
Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
RESEARCH
Open Access
A before and after comparison of the effects of
forest walking on the sleep of a community-
based sample of people with sleep complaints
Emi Morita1*, Makoