rank
test was employed for intragroup comparisons. The effect size was calculated using the effect size d
for the parametric data and the effect size r for the non-parametric data [22]. Interpretations of d and r
are as follows: d = 0.2 (small effect size), d = 0.5 (moderate effect size), d = 0.8 (large effect size), r = 0.1
Int. J. Environ. Res. Public Health 2018, 15, 1977
6 of 11
(small effect size), r = 0.3 (moderate effect size), r = 0.5 (large effect size) [23,24]. SPSS for Windows
Version 22.0 was used for all data analyses, and the statistical significance was set at p = 0.05.
3. Results
There was no significant difference between the experimental and control groups in the
homogeneity test of general characteristics and outcome variables. The demographic characteristics
and outcome variables of the groups are shown in Table 2.
Table 2. Homogeneity test of participants’ demographic characteristics and outcome variables during
the pre-test (N = 52).
Exp. (n = 24) Cont. (n = 28)
Characteristics/Variables Categories
n (%)
n (%)
χ2/t/Z
p
M ± SD
M ± SD
Age (years)
11.83 ± 0.82
11.75 ± 0.97
0.33
0.741 †
Gender
Male
Female
8 (33.3)
16 (66.7)
14 (50.0)
14 (50.0)
1.47
0.225 ‡
Grade
4th
10 (41.7)
11 (39.3)
5th
8 (33.3)
9 (32.1)
0.09
0.958 ‡
6th
6 (25.0)
8 (28.6)
Perceived health status
Self-esteem
Depression
Peer relationships
Attention deficit and hyperactivity
LF/HF ratio
4.04 ± 0.95
31.42 ± 5.48
12.26 ± 7.99
79.27 ± 12.34
15.09 ± 9.26
1.02 ± 0.58
3.68 ± 1.12
31.86 ± 5.06
9.39 ± 7.27
78.54 ± 13.77
14.85 ± 11.57
1.67 ± 1.38
−1.31
−0.04
−1.33
0.20
−0.66
−1.83
0.191 §
0.971 §
0.184 §
0.845 †
0.507 §
0.068 §
Exp.: experimental group; Cont.: control group; LF: low frequency; HF: high frequency; M: mean; SD: standard
deviation; † t-test; ‡ χ2 test; § Mann-Whitney U-test.
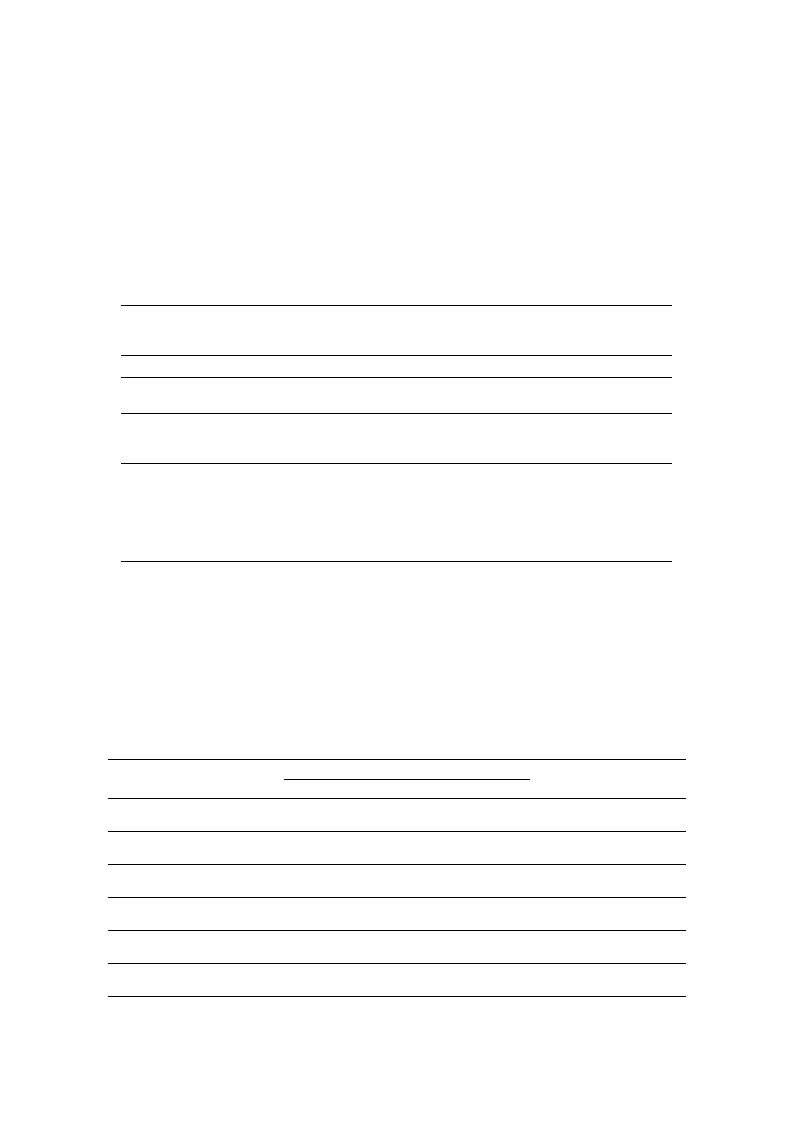
Table 3 shows the comparison of pre- and post-test mean scores for the experimental and control
groups. In the experimental group, self-esteem was significantly increased (p = 0.030, d = 0.47),
and depression was significantly decreased (p = 0.020, r = −0.48) after the intervention. No statistically
significant changes were found in the control group. This means that this program was partly effective
in improving children’s psychological health.
Table 3. Comparisons of changes in outcome variables between the experimental and control groups
(N = 52).
Variables
Group
Pre-Test
Post-Test
M ± SD
Difference
t or Z
p
ES
d/r
Perceived health
status
Exp.
Cont.
4.04 ± 0.95
3.48 ± 1.12
4.21 ± 0.83
3.86 ± 0.97
0.17 ± 0.96
0.18 ± 1.22
0.76
0.449 ‡ 0.15
0.62
0.538 ‡ 0.12
Self-esteem
Exp.
Cont.
31.42 ± 5.48
31.86 ± 5.06
33.21 ± 4.35
30.43 ± 5.03
1.79 ± 3.79
−1.43 ± 4.73
2.32
−1.12
0.030 †
0.265 ‡
0.47
−0.21
Depression
Exp.
Cont.
12.26 ± 7.99
9.39 ± 7.27
9.67 ± 6.44
8.57 ± 6.86
−2.74 ± 5.55
−0.82 ± 4.44
−2.32
−0.63
0.020 ‡
0.531 ‡
−0.48
−0.12
Peer relationships
Exp.
Cont.
79.27 ± 12.34 78.96 ± 11.11 −0.43 ± 12.34
78.54 ± 13.77 80.36 ± 13.40 1.82 ± 9.10
−0.16
1.19
0.875 †
0.236 ‡
−0.03
0.22
Attention deficit
and hyperactivity
Exp.
Cont.
15.09 ± 9.26 15.58 ± 11.99
14.85 ± 11.57 14.14 ± 9.77
0.22 ± 7.50
−0.48 ± 9.85
0.14
−0.25
0.891 †
0.802 †
0.03
−0.05
LF/HF ratio
Exp.
Cont.
1.02 ± 0.58
1.67 ± 1.38
1.05 ± 0.61
1.45 ± 0.95
0.03 ± 0.71
−0.22 ± 0.98
0.19
−1.20
0.849 †
0.241 †
0.04
−0.23
Exp.: experimental group; Cont.: control group; LF: low frequency; HF: high frequency; M: mean; SD: standard
deviation; ES: effect size; † paired t-test; ‡ Wilcoxon signed rank test.

