
Article
The Physiological and Psychological Effects Benefits of Forest
Therapy (FT) on Tourists in the Kranjska Gora Destination
Darija Cvikl 1,2,*, Cvetka Avguštin 3 and Samo Kreft 4
1 Vocational College for Hospitality, Wellness and Tourism Bled, Prešernova 32, 4260 Bled, Slovenia
2 International Society of Forest Therapy, Piaristengasse 1, 3500 Krems, Austria
3 South Easthern Europe Forest Medical Alliance, 11000 Belgrade, Serbia
4 Faculty of Pharmacy, University of Ljubljana, Aškercˇeva 7, 1000 Ljubljana, Slovenia
* Correspondence: darija.cvikl@vgs-bled.si; Tel.: +386-51-608-251
Abstract: To explore the effects of forest therapy in the Kranjska Gora tourist destination, experimental
research on 50 tourists was implemented. By designing and following a specific forest therapy
protocol, the physiological stress markers and psychological effects on tourists were measured. The
results provide clear evidence of positive effects and health benefits on tourists. Additionally, the
forest therapy experience is presented through the tourists’ fit-back and perception. The research
results could be very useful for destination management, tourist providers, and the development of a
forest therapy tourism activities, as well as the well-being forest tourism.
Keywords: forest therapy; tourists; physiological and psychological effects; cortisol; dhea (dehy-
droepiandrosterone); SPANE; PHI I; PHI II
Citation: Cvikl, D.; Avguštin, C.;
Kreft, S. The Physiological and
Psychological Effects Benefits of
Forest Therapy (FT) on Tourists in the
Kranjska Gora Destination. Forests
2022, 13, 1670. https://doi.org/
10.3390/f13101670
Academic Editors: Qing Li, Won
Sop Shin and Christos Gallis
Received: 19 August 2022
Accepted: 5 October 2022
Published: 11 October 2022
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2022 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
1. Introduction
The development of forest therapy (FT) was triggered by the need to relax in the forest
and to isolate from various stressors. Professor Qing Li, of Department of Rehabilitation
Medicine, Nippon Medical School Hospital, Japan, the world’s foremost expert in forest
medicine and immunology, and Amos Clifford, the founder of the US-based Association of
Nature and Forest Therapy, the world-leading organization in the movement to integrate
nature and forest therapies, recognize FT as a method in which the natural environment
of the forest is used for health care practices. There are many research studies about
the positive physiological and psychological beneficial impacts and effects of the forest
environment on human health and well-being so far [1–6], and several review articles on
the same subject [7–10], but very little on tourists at a tourist destination.
The connection between forest bathing and the field of tourism was made by Konu
(2015) in her definition of forest well-being tourism. Furthermore, the authors Ohe, Ikei,
Song, and Miyazaki (2017) later defined forest therapy tourism (FTT) as an emerging
tourism activity. With a relatively new tradition of maintaining personal health and
well-being, the so-called ‘forest bath’ (or jap. shinrin-yoku), a type of forest relaxation
theory, combined with recreation [1,11], and a touristic activity [12], a new type of tourist
product could be created. An integration of tourism and health services could lead to
the development of a forest therapy tourist product [13], and subsequently also to the
quality development and institutionalization of forest tourism as a specific type of tourist
activity [14,15]. FTT therefore has two aspects: it can be used for patients in support of
therapy and for tourists in pursuit of wellness tourism.
Therapeutic forest activities that are already carried out in tourism practice, include
naturopathic elements, such as water immersion (e.g., Kneipp therapy) and climatotherapy
(climatic terrain cure, heliotherapy, and fresh-air rest cure) to enhance the health benefits
of forest mindedness and nutritional therapy [7,15,16]. Some countries, among the first of
which were Japan and China [17], as well as Sweden [18], carry out public health promotion
Forests 2022, 13, 1670. https://doi.org/10.3390/f13101670
https://www.mdpi.com/journal/forests
Forests 2022, 13, 1670
2 of 21
in the forest in addition to forest tourism activities, while in Germany, FT is incorporated
into the national health system [13]. In Poland, citizens stated that recreational activity
in urban green spaces and forests reduced stress caused by the COVID-19 pandemic. On
this basis, the Polish Tourist Organization is planning to examine the new travel habits
of domestic tourists [19]. The forest has a therapeutic effect and relieves many symptoms
of respiratory diseases, psychosomatic diseases, mental illnesses, cardiovascular diseases,
lifestyle disorders, oncological diseases, neurological diseases, and certain orthopedic
diseases, and it preventively strengthens human physical and mental health [20]. There is
growing tourist use of socio-cultural forest values for therapeutic tourism purposes, and
the connection between FT and tourism is evident [21].
Undoubtedly, there is an embracement of FT as a new healthy activity among different
stakeholders within the tourism industry, where health is recognized as new wealth. To
find out the healing effects of the Kranjska Gora destination forest area on tourists, the
physiological stress markers [22] and psychological parameters were measured. Cortisol
concentration, DHEA concentration, systolic blood pressure, diastolic blood pressure, and
heart rate are commonly used parameters for the immune system and general human well-
being [5,6,23]. SPANE is a commonly used scale for measuring human well-being [24,25].
The need for the Pemberton happiness index [26], a measure of well-being that integrates
various aspects of an individual’s well-being, was recognized, beside the positive and
negative emotions. The PHI is a general measure of human well-being that contains
both hedonic and eudaimonic elements of well-being. Additionally, the PHI focuses
on psychological factors that could influence the well-being assessment. Pemberton’s
happiness index consists of two scales, one that assesses remembered well-being and
includes the domains of general, hedonic, eudaimonic, and social well-being. The second
scale experienced well-being, where positive and negative events that could be related to
experiencing well-being are listed.
This research wants to enlighten not only the physiological and psychological thera-
peutic effects of the forest on tourists, but also the applicability of FT in the tourism industry
2. Materials and Methods
The research took place in the Kranjska Gora destination (see Figure 1), an Alpine
valley with developed tourist infrastructure, which lies in the northwestern part of Slovenia,
right next to the border with Austria and Italy.
Figure 1. Kranjska Gora valley.
The interdisciplinary team of specialists conducted this research. One of them was
the specialist for forest tourism from the Vocational College for Hospitality, Wellness and
Tourism Bled, Slovenija, the other was the fito-pharmacy specialist from the Faculty of

Forests 2022, 13, 1670
3 of 21
Pharmacy, University of Ljubljana, and the third was the doctor specialist of internal and
social medicine and ANFT certificated guide to FT (see Appendix A, Figure A1). Physiolog-
ical measurements were examined and conducted by a certified laboratory and medical
equipment, and validated by the Ministry of Health (see Appendix B, Figure A2). A clini-
cally validated monitor device was used for blood pressure monitoring. All psychological
tests (SPANE, PHI I, and PHI II) were validated by the Department of Psychology at The
Faculty of Arts, University of Ljubljana.
2.1. Population Definition
The research recruited 50 male and female adult volunteers (hereinafter referred to as
tourists) who were willing to spend forty-eight (48) hours at the destination of Kranjska
Gora. One of the main definitions of a tourist that distinguishes a tourist from a day tripper
or excursionist is an overnight stay of 24 h or more away from home (Jafari and Xiao, 1957).
The recruitment of volunteers was made via a public call on the website of the Municipality
of Kranjska Gora. The information was also shared on social media. Fifty volunteers were
included in the study. On the day the survey began, 47 volunteers arrived at the site, and
3 dropped out due to possible COVID-19.
2.2. Forest Therapy Sessions
A few days before the tourists arrived, all four forest therapy (FT) guides met at the
destination of Kranjska Gora and selected individual forest locations where they later
guided the tourists through FT sessions. On the day the forest therapies (FT) were per-
formed, the four FT guides met in the morning to check the details of the FT protocol
once again, and they took time to connect with nature and with themselves in silence
immediately before conducting the FT sessions. After that, each FT guide joined his group
of tourists and provided a short introduction, a personal presentation, and a presentation
regarding the destination of Kranjska Gora. Before the FT started, the tourists were invited
to be extremely respectful of nature, to be careful while walking, and to manage their fluid
intake and sun protection. This was followed by a short presentation about the basics of FT.
The tourists were exposed to two conducted forest therapies in the forest. They walked,
altogether, approximately 1 km during each of the two FT sessions on pre-selected forest
paths. A guided structured walk, with an ANFT certified forest therapists (see Appendix A,
Figure A1) was used as a method of exposure to the forest, as described below.
In the introductory circle, each tourist stated his name and described why he was
grateful that day and identified his favourite creature from nature or favourite type of tree.
This was followed by invitations in accordance with the standard FT sequence: pleasure of
presence, what’s in motion, and tea. Between what’s in motion and tea, the forest therapy
guides included two of the following invitations in the morning or afternoon: socializing
with water, mirrors, time for yourself, and small things. Each volunteer, therefore, experi-
enced all the invitations. The conduct of the “Pleasures of Presence” invitation: In a flat
and open area, the guide asked tourists to form a circle and when ready to close their eyes
(or keep them softly open). The guide invited them to focus on their senses, one at a time.
He asked: “What scents do you perceive? What sounds can you hear far away? Which
ones are closest to you? Can your skin feel the wind?” The guide then asked tourists to
open their eyes very slowly and imagine they are seeing the world for the very first time.
The conduct of the “What’s in Motion” invitation: The guide invited the group to
walk very slowly for approximately 10 to15 min and observe whatever is in motion (insects,
leaves in the wind, etc). At the end of this invitation, the guide asked tourists to choose
a “being” in the forest—such as a leaf or a rock—and pass it around the group. As each
person held that being, they shared their experiences, while others practiced deep listening.
At the end of the time designated for each invitation, the guides invited the tourists to
form a circle to share their experiences. During the tea session, the guides offered the
tourists sunflower and pumpkin seeds and dried cranberries and thanked them for taking
part in the walk. Together, the guides and the tourists then thanked nature for revealing

Forests 2022, 13, 1670
4 of 21
itself to them and returned a cup of tea to the earth for this purpose. Before that, each
guide expressed his intention and/or what he wanted to give back to nature through his
offering of tea. This concluded the FT session. Then, during a snack, the tourists chatted
individually or in small groups and shared the messages they received from nature, and
they headed toward their accommodations.
2.3. Research Protocol Design
In the following, we present the designed protocol, which was followed by all partici-
pants of the research.
1. Step. Defining of the physiological and psychological parameters according to the
purpose of the research.
2. Step. Sample criterion. Two selected criterions were followed. The first was based
mainly on the fact that participants have to define themselves as tourists, which is
why the accommodation for all of them was arranged at the destination for two
(2) nights. The second was based on the accommodation facilities capacity. Fifty beds
were provided by the municipality and the tourist organizations in situ, so fifty (50)
voluntarily registered adults of the male and female sex, who were willing to spend
forty-eight (48) hours at the destination of Kranjska Gora, were planned by design.
3. Step. To define the sampling method. An online announcement was chosen for the
recruitment of volunteer participants on the website of the Municipality of Kranjska
Gora, as well as through shared information on social networks. Fifty (50) volunteers
were planned to be included in the study.
4. Step. Inclusion criteria: volunteers in the age group 19 to 100, both sexes.
5. Step. Exclusion criteria: persons unable to complete the questionnaire; persons
unable to walk in the woods; persons who did not submit all the necessary samples
before and after the therapies; persons who did not adhere to the deadlines in the
implementation protocol and who submitted samples or completed questionnaires
late or at different deadlines.
6. Step. Research itinerary.
a. Before arriving in Kranjska Gora, all registered tourists were informed by e-mail
in detail about the course and purpose of the research. All the participants
were invited to sign a voluntary statement of informed consent to participate in
the survey.
b. All registered tourists were asked to fulfill a psychological questionnaire online
on Wednesday, 16 June 2021 in their usual environment, two days before arriv-
ing at destination at a specific time, between 8 and 9 am. They did the same
the second time after both forest therapies at the Kranjska Gora destination.
The participants were answered the questionnaire both times at the same time:
between 8 and 9 am.
c. Registered tourists were randomly divided into 4 groups according to ANFT
protocol sample size criteria (12 or 13 participants in each group). Each group
acted as a unit that was accommodated separately. Each participant was accom-
modated in a 4-star accommodation at the Kranjska Gora destination tourist
providers. One of them, Jasna Chalet, is shown in Figure 2. Each group was
provided with its own assistants to perform the measurements, and each group
had its own forest therapist. The groups did not meet each other (except at a
joint meeting).
d. On Friday, 18 June 2021 (day 1), after arriving in Kranjska Gora, all regis-
tered participants were informed once again about the course and purpose of
the research.
e. On Saturday, 19 June 2021, after the first night sleeping in the destination, all par-
ticipants became tourists. After breakfast, all tourists provided their first saliva
samples in the morning to measure stress hormone concentrations (cortisol and
DHEA), blood pressure (systolic and diastolic), and heart rate. Sampling tubes
Forests 2022, 13, 1670
5 of 21
and sampling instructions were provided by the same laboratory mentioned
above. The collection of a saliva samples prevailed over the collection of a
blood samples, mainly to avoid possible inconveniences or stress from needle
insertion, and because it is more user-friendly.
f. On Saturday, 19 June 2021, during the day, tourists divided into 4 groups 2×
(1× morning and 1× afternoon) and participated in FT. The first FT session
lasted 3 h and was conducted between 10 am and 1 pm, and the second lasted for
2 h between 3 pm and 5 pm. Forest therapies were performed by ANFT-certified
guides according to the protocol of the educational institution.
g. On Sunday, 20 June 2021 (after the second night at the resort), all tourists
participated in the survey in the morning between 8 and 9 am and took the
same set of tests and measurements as on Saturday, at the same time as the
previous day.
h. They also filled in the psychological questionnaire again, which they filled in at
home 2 days before arriving in Kranjska Gora. The time of completion of the
questionnaire was defined between 8 and 9 o’clock in the morning.
i. Saliva samples were agreed to be delivered on 21 June 2021 to the diagnostic
laboratory, which performed the necessary physiological measurement results.
j. All participants gave signed conscious and free consent to the research. All
volunteers who decided to participate in the research were informed in an
appropriate and understandable way about the purpose, plan, and methods of
the research. They were also informed that they could withdraw their consent at
any time without explanation. They were promised data protection as well. All
voluntarily registered tourists registered in writing and undertook to comply
with the PCT conditions in force at the time of the survey.
k. Data collection and analysis. Each registered tourist was be registered by name
and surname. At the suggestion of the loratory that performed the sample
analysis, we abandoned the original idea of recording with computer-generated
code. The proposal of the laboratory to perform the analysis is to state names
and surnames, as in the case of an incorrect or duplicate code number, the
sample and/or duplicate samples must be discarded. All data were to be
used only to prepare a report on the results of the research and a research
article, without providing personal data. The rest of the biological material was
professionally (routinely) discarded and destroyed.
Figure 2. Jasna Chalet Resort by the lake Jasna, Slovenia: http://jasnaresort.com/en/ (accessed on
22 June 2022).

Forests 2022, 13, 1670
6 of 21
3. Results
In this study, a set of fifty (50) participants was reached. They all agreed to take ac-
quired physiological and psychological measurements according to protocol. Additionally,
they agreed to obtain the status of a tourist by accepting two nights of accommodation in
the Kranjska Gora destination.
Of the 50 selected volunteers, 47 valid samples for physiological measurements were
obtained. Due to the COVID-19 or non-submission of a saliva sample prior to therapy,
three participants canceled their registration or did not completely fulfill the required
physiological measurements. A total of 47 participants were present during all of the study
process (Figure 3) and participated in two forest therapies, according to research protocol.
In addition, each participant filled out two psychological questionnaires twice. Due to
incomplete answers or unsubmitted questionnaires, 7 questionnaires were invalid and
43 valid questionnaires were obtained for further processing of the results.
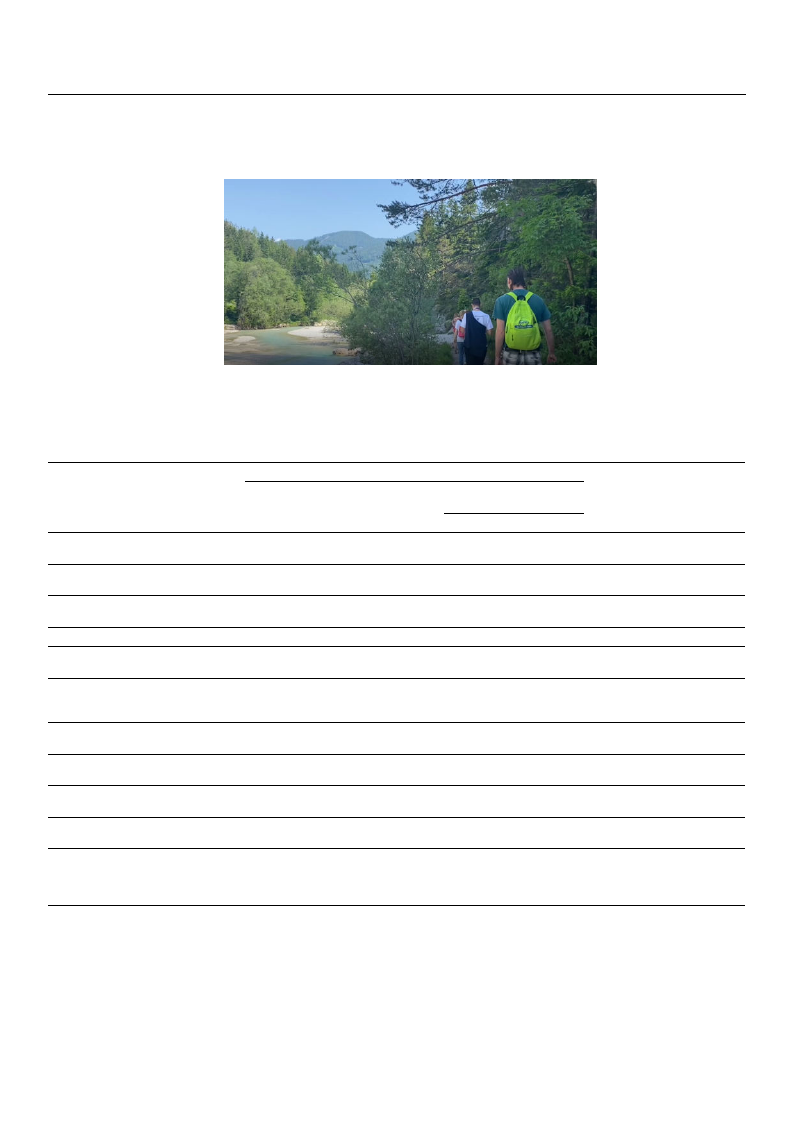
Figure 3. Of the fifty volunteers, forty-seven arrived and accommodated in the Kranjska Gora
destination forest area.
In accordance with the protocol, the measurement of following parameters was re-
alised according to the study protocol design before and after the FT experience at the
Kranjska Gora destination:
• stress-indicating hormone DHEA (dehydroepiandrosterone) with saliva sample;
• stress-indicating hormone cortisol with saliva sample (Figure 4);
• blood pressure (systolic and diastolic) (Figure 5);
• heart rate;
• stress index;
• the scale of positive and negative experience (SPANE);
• the Pemberton happiness index (PHI I and PHI II).
Physiological measurements were conducted according to instructions of Diafit,
d.o.o., Spodnji Slemen 6, 2352 Selnica ob Dravi, Slovenia. The clinically validated mon-
itor device Model M6AC (Omron Healthcare Co Ltd.: Muko-shi, Japan) (Model M6AC:
OMRON M3: http://www.dableducational.org/Publications/2014/ESH-IP%202010%2
0Validation%20of%20Omron%20M6%20AC%20(HEM-7322-E).pdf (accessed on 18 August
2022)) was used for blood pressure monitoring. All psychological tests (SPANE, PHI I, and
PHI II) were validated by the Department of Psychology at The Faculty of Arts, University
of Ljubljana.

Forests 2022, 13, 1670
7 of 21
Figure 4. Taking the saliva sample of participant.
Figure 5. Blood pressure measurement with validated and clinically approved device.
3.1. Stress Marker Parameters—Overall Average and by Gender
The mean values of most of the measured parameters (markers of stress) were higher
in men than in women (see Tables 1 and 2), with two exceptions out of ten (diastolic
pressure before FT and heart rate after FT), which were higher in women. The largest
difference was in the concentration of the hormone DHEA in saliva before FT, which was,
on average, more than two times higher in men than in women. However, none of the
gender differences were statistically significant.
Average concentrations of the two stress-indicating hormones cortisol and DHEA
before and after FT are given in Table 1 below.
Average results of systolic and diastolic pressure, both before and after FT experience,
are given in Table 2 below.
Forests 2022, 13, 1670
8 of 21
Table 1. Average concentrations of the two stress-indicating hormones cortisol and DHEA before
and after forest therapy.
Gender Mean
N
Std.
Dev.
Min. Max.
Significance of the
Difference between
Genders (p)
Cortisol—before
(nmol/L)
M
F
Total
8.16 10 3.64 4.00 15.60
7.96 36 3.31 3.10 16.60
8.00 46 3.34 3.10 16.60
0.870
Cortisol—after
(nmol/L)
M
F
Total
8.47 10 3.17 4.50 14.70
7.44 37 3.02 2.50 14.60
7.66 47 3.05 2.50 14.70
0.352
DHEA—before
(pg/mL)
M
F
Total
1411
684
842
10 2451
36 527
46 1228
200 8335
89 2502
89 8335
0.098
DHEA—after
(pg/mL)
M
F
Total
827
10 486 108 1582
563
37 342
71 1900
619
47 387
71 1900
0.055
Table 2. Average values of heart parameters (pressure and rate) before and after forest therapy.
Gender Mean
N
Std.
Dev.
Significance of the
Min. Max. Difference between
Genders (p)
Systolic
pressure—before
(mm Hg)
M
F
Total
126.4 10 12.0 106 137
118.9 37 19.8 91 182
120.5 47 18.6 91 182
0.265
Systolic
pressure—after
(mm Hg)
M
F
Total
119.7 10 10.0 103 132
115.8 37 17.8 91 177
116.6 47 16.4 91 177
0.519
Diastolic
pressure—before
(mm Hg)
M
F
Total
76.3 10 7.3 67 87
76.9 37 10.6 62 115
76.8 47 10.0 62 115
0.859
Diastolic
pressure—after
(mm Hg)
M
74.3 10 8.4 57 84
F
73.7 37 11.0 58 123
Total
73.8 47 10.4 57 123
0.892
M
78.4 10 10.8 64 93
Heart rate—before
(1/min)
F
77.3 37 10.5 58 102
Total
77.5 47 10.5 58 102
0.778
M
72.4 10 10.6 55 84
Heart rate—after
(1/min)
F
74.6 37 9.0 54 93
Total
74.1 47 9.3 54 93
0.511
3.2. Comparison of Parameters before and after Forest Therapy
To compare the measured parameters before and after FT, the differences were cal-
culated (Table 3). We can see that in the entire population after FT, all five stress markers
decreased compared to their values before FT. Additionally, in the separate calculation
Forests 2022, 13, 1670
9 of 21
for each gender, we see that in women, the results of all five measurements decreased,
and in men, the results of four measurements decreased; only cortisol increased slightly
(statistically insignificantly) from 8.16 to 8.47 nmol/L, which is 3.8% of the initial value. In
women, cortisol decreased by 6.5%, which was also not significant.
Table 3. Differences in average values of measurements of physiological parameters before and after
forest therapy.
Cortisol
DHEA
Systolic
pressure
Diastolic
pressure
Heart
rate
Gender
M
F
Total
M
F
Total
M
F
Total
M
F
Total
M
F
Total
Average
−0.3200
0.4556
0.2870
584.6
118.5
219.8
6.7000
3.0541
3.8298
2.0000
3.1622
2.9149
6.0000
2.7027
3.4043
N Std. Deviation Min.
10
1.77
−3.20
36
2.73
−6.40
46
2.56
−6.40
10
2213.6
−549
36
284.8
−358
46
1039.6
−549
10
11.06
−8
37
7.97
−11
47
8.72
−11
10
5.92
−10
37
7.37
−9
47
7.04
−10
10
7.39
−10
37
7.96
−14
47
7.88
−14
Max.
2.40
6.40
6.40
6846
1207
6846
29
19
29
11
22
22
15
26
26
Significance of the
Difference between
Genders (p)
0.403
0.213
0.245
0.649
0.245
Significance of
Difference
before–after FT (p)
0.594
0.325
0.450
0.425
0.017
0.158
0.088
0.026
0.004
0.314
0.013
0.007
0.030
0.046
0.005
The hormone dehydroepiandrosterone (DHEA) decreased much more than cortisol
during FT. It decreased by 26% in the general population, by 41% in men, and by 18% in
women. Because men had high variability in this hormone, this decrease was not significant
in men and the general population, but it was significant in women. The decrease in systolic
pressure, diastolic pressure, and heart rate (pulse) was statistically significant both in the
entire population and in a separate analysis of the female subpopulation. In men, due to
greater variability, lower pressure reduction was not significant.
3.3. Stress Index
Stress is a human condition that is reflected in different individuals with slightly differ-
ent changes in individual physiological parameters, and the measurements of physiological
parameters are influenced by other factors and random error. As a result, the state of stress
can be measured more accurately by calculating the stress index, where part of the random
error and individual characteristics is reduced due to the larger number of measurements
included in one parameter.
In this study, the stress index is calculated as the average of the normalized values of
all five measured physiological parameters according to the following formula:
stress index =
cortizol
nk
+
DHEA
nD
+
sist
ns
+
diast
nd
+
rate
np
5
∗ 100
As normalization coefficients (nk, nD ns, nd, and np), we used the average normal values
of each of the parameters as follows: ten (10) for cortisol, one thousand (1000) for DHEA,
one hundred and twenty (120) for systolic pressure, eighty (80) for diastolic pressure, and
Forests 2022, 13, 1670
10 of 21
Gender
Stress—
before
Stress—
after
Stress—
difference
Male
Female
Total
Male
Female
Total
Male
Female
Total
seventy (70) for pulse. In this study, the stress index decreased during FT (Table 4) by more
than 7% in the entire population. The decrease was 5% for women and 13% for men.
Table 4. Average values of the stress index before and after forest therapy.
Mean
107.10
90.51
94.04
92.70
85.22
86.81
14.40
5.28
7.22
Significance of the
Significance of
N Std. Deviation Minimum Maximum Difference between Difference before—after
the Genders (p)
Therapy (p)
10
53.68
76.89
256.03
37
15.30
63.91
144.39
0.099
47
28.18
63.91
256.03
10
12.86
78.30
110.83
37
12.05
66.06
128.01
0.093
47
12.47
66.06
128.01
10
46.41
−7.53
145.19
0.352
37
9.98
−11.76
24.19
0.264
0.003
47
22.66
−11.76
145.19
0.034
The decrease in the stress index was statistically significant both in the overall pop-
ulation and in a separate analysis of the female subpopulation. In men, due to greater
variability or lower pressure reduction, the decrease in the stress index was not significant,
although the decrease was higher than in women.
We observed that in volunteers who had a higher level of stress at the first mea-
surement, the stress reduction during FT was higher. Therefore, we made an additional
calculation from which we excluded 19 volunteers with a stress index at the first measure-
ment of less than 85. In the remaining 28 volunteers with higher stress, the reduction in the
stress index was as much as 11.7%. In the overall population, there was an improvement
of 7%.
3.4. Psychological Tests—Results of Paired Positive and Negative Experience as well as Hedonic
and Eudaimonic Elements of Well-Being Parameters
Psychological tests were taken two times. The first time at participants’ homes, and
second time after two (2) conducted FT sessions (1× morning and 1× afternoon) at the
Kranjska Gora destination forest area. The first FT session lasted 3 h and was conducted
between 10 am and 1 pm (Figure 6), and the second lasted for 2 h between 3 pm and
5 pm the same day on pre-selected forest paths in the vicinity of the accommodation
facilities. The groups did not meet each other during the research and forest therapies.
Forest therapies were performed by ANFT-certified guides according to the protocol of the
educational institution. We performed a non-parametric Wilcoxon two related samples test
on analyzing psychological tests. This test is used as an alternative to the paired samples
t-test, as data are not normally distributed (but the results are very similar to the Wilcoxon
test). The characteristic rate used in the calculations is 5%.
The scale of positive and negative experience (SPANE) before and after the FT experi-
ence display of paired samples of positive and negative experiences is presented in Table 5.
The recommended timeframe for a representative capture of emotions and experiences is
four (4) weeks, which was not possible for two reasons: limited financial resources and
the average length of stay, 2.5 days, which applies to the destination of Kranjska Gora
and Slovenia. These facts lead us to the decision to offer and enable all participants two
overnight stays in the destination of Kranjska Gora. We were interested in whether, when
measuring the emotional states in the period between 16 June 2021, and 20 June 2021,
despite a very short stay in the destination of Kranjska Gora, the emotional states of the
participants improve significantly. The results in Table 5 show that individual positive
emotions improved upward, while the impact of negative emotions decreased. Except
Forests 2022, 13, 1670
11 of 21
for the stress parameter, the results for all other measured parameters show statistically
significant positive results.