Int. J. Environ. Res. Public Health 2018, 15, 1977
7 of 11
4. Discussion
The aim of this study was to investigate the effects of a combined health promotion program
using urban forests and nursing student mentors on the perceived and psychological health of
elementary-school students. Previous studies have performed forest activities or green activities [25–30]
or mentoring programs [31–34], but we expected positive reinforcement by not only using forest
activities but also mentors in this study. As a result, self-esteem and depression were significantly
improved in the experimental group, who participated in the health promotion program.
Previous forest activity studies conducted with children and adolescents reported that forest
activities had positive effects on mental and physical health, including conditions such as ADHD,
anxiety, depression, high blood pressure, and the lack of physical activity [11,35,36]. Also, a previous
systematic review has reported that urban green space can increase physical activity levels, and access
to urban green space also reduces stress and improves mood and the quality of life for people of all
ages [37].
It has also been reported that green exercise has a positive effect on self-esteem and social
interaction for adults [26]. Further studies that have examined the effectiveness of forest activity
programs for children in community centers for children in Korea also reported improved children’s
self-esteem [12,27]. In this study, after participating in the program, the self-esteem of the experimental
group increased by 1.79 ± 3.79, whereas that of the control group decreased by 1.43 ± 4.73, indicating
that the program improved self-esteem. However, some studies have reported that playing in nature
has no significant effect on children’s self-esteem [25,30,38]. These researchers argue that children
and adolescents may not receive the benefits of nature-friendly interventions because they do not
experience the same level of connection with the natural environment as adults. Studies on the effects
of forest camps and forest schools on improving psychological health outcomes, including self-esteem,
have commented on the necessity of the direct use of the natural environment and suggested activities
that use natural environments such as camping and horticulture [39]. In his book Last Child in the
Wood, Louv [40], who had earlier attracted the attention of the world by emphasizing the need for
contemporary children to be in contact with nature, has accumulated the positive effects of nature on
children’s relaxation, self-worth, and self-esteem. He especially emphasized the importance of nature
itself and did not focus on the structured program, but instead focused on giving them a chance to
connect with and have free play in nature. Also, it was revealed that children who participated in
camp demonstrated improved initiative and self-direction that transferred to their lives at home and
in school. Therefore, children may need more time for direct interaction with or exploration in nature,
as well as further structured interventions beyond simply playing in the forest, to have a more positive
effect on self-esteem. In this study, the positive effect on self-esteem may be attributed to the direct
interaction with nature activities and nursing student mentors in the intervention.
Also, by spending more time in and feeling the benefits of nature in a calm and natural
environment, children’s nervous systems can relax from the resulting increase in parasympathetic
nerve activation. While not found in this study, several previous studies with adults reported that
forest activity leads to an activated parasympathetic nervous system, enhanced HF components of
HRV, and lower LF/HF as a positive relaxation effect of forest therapy [41–43]. In previous studies
that provided forest-based interventions, assessments of the effect were made immediately after the
intervention. But in the present study, a post-test was performed one week after the last program was
provided, which may have increased confounding factors. Therefore, further research is needed to
consider the timing of measurement.
The differences in depressive symptoms within the group decreased in the experimental group
(2.74 ± 5.55) and the control group (0.82 ± 4.44) in this study, but only that of the experimental group
was statistically significant. In a systematic review of the effects of forest therapy on depression,
forest therapy has been reported to be a new and effective intervention in reducing depression in
elementary-school students as well as adults [15,44]. According to the meta-analysis, which evaluated
the effectiveness of the forest-related programs, forest-related programs showed the greatest effect
Int. J. Environ. Res. Public Health 2018, 15, 1977
8 of 11
on depression (ES = 1.358) among psychological outcome variables, and self-esteem (ES = 1.269) and
sociality (ES = 1.281) showed high effect sizes [45].