Figure 6. Forest therapy sessions conducted by an ANFT-certificated guide.
Table 5. The scale of positive and negative experience (SPANE) before and after the forest therapy
experience display of paired samples.
Paired Differences
Paired Sample t-Test
Mean
Std.
Deviation
Std. Error
Mean
95% Confidence Interval
of the Difference
t
df
Sig.
(2-Tailed)
Lower
Upper
Pair 1
positive
before—positive after
−0.750
0.839
0.126
−1.005
−0.495
−5.931 43
0.000
Pair 2
negative
before—negative after
1.205
0.878
0.132
0.938
1.472
9.099
43
0.000
Pair 3
good before—good
after
−0.614
0.813
0.123
−0.861
−0.366
−5.006 43
0.000
Pair 4
bad before—bad after
0.932
0.900
0.136
0.658
1.205
6.871
43
0.000
Pair 5
pleasant
before—pleasant after −
−0.955
0.861
−0.130
− −1.216 −
−0.693
−7.350 43
0.000
Pair 6
Pair 7
Pair 8
uncomfortable
before—uncomfortable
after
−
happy before—happy
after
−
sadly before—sadly
after
0.977
−0.705
0.909
0.902
0.851
0.984
0.136
−
0.128
−
0.148
0.703
−
−
−0.963
−
−
0.610
1.251
−0.446
1.208
7.188
43
−5.490 43
6.128
43
0.000
0.000
0.000
Pair 9
Pair 10
scared before—scared
after
−
joyfully
before—joyfully after
0.477
−1.159
0.876
1.010
0.132
−
0.152
0.211
−
−
−1.466
0.744
−0.852
3.615
43
−7.611 43
0.001
0.000
Pair 11
Pair 12
angry before—angry
after
stress before—stress
after
0.955
−0.091
1.077
2.429
0.162
0.366
0.627
−0.829
1.282
0.647
5.877
43
−0.248 43
0.000
0.805
The results of the Pemberton happiness index PHI I and PHI II are given in Tables 6 and 7.
Pair 3: worth useful before—worth useful after (with 2-tailed sig. 0.006), pair 8: important
before—important after (sig. 0.008), pair 10: bad moments before—bad moments after
(sig. 0.744) and pair 11: potential before—potential after (sig. 0.054) did not show statistically
better results, but all others, such as satisfaction, energy, worth usefulness, satisfaction
with yourself, learning experiences, and enjoyment, did show statistically significant
positive results.
Forests 2022, 13, 1670
12 of 21
Table 6. Pemberton happiness index PHI I before and after the forest therapy experience—display of
paired samples.
Paired Samples Test
Pair 1
satisfaction before—satisfaction after
Pair 2
energy before—energy after
Pair 3
worth useful before—worth useful after
Pair 4
satisfied with yourself before—satisfied with
yourself after
Pair 5
learning experiences before—learning
experiences after
Pair 6
connection before—connection after
Pair 7
problems before—problems after
Pair 8
important before—important after
Pair 9
enjoyment before—enjoyment after
Pair 10
bad moments before—bad moments after
Pair 11
potential before—potential after
b Based on negative ranks.
Z
−3.162 b
−3.230 b
−2.746 b
−3.061 b
−2.853 b
−3.224 b
−2.732 b
−2.667 b
−3.060 b
−0.327 b
−1.925 b
N
Sig. (2-Tailed)
43
0.002
43
0.001
43
0.006
43
0.002
43
0.004
43
0.001
43
0.006
43
0.008
43
0.002
43
0.744
43
0.054
Table 7. Pemberton happiness index PHI II before and after the forest therapy experience—display
of paired samples.
Paired Samples Test
Pair 1
proud before—proud after
Pair 2
overwhelmed before—overwhelmed after
Pair 3
fun before—fun after
Pair 4
bored before—bored after
Pair 5
enjoy doing before—enjoy doing after
Pair 6
worried before—worried after
Pair 7
learned something interesting before—learned
something interesting after
Pair 8
things happened that made me really angry
before—things happened that made me really
angry after
Pair 9
gave myself a treat before—gave myself a treat
after
Pair 10
felt disrespected before—felt disrespected after
b Based on negative ranks. c Based on positive ranks.
Z
−0.632 b
−4.811 c
−3.464 c
−1.732 c
−3.464 b
−4.600 c
−4.359 b
−3.162 c
−4.379 b
−2.828 c
N
Sig. (2-Tailed)
43
0.527
43
0.000
43
0.001
43
0.083
43
0.001
43
0.000
43
0.000
43
0.002
43
0.000
43
0.005
The PHI II measurements dealt with perceived well-being (see Table 7). All measured
parameters: overwhelmed, fun, enjoyed doing something, worried less, learned something
interesting, things happened that made me really less angry, gave myself a treat, felt
disrespected less, showed statistically significant positive results, except for the parameters
proud before—proud after, bored before—bored after.
3.5. Forest Therapy Experience Is Presented through the Tourists’ Fit-Back and Perception
Usable questionnaire results (completed 80% of all 13 questions) were submitted by
31 tourists, 27 women, (73% of all female tourists involved) and 4 men (40% of all male
tourists involved). A total of 66% of all 47 tourists participated in the survey. The highest
share of tourists (36%) was from the 45–54 age group. Fifty-two percent of the tourists
visit the forest several times per week, twenty-nine percent once per week, and thirteen
percent every day. Forty-five percent of the tourists usually spend 1–2 h per week in the

Forests 2022, 13, 1670
13 of 21
forest, twenty-three percent spend 2–4 h, nineteen percent spend 4–6 h and, the remaining
thirteen percent spend 6 h or more in the forest.
When asked about the impact of socializing with the forest on the mind, the tourist
respondents wrote some of the following: it relaxes me and distracts me from constantly
planning and thinking about future work obligations; it relaxes me, calms me down, I
feel good, reduces tension in the body; relaxing, anti-stress, improving concentration;
socializing with the forest has an extremely relaxing effect on me, it inspires me, it helps me
to clear my mind; disconnection of thought, reassuring; reassurance and clarity; positive,
encouraging; the forest forms positive thoughts, walks through the forest have the effect
of calming my mind; and easier concentration and focus. Among the answers to the
question of how socializing with the forest affects their emotions, we find the following:
pleasure, excitement; positive—I shake off any anger and bad mood; it has a relaxed,
calming and positive effect; everything seems more relaxed to me, thoughts are calm; I
am more loving to myself and to others, happy, joyful . . . ; joy and love overwhelm me in
the forest; soothing, meditative; it fills me with a sense of relaxation, happiness and joy;
calms them, e.g., euphoric; and very different, sometimes triggering joy, sometimes crying,
followed by relaxation, joy.
Most answers are about reduction in stress (calming, relaxing) and much less of the
answers are about stimulation (excitement, euphoric) of the mood. This is in line with the
expected effects of the FT, but can also be caused by the suggestive influence of the study.
When the tourists listen to the birds while socializing with the forest, when they breathe
the forest air and when they observe the natural environment, they reported feeling the
following: I feel nature and all its power, tranquility, joy, happiness, constantly happening
. . . ; peace, contentment, happiness; release; peace and joy; coexistence with nature; helps
to relax, drive away other thoughts; relaxation, joy of life, playfulness; energy, the power
of nature; the power of good feeling and wonder; peace in oneself and joy; and lightness,
calmness, curiosity . . . you could also say a kind of magic.
The scents the tourists perceive in the forest included the following: woody, the
smell of earth, conifers; I usually go through the woods too fast and do not detect odors;
depending on the period, the smell of spruce, mushrooms, cyclamen, earth; I would say
that I do not perceive the smell so much, it is such a forest smell that I often perceive, but
I really do not know what exactly emits this smell; in addition to the smell of the forest,
it seems to me that I often smell mushrooms; fragrances, freshness, moisture-water; the
smell of trees; moss, the smell of the morning, of the old house, of the wind and the shade;
I sense the freshness of fresh air that clears my lungs, and I breathe deeply; and coniferous
essential oils and flowering trees.
The tourists reported hearing the following sounds in the forest: birds singing, leaves
rustling; singing of birds, rustling of leaves, movement of animals through the undergrowth,
wind in the canopy; the sounds are cheerful and relaxing all the way from the chirping of
birds and the rustling of leaves; crickets, birds, rustling of leaves, cracking of dry twigs
underfoot; chirping, barking, breaking dry branches; the chirping of birds, the rustling of
trees, the sound of animals; in the forest I hear the chirping of birds, the sounds of various
insects, the noises of animals retreating before me, sometimes the barking of dogs from
the village, the ringing of the clock in the bell tower of a nearby village; birds, rustling
of canopies due to wind and undergrowth when walking; and the chirping of birds, the
movement of branches, the rustling of leaves, the wind in the canopy.
The tourists’ attention in the forest was most often also attracted by the following:
the green color of leaves, trees with their interesting shapes of leaves and bark, events
in undergrowth and canopy; something special constantly happening, that is, from the
movement and sounds of animals and plants; I am always fascinated by different shades of
colors; I notice the most different shades of green and autumn colors; I am very attracted to
winter in the forest; I admire the snow, the frost, the ice on the branches, and the footsteps
of the animals in the snow; tall, mighty trees, the smell of the forest, the chirping of birds;
wind and movement of plants, trees due to wind; it always seems to me as magical as if

Forests 2022, 13, 1670
14 of 21
the forest spoke in this way; trees, canopy, leaves on the ground (especially in autumn),
sometimes birds or clouds in the sky when I look at the canopy; and fluttering tree leaves;
ants, mice, deer.
Many tourists expressed the admiration of the nature in their answers of their attention,
sounds and scents in the forest. This could also have an influence on the relaxing effect of
the FT.
The tourists wrote about the role of the FT guide as follows: The guide helped us to
slow down, relax, do ordinary things in a different way and thus connect with ourselves,
with nature, which opens the way to the process of self-knowledge and self-healing—to
get the positive effects we need at a given moment; at the beginning it has an important
role—it has this role to stop us and remind us of all the happenings in the forest, which
we ourselves overlook or we completely forget that it is there, because we are always in a
hurry or we are thinking about other things, instead of relaxing and connecting with the
surroundings and experiencing it in its entirety; important—guiding, motivation, a kind of
mentoring—and with invitations, it somehow gives ideas and teaches you in all the ways
we can observe and explore the forest, connect with it; guides, helps and directs attention
to the purpose of the chosen therapy to focus on the perception of either hearing, sight,
smell; due to the different view, I did not know it was all so connected. In the end, I got the
message of the ancestors with the help of a guide who led the group; a FT guide can play
a very important role, especially for people who are not accustomed to such coexistence
with the forest and who would like to get closer to it. The guide can also make people
aware, show them how the forest can be healing for soul and body, and remind them that
the forest is our home—so we need to take care of it; the guide is the connecting thread
with the forest; guidance in returning to ourselves and in the awareness that we are part of
nature; it has a connecting and motivating role, it helps people to open up; connecting an
individual or groups with nature and vice versa. All the tourists reported that the forest
environment calms them, helps them to focus, and fills them with joy and connects them
with themselves.
4. Discussion
Based on the findings of the literature review, especially regarding the design of the
research protocol recommendations and limitations [14] (p. 31,38), we devoted special
attention to the protocol design. However, due to limitations in the conducted research,
positive findings are disputable.
First and above all, it is difficult to isolate the impact of accommodation at the destina-
tion from the impact of the forest environment on the tourist.
Secondly, it is very expensive to assure a big enough research sample with the same
protocol design; for example, for more than 500 participants, i.e., tourists. Nevertheless, we
can say that by measuring the impact of the forest on the tourist between two nights, i.e.,
after the first night of sleep and finishing one day before departure, the study minimized
the disturbance factors due to adaptation to the new environment.
The third limitation, in particular, is the scale time measurement and exposure time
to forest environment. SPANE, PHI I, and PHI II are based on the measurement of the
frequency of feelings during the past few weeks or one month. In the tourism industry, it is
difficult to find a tourist who would spend so much time in a destination at once. However,
such a measurement would not be in accordance with the real accommodation in situ.
Fourth, it is very difficult to provide a real destination environment for research
purposes longer than we did in our research. It is also very expensive, due to the high
season on the one hand and the real average occupancy of accommodation capacities
at the destination (2.5 days) on the other. The scale is appropriately stable only over a
2-month period [27]; meanwhile, in it could be sensitive to fluctuations in mood if we are
conducting a short-term measurement, such as in 2 days. The suggestions received from
the experts from the University of Ljubljana, Department of Psychology recommended an
observation period of 4 weeks for measurements, but one cannot afford this in tourism,
Forests 2022, 13, 1670
15 of 21
and the question of the usefulness of a longer period of accommodation also arises as the
average length of stay of a tourist at a destination is less than 3 days. That is why we
decided to accommodate tourists for two nights at the destination, as the average length of
tourist accommodation in the destination of Slovenia was 2.1 days [31]. Compared to other
studies, the time of exposure to the forest in some cases was very short, barely 15 min [25].
Therefore, to achieve greater relevance of the results, we recommend repeating the same
measurements in all seasons (spring, summer, autumn, and winter) with a longer period of
accommodation for the participants as tourists at the destination, if possible.
Fifth, a controlled study should be carried out on tourist participants in a resort outside
the forest area, with the same parameters.
Regarding the other parameters of the survey, we also note certain differences. Re-
search studies were conducted during different seasons, for example in winter (ibid).
Different techniques were used, such as Shinrnin-yoku [28], or recreation, such as walking
or cycling [19,29]. The exposures to the natural environment were on different green areas,
for example, in the forests, in city parks, at the coastal area, and elsewhere in nature [30].