In this study, mentors seemed to function as an effective intervention tool, in addition to the forest
activities. There was a positive effect of self-understanding, confidence, and achievement through the
participants’ relationships with the mentors, which might reinforce the participants’ internal factor.
This result shows a similarity to the results of previous studies that explored the effect of mentoring
programs [31,34], in which the relationship between mentors positively affected the psychological
health of vulnerable youths. According to the qualitative study of Akrimi, et al. [46], which explored
the experience of school-aged children participating in a charity mentoring program with volunteer
university-student mentors, the unconditional and supportive relationship between the children and
mentors were commonly experienced. The developments of social-emotional, cognitive, and identity
of the youth are accomplished based on their emotional connectedness with mentors and result in
positive outcomes for the youth [33].
Previously, Kim [32] explored the competence of mentors using the Delphi analytic approach.
Interpersonal skills, observation ability, and communication ability are necessary competencies for the
mentors. With these skills, mentors can consider and respect themselves and others, sense mentees’
changes, and make accurate communication. These skills are emphasized in the field of nursing. For
example, the Nursing and Midwifery Council [47] suggested communication and interpersonal skills
as one of the standards for competence of registered nurses; therefore, educational nursing institutions
should focus on educating their students to foster these abilities through the program. Thus, through
the nursing students’ participation as mentors, they spontaneously formed supportive relationships
with youth and educed children’s psychological and emotional development. An online survey and
interviews were conducted for a qualitative study about the experiences of seven nursing students
participating in this health promotion program. The qualitative study of the nursing students was
undertaken at the same time as the evaluation of the children, but that the results have been reported
separately [48]. As a result of qualitative research, this program was helpful for nursing students, as it
provided opportunities for them to interact with and understand children.
Meanwhile, the peer relationship questionnaire item, used as an indicator of sociality, includes
questions about the presence of friends, reliability, and continuity of friendship; it showed no significant
difference between the groups. The questions about peer relationships mainly focus on the relationships
with school friends, and thus the improvement of relationships with other children at the community
center may not be reflected.
This study has some limitations. First, it was not possible to confirm whether the effect
of the intervention was due to the mentoring or the urban forest activities because the health
promotion program in this study utilized both urban forest activities and mentoring. Therefore, future
studies will be required using a design to identify the individual effects of the forest activities and
mentoring, and advanced analyses, such as mediation analyses. Such analyses will provide a clearer
understanding of each component on the intervention. Second, it was a quasi-experimental study in
which randomization was not used in place of intervention or assignment of the study participants.
Community centers for the children participating in the study were selected based on accessibility
and preference, which could lead to an imbalance or bias between study conditions and may have
influenced subsequent analyses. Third, though both groups did not significantly differ at the baseline
(as a result of lack of power), there seems to be a substantial difference in gender distribution among
intervention and control condition. Particularly since girls might be more “vulnerable” to psychosocial
health outcomes than boys [49,50], the influence of gender on the effectiveness of intervention cannot
be ruled out. Fourth, consideration should be given to more diverse outcome variables such as
emotions, which have been the most studied responses to green exercise [51]. As the health promotion
program consisted of 60 min of activity after 30 min of lecture, there was not enough time allocated to
being active in the forest, except for the time to move to the urban forest. It is also possible that the
participants felt less interested in the program because they felt that the indoor lectures formed part of

Int. J. Environ. Res. Public Health 2018, 15, 1977
9 of 11
the classroom. Future research with a structured outdoor activity-focused program is recommended,
and consideration should be given to encouraging the interest of the research participants. Also,
more appropriate outcome measures might be required to identify the benefits of the program across
multiple outcomes.
Despite these limitations, this program has visible strengths incorporating the feasibility of forest
therapy as a health promotion program, which makes use of readily accessible urban forest parks,
and the participation of nursing students as mentors, which might strengthen the psychological
support for the participating children.