Even though the tourists spent only 2 nights at the destination (which is the average
period of tourist accommodation in Slovenia) [31], and the entire experience of FT was
in one day, the results are very encouraging. The study measured the most frequently
observed physiological and psychological parameters. The results of the measurements
show that the signs of stress were greatly reduced in the period from Saturday morning to
Sunday morning. The average values of all five measured physiological parameters were
reduced after the two FT sessions: cortisol concentration in saliva, DHEA concentration
in saliva, systolic blood pressure, diastolic blood pressure, and heart rate. The reduction
in systolic blood pressure in our study was 3.8 mmHg, which is significant (p = 0.004),
but slightly less than in a study on 12 volunteers in Hungary [22], where the reduction in
systolic blood pressure was 6 mmHg. They did not measure cortisol, DHEA, diastolic blood
pressure, and heart rate. In our study we observed a nonsignificant reduction in cortisol
concentration in saliva (8 nmol/L before the forest therapies and 7.66 nmol/L after the
forest therapies, p > 0.05), which is different than in the study on 17 volunteers in Japan [6],
where the reduction was from 4.5 nmol/L to 3.3 nmol/L. According to our knowledge,
we were the first to measure the influence of FT on a stress marker DHEA, and we found
a significant reduction in this parameter in women and a strong nonsignificant trend of
reduction in men. This reduction is most likely mainly due to the impact of the two FT
sessions carried out on Saturday during the day. To minimize the influence of other factors,
both measurements (before and after therapy) were performed at the same time of day
(at 9 am). Since changing variables, such as the environment and vacation, are among the
most stressful events [22], (p. 103); [32], (p. 28), the tourists in this study arrived at the
Kranjska Gora location one day before the first measurement (Friday afternoon), so we
expect a change in factors, such as location, accommodation, and type of breakfast, affected
both measurements, but not the difference that occurred between Saturday and Sunday.
It is still possible that the signs of stress from Saturday to Sunday were reduced due to
factors other than FT. A study with two-day-conducted FT in Taiwan also notes that some
factors that were not considered in the research, such as temperature, humidity, negative
air ions, and illumination should be controlled in future studies in order to give a more
precise estimation regarding the effects of visiting a forest [28]. Other possible factors are
the forest climate, the ambience, carefree socialization, the comfort of the accommodations
at the destination and the cuisine, and changes in the environment, which could also have
a positive effect on the mental well-being of the tested tourists.
On the other hand, it is possible that FT had a beneficial effect on other physiological
parameters that were not measured in the study, or that the impact of FT on the measured
parameters may become more pronounced after a longer time.
The most used scale for assessing favorable and unfavorable emotions after exposure
to forest is the positive and negative affect scale (PANAS) [27], or the profile of mood states
(POMS) [25,30,31] scale. However, according to Diener (2009), it has some limitations,

Forests 2022, 13, 1670
16 of 21
which made us decide to use the recommended scale of positive and negative experiences
(SPANE). The SPANE was used for the measurement of the subjective feelings of well- and
ill-being [23,24]. A different approach to measurement, however, the Pemberton happiness
index (PHI I and PHI II) [21] of well-being, focuses on “experienced well-being,” which
assesses people’s current emotional states and feelings in real time, rather than relying
on individuals’ recall of feelings from past events/experiences. In addition to the POMS,
other studies also used other questionnaires to measure psychological states, such as the
restorative outcome scale (ROS), subjective vitality scale (SVS), Warwick–Edinburgh mental
well-being scale (WEMWBS) [33], psychological well-being scale (WB) [34], or restorative
outcome scale (ROS), and subjective vitality scale (SVS) [3]. Regardless of the type of
psychological questionnaire, the outcomes are questionable due to too short exposure to
the forest.
Found that, when evaluating well-being, it is more than the intensity of the emotion or
emotional state, important duration, i.e., how long a certain positive or negative experience
is. In addition, intensity is a more subjective concept, and the interpretation of intensity
can vary considerably from individual to individual [24]. Pemberton’s happiness index, on
the other hand, consists of two scales, one that is used to assess remembered well-being
and includes the domains of general, hedonic, eudaimonic, and social well-being, and the
second scale, experienced well-being, where positive and negative events that could be
related to experiencing well-being are listed. We interpret the results of both tests.
Numerous studies and systematic reviews found and published many various health and
well-being effects and benefits from FT as a specific type of exposure to nature [1–15,35]. At
the same time, they indicate a lack of high-quality studies with clear scientific evidence, for
example on the immune system, endocrine system, nervous system, etc. FT undoubtedly
benefits human health, but it is not yet completely clearly proven what this therapeutic or
healing effect is on individual disease indicators.
An observation period of 4 weeks would be desirable, but one cannot afford this in the
scope of tourism. A longer regular practice of FT can be achieved in the home environment.
5. Conclusions
This study examined physiological and psychological therapeutic effects of the FT on
tourists in the Kranjska Gora destination. The intention was to enlighten the usefulness
of FT in natural tourist resorts and destinations. Forest therapies were conducted with
the expert guidance of groups in accordance with the ANFT-specified and structured
animation. Participants were placed in a real environment at the Kranjska Gora destination
for two nights, so they became tourists. Testing the beneficial effect of FT in a real economic
environment, it is necessary to provide quality user experiences. According to Zahng
and Ye (2022, 13) “ . . . it is necessary to enrich FT service products and to integrate forest
therapies with tourism and health services and to consider leisure and tourism as a potential
way of developing and implementing FT”.
Research protocol design was followed and realized by presented tourists at the
research forest destination. The research was conducted from 18 to 20 June 2021. It
provided the clear scientific evidence of the health benefits for tourists, resulting from the
influence of the specific six (6)-step forest therapy tourism protocol at the destination of
Kranjska Gora, Slovenia.
The results of this research will contribute to the body of knowledge about FT and will
trigger innovative sustainable development solutions in the field of nontraditional tourist
use of forests. With the new scientific findings in the field of public health, the clarification
of FT human health benefits is also going to affect the development of forest therapeutic
tourism. Further research activities should be conducted by the tourism sector regarding
new markets and tourist segments based on this scientific evidence. This research will also
contribute to the popularization of FTT in Slovenia and encourage decision-makers and
stakeholders in the tourism sector to develop and expand the range of vigilant activities,
including FT, in local natural environments within destinations such as Kranjska Gora

Forests 2022, 13, 1670
17 of 21
who will recognize the potential of therapeutic forest tourism and the desire for a new
and innovative development direction. In this way, they will also make an important
contribution to the public health of the individual and society, and to the sustainable use of
natural resources. The presented forest therapy tourism research protocol at the destination
of Kranjska Gora can be used as guidance by planners and practitioners from all over to
increase and improve the effectiveness of nature-based interventions within forest envi-
ronments. By orienting towards the development of FT and well-being tourism, Slovenia
could achieve extreme advantages in comparison with other green outdoor destinations.
Author Contributions: Conceptualization, D.C. and S.K.; methodology, D.C.; software, D.C.; valida-
tion, D.C., C.A. and S.K.; formal analysis, D.C. and S.K.; investigation, D.C., C.A. and S.K.; resources,
D.C.; data curation, D.C.; writing—original draft preparation, D.C. and S.K.; writing—review and
editing, D.C.; visualization, D.C.; supervision, D.C.; project administration, D.C.; funding acquisition,
D.C. All authors have read and agreed to the published version of the manuscript.
Funding: This study was funded by the municipality of Kranjska Gora from Slovenia, an excellent,
lively mountain village, the organizer of the FIS World Cup matches, located in the valley between
the Julian Alps and Karavanke.
Data Availability Statement: Not applicable.
Acknowledgments: We are also grateful for the cooperation of all tourist organizations from the
municipality that collaboratively support FTT development. We would like to thank for all their
technical and administrative support, also.
Conflicts of Interest: The authors declare no conflict of interest. The funders had no role in the design
of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or
in the decision to publish the results.
Appendix A
Figure A1. Cont.

Forests 2022, 13, 1670
18 of 21
Figure A1. The Association of Nature and Forest Therapy (ANFT)—4 Certificate for Forest Therapy
guides, participating in this research.