5. Conclusions
Our study showed that a combined health promotion program using urban forests and nursing
student mentors significantly improved self-esteem and depression of elementary-school students in
community centers for children. It is important that the forest healing program, which is growing in
worldwide interest, has been applied to Korean children and that the perceived and psychological
health effects have been grasped, which will contribute to the spread of health promotion programs
using nature in the future.
Author Contributions: K.-S.B. contributed toward the research design, intervention, data collection, analyses,
and writing of the paper. S.K. contributed toward the intervention, data collection, and writing of the paper.
M.K.S., K.I.K., and Y.J. contributed toward the intervention, data collection, and writing of the paper.
Funding: This research was supported by the National Research Foundation of Korea (NRF) grant funded by the
Korea government (Reference number: NRF-2016R1A2B4007767).
Conflicts of Interest: The authors declare no conflict of interest. The founding sponsors had no role in the design
of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the
decision to publish the results.
References
1. Choi, I.; Mo, S.; Lee, S. A Study on Mental Health Improvement Policy for Children and Adolescents II; National
Youth Policy Institute: Seoul, Korea, 2012.
2. Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.;
Okely, A.D.; Connor Gorber, S.; et al. Systematic review of sedentary behaviour and health indicators in
school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [CrossRef]
[PubMed]
3. Son, J.W.; Ha, S.Y. Examining the influence of school forests on attitudes towards forest and aggression for
elementary school students. J. Korean Inst. For. Recreat. 2013, 17, 49–57.
4. Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press:
New York, NY, USA, 1989.
5. Corraliza, J.A.; Collado, S.; Bethelmy, L. Nature as a moderator of stress in urban children. Procedia-Soc.
Behav. Sci. 2012, 38, 253–263. [CrossRef]
6. Korpela, K.; Kyttä, M.; Hartig, T. Restorative experience, self-regulation, and children’s place preferences.
J. Environ. Psychol. 2002, 22, 387–398. [CrossRef]
7. Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of nature therapy: A review of the research in Japan.
Int. J. Environ. Res. Public Health 2016, 13, 781. [CrossRef] [PubMed]
8. The National Law Information Center Forestry Culture and Recreation Act. Available online: http://www.
law.go.kr/main.html (accessed on 20 March 2017).
9. Howard, J. Integrating Outdoor Experience with Curricular Learning. Available online: https://www.wcmt.
org.uk/sites/default/files/report-documents/Howard%20J%20Repor%202015%20Final.pdf (accessed on
10 March 2017).
10. Muñoz, S.-A. Children in the Outdoors; Sustainable Development Research Centre: London, UK, 2009.
11. McCormick, R. Does access to green space impact the mental well-being of children: A systematic review.
J. Pediatr. Nurs. 2017, 37, 3–7. [CrossRef] [PubMed]

Int. J. Environ. Res. Public Health 2018, 15, 1977
10 of 11
12. Kim, S.A.; Joung, D.; Yeom, D.G.; Kim, G.; Park, B.J. The effects of forest activities on attitudes toward forest,
stress, self-esteem and mental health of children in community child centers. J. Korean Inst. For Recreat. 2015,
19, 51–58.
13. Kim, J.Y.; Shin, C.S.; Yeoun, P.S.; Yi, J.Y.; Kim, M.R.; Kim, J.K.; Yoo, Y.H. Forest healing program impact on the
mental health recovery of elementary school students. J. Korean Inst. For. Recreat. 2013, 17, 69–81. [CrossRef]
14. Choi, J.-H.; Kim, K.-E. Eating attitude of children using community child center: A structural equation
modeling approach. Adv. Sci. Technol. Lett. 2014, 47, 351–356.
15. Song, M.K.; Bang, K.-S. A systematic review of forest therapy programs for elementary school students.
Child Health Nurs. Res. 2017, 23, 300–311. [CrossRef]
16. Kang, K.; Kim, S. Health problems and related factors of socially vulnerable school-age children in Seoul.
J. Korean Soc. School Health 2017, 30, 181–193.
17. Taelman, J.; Vandeput, S.; Spaepen, A.; Van Huffel, S. Influence of Mental Stress on Heart Rate and Heart
Rate Variability. In Proceedings of the 4th European Conference of the International Federation for Medical
and Biological Engineering (IFMBE), Antwerp, Belgium, 23–27 November 2008; pp. 1366–1369.
18. Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2015.
19. Han, E.; Yoo, A.-J. Children’s and adolescents’ depression, attributional style and academic achievement.
J. Korean Home Econ. Assoc. 1994, 32, 147–157.
20. Kim, Y.-J. Effects of Solution-Focused Brief Group Counseling Program on the Isolated Elementary School
Children’s Peer Relationship and Self-Esteem. Master’s Thesis, Korea National University of Education,
Cheongju, Korea, 2005.
21. Bahn, G.-H.; Shin, M.-S.; Cho, S.C.; Hong, K.-E. A preliminary study for the development of the assessment
scale for ADHD in adolescents: Reliability and validity for cass(s). Korean J. Child Adolesc. Psychiatry 2001, 12,
218–224.
22. Field, A. Discovering Statistics Using IBM SPSS Statistics, 4rd ed.; Sage: Los Angeles, CA, USA, 2013.
23. Gignac, G.E.; Szodorai, E.T. Effect size guidelines for individual differences researchers. Personal. Individ.
Differ. 2016, 102, 74–78. [CrossRef]
24. Wolf, T.J.; Spiers, M.J.; Doherty, M.; Leary, E.V. The effect of self-management education following mild
stroke: An exploratory randomized controlled trial. Top. Stroke Rehabil. 2017, 24, 345–352. [CrossRef]
[PubMed]
25. Reed, K.; Wood, C.; Barton, J.; Pretty, J.N.; Cohen, D.; Sandercock, G.R. A repeated measures experiment of
green exercise to improve self-esteem in UK school children. PLoS ONE 2013, 8, e69176. [CrossRef] [PubMed]
26. Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health?
A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [CrossRef] [PubMed]
27. Choi, S.-J.; Koh, Y.-S. Effect of combined program of horticultural therapy and forest therapy on self-esteem,
social competence, and life respect of low-income family children at community children’s center. J. School
Soc. Work 2014, 29, 671–699.
28. Cho, Y.M.; Shin, W.S.; Yeoun, P.S. The influence of forest experience program length on sociality and
psychology stability of children from low income families. J. Korean Inst. For. Recreat. 2011, 15, 97–103.
29. Kim, M.H. A study on the positive effects of forest activities for children from economically underprivileged
households on their emotional state, life satisfaction, and ego-resilience. Korean J. Child Stud. 2014, 35,
223–247. [CrossRef]
30. Wood, C.; Gladwell, V.; Barton, J. A repeated measures experiment of school playing environment to increase
physical activity and enhance self-esteem in UK school children. PLoS ONE 2014, 9, e108701. [CrossRef]
[PubMed]
31. Karcher, M.J. The study of mentoring in the learning environment (SMILE): A randomized evaluation of the
effectiveness of school-based mentoring. Prev. Sci. 2008, 9, 99–113. [CrossRef] [PubMed]
32. Kim, N.S. Designing youth mentoring for disadvantaged family. Korean J. Youth Stud. 2011, 18, 355–380.
33. Rhodes, J.E. Stand by Me: The Risks and Rewards of Mentoring Today’s Youth; Harvard University Press:
Cambridge, MA, USA, 2009.
34. Yadav, V.; O’Reilly, M.; Karim, K. Secondary school transition: Does mentoring help ‘at-risk’ children?
Community Pract. 2010, 83, 24–28. [PubMed]

Int. J. Environ. Res. Public Health 2018, 15, 1977
11 of 11
35. Duncan, M.J.; Clarke, N.D.; Birch, S.L.; Tallis, J.; Hankey, J.; Bryant, E.; Eyre, E.L. The effect of green exercise
on blood pressure, heart rate and mood state in primary school children. Int. J. Environ. Res. Public Health
2014, 11, 3678–3688. [CrossRef] [PubMed]
36. Sharma-Brymer, V.; Bland, D. Bringing nature to schools to promote children’s physical activity. Sports Med.
2016, 46, 955–962. [CrossRef] [PubMed]
37. Lee, A.C.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public
Health 2011, 33, 212–222. [CrossRef] [PubMed]
38. Barton, J.; Sandercock, G.; Pretty, J.; Wood, C. The effect of playground-and nature-based playtime
interventions on physical activity and self-esteem in UK school children. Int. J. Environ. Health Res.
2015, 25, 196–206. [CrossRef] [PubMed]
39. O’Brien, L.; Murray, R. Forest School and its impacts on young children: Case studies in Britain. Urban For.
Urban Green. 2007, 6, 249–265. [CrossRef]
40. Louv, R. Last Child in the Woods: Saving Our Children from Nature-Deficit Disorder; Algonquin books of Chapel
Hill: Chapel Hill, NC, USA, 2008.
41. Tsunetsugu, Y.; Lee, J.; Park, B.-J.; Tyrväinen, L.; Kagawa, T.; Miyazaki, Y. Physiological and psychological
effects of viewing urban forest landscapes assessed by multiple measurements. Landsc. Urban Plan. 2013,
113, 90–93. [CrossRef]
42. Bang, K.-S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.-K.; Park, B.-J.; Song, M.K. The Effects of a Campus
Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health.
Int. J. Environ. Res. Public Health 2017, 14, 728. [CrossRef] [PubMed]
43. Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku
(taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across
Japan. Environ. Health Prev. Med. 2009, 15, 18. [CrossRef] [PubMed]
44. Lee, I.; Choi, H.; Bang, K.-S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms
among adults: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 321. [CrossRef] [PubMed]
45. Cho, Y.M.; Kim, D.J.; Lee, K.H.; Lee, H.E.; Lee, Y.J. A study on effect of forest related programs based on the
meta-analysis. J. Korean Inst. For. Recreat. 2015, 19, 1–13.
46. Akrimi, S.; Raynor, S.; Johnson, R.; Wylie, A. Evaluation of SHINE—Make every child count: A school-based
community intervention programme. J. Public Ment. Health 2008, 7, 7–17. [CrossRef]
47. Nursing and Midwifery Council. Standards for Competence for Registered Nurses. Available
online: https://www.nmc.org.uk/globalassets/sitedocuments/standards/nmc-standards-for-competence-
for-registered-nurses.pdf (accessed on 10 March 2017).
48. Kim, S.; Bang, K.-S.; Kang, K.; Song, M.K. Mentoring experience of nursing students participating in a health
promotion program for elementary school students. J. Korean Acad. Soc. Nurs. Educ. 2018, 24, 137–148.
49. Leventhal, K.S.; DeMaria, L.M.; Gillham, J.E.; Andrew, G.; Peabody, J.; Leventhal, S.M. A psychosocial
resilience curriculum provides the “missing piece” to boost adolescent physical health: A randomized
controlled trial of Girls First in India. Soc. Sci. Med. 2016, 161, 37–46. [CrossRef] [PubMed]
50. Rubenstein, L.M.; Hamilton, J.L.; Stange, J.P.; Flynn, M.; Abramson, L.Y.; Alloy, L.B. The cyclical nature of
depressed mood and future risk: Depression, rumination, and deficits in emotional clarity in adolescent
girls. J. Adolesc. 2015, 42, 68–76. [CrossRef] [PubMed]
51. Han, K.-T. The effect of nature and physical activity on emotions and attention while engaging in green
exercise. Urban For. Urban Green. 2017, 24, 5–13. [CrossRef]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access
article distributed under the terms and conditions of the Creative Commons Attribution
(CC BY) license (http://creativecommons.org/licenses/by/4.0/).