Forests 2022, 13, 1670
Appendix B
19 of 21
Figure A2. Cont.
Forests 2022, 13, 1670
20 of 21
Figure A2. Permission to conduct research in the field of biochemistry from the Ministry of Health.
References
1. Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [CrossRef] [PubMed]
2. Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Shimizu, T.; Kawada, T.; Park, B.J.; Ohira, T.; et al.
Effect of phytoncide from trees on human natural killer cell function. Int. J. Immunopathol. Pharmacol. 2009, 22, 951–959. [CrossRef]
3. Bielinis, E.; Łukowski, A.; Omelan, A.; Boiko, S.; Takayama, N.; Grebner, D.L. The Effect of Recreation in a Snow-Covered Forest
Environment on the Psychological Wellbeing of Young Adults: Randomized Controlled Study. Forests 2019, 10, 827. [CrossRef]
4. Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a Forest Therapy Program and the Forest Environment on Female Workers’ Stress. Urban
For. Urban Green 2015, 14, 274–281. [CrossRef]
5. Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Physiological and
psychological effects of a forest therapy program on middle-aged females. Int. J. Environ. Res. Public Health 2015, 12, 15222–15232.
[CrossRef]
6. Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological
and psychological effects of forest therapy on middle-aged males with high blood pressure. Int. J. Environ. Res. Public Health 2015,
12, 2532–2542. [CrossRef]

Forests 2022, 13, 1670
21 of 21
7. Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The psychological and physical effects of forests on
human health: A systematic review of systematic reviews and meta-analyses. Int. J. Environ. Res. Public Health 2021, 18, 1770.
[CrossRef]
8. Hansen, M.M.; Jones, R.; Tocchini, K. Shinrinyoku (forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ.
Res. Public Health 2017, 14, 851. [CrossRef]
9. Doimo, I.; Masiero, M.; Gatto, P. Forest and well-being: Bridging medical and forest research for effective forest-based initiatives.
Forests 2020, 11, 791. [CrossRef]
10. Grilli, G.; Sacchelli, S. Health benefits derived from forest: A review. Int. J. Environ. Res. Public Health 2020, 17, 6125. [CrossRef]
11. Konu, H. Developing a forest-based wellbeing tourism product together with customers–An ethnographic approach. Tour. Manag.
2015, 49, 1–16. [CrossRef]
12. Ohe, Y.; Ikei, H.; Song, C.; Miyazaki, Y. Evaluating the relaxation effects of emerging forest-therapy tourism: A multidisciplinary
approach. Tour. Manag. 2017, 62, 322–334. [CrossRef]
13. Cvikl, D. Forest well-being tourist product: The case of shinrin-yoku, Obedska bara, Srbija. Tur. Posl. 2016, 18, 99–107. [CrossRef]
14. Cvikl, D. Forest Therapy and Well-Being Tourism Literature Review–With Assessment of Potential for Slovenia. Acad. Tur. 2022.
[CrossRef]
15. Cvikl, D. Factors of Forest Tourist Attractivness. Ph.D. Thesis, University of Primorska, Koper, Slovenia, 2022.
16. Chen, B.; Nakama, Y. Thirty years of forest tourism in China. J. For. Res. 2013, 18, 285–292. [CrossRef]
17. Nilsson, K.; Sangster, M.; Gallis, C.; Hartig, T.; De Vries, S.; Seeland, K.; Schipperijn, J. Forests, Trees and Human Health; Springer
Science & Business Media: Berlin/Heidelberg, Germany, 2011. [CrossRef]
18. Schuh, A.; Immich, G. Waldtherapie: Das Potenzial des Waldes für Ihre Gesundheit; Springer: Berlin/Heidelberg, Germany, 2019.
19. Looker, T.; Gregson, O. Premagajmo Stres: Kaj Lahko z Razumom Storimo Proti Stresu; Cankarjeva založba: Ljubljana, Slovenia, 1994.
20. Šmejc, P. Individualno Upravljanje Stresa. Ph.D. Thesis, University of Primorska, Koper, Slovenia, 2011.
21. Hervás, G.; Vázquez, C. Construction and validation of a measure of integrative well-being in seven languages: The Pemberton
Happiness Index. Health Qual. Life Outcomes 2013, 11, 66. [CrossRef]
22. Peterfalvi, A.; Meggyes, M.; Makszin, L.; Farkas, N.; Miko, E.; Miseta, A.; Szereday, L. Forest bathing always makes sense: Blood
pressure-lowering and immune system-balancing effects in late spring and winter in Central Europe. Int. J. Environ. Res. Public
Health 2021, 18, 2067. [CrossRef]
23. Diener, E.; Wirtz, D.; Biswas-Diener, R.; Tov, W.; Kim-Prieto, C.; Choi, D.W.; Oishi, S. New measures of well-being. In Assessing
Well-Being; Springer: Dordrecht, Switzerland, 2009; pp. 247–266. [CrossRef]
24. Jovanovic´, V. Beyond the PANAS: Incremental validity od the Scale of Positive and Negative Experience (SPANE) in relation to
well-being. Pers. Individ. Differ. 2015, 86, 487–491. [CrossRef]
25. Grabowska-Chenczke, O.; Wajchman-S´witalska, S.; Woz´niak, M. Psychological Well-Being and Nature Relatedness. Forests 2022,
13, 1048. [CrossRef]
26. Venter, Z.S.; Barton, D.N.; Gundersen, V.; Figari, H.; Nowell, M. Urban nature in a time of crisis: Recreational use of green space
increases during the COVID-19 outbreak in Oslo, Norway. Environ. Res. Lett. 2020, 15, 104075. [CrossRef]
27. Wajchman-S´witalska, S.; Grabowska-Chenczke, O.; Woz´niak, M.; Bałaj, B. Psychosocial Determinants of Recreational Activity
within Urban Green Spaces during the COVID-19 Pandemic in Poland. Forests 2022, 13, 1569. [CrossRef]
28. Chen, H.T.; Yu, C.P.; Lee, H.Y. The effects of forest bathing on stress recovery: Evidence from middle-aged females of Taiwan.
Forests 2018, 9, 403. [CrossRef]
29. Liu, Q.; Wang, X.; Liu, J.; An, C.; Liu, Y.; Fan, X.; Hu, Y. Physiological and Psychological Effects of Nature Experiences in Different
Forests on Young People. Forests 2021, 12, 1391. [CrossRef]
30. Annual Report of Slovenian Tourist Board for 2019. Available online: https://www.slovenia.info/uploads/dokumenti/tvs/2019
/turizem_v_stevilkah_2019.pdf (accessed on 18 August 2022).
31. Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in
forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 1–11. [CrossRef]
32. Shin, W.S.; Shin, C.S.; Yeoun, P.S.; Kim, J.J. The influence of interaction with forest on cognitive function. Scand. J. For. Res. 2011,
26, 595–598. [CrossRef]
33. Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS
scales. J. Personal. Soc. Psychol. 1988, 54, 1063. [CrossRef]
34. Kotte, D.; Li, Q.; Shin, W.S.; Michalsen, A. (Eds.) International Handbook of Forest Therapy; Cambridge Scholars Publishing:
Newcastle upon Tyne, UK, 2019.
35. Zhang, Z.; Ye, B. Forest Therapy in Germany, Japan, and China: Proposal, Development Status, and Future Prospects. Forests
2022, 13, 1289. [CrossRef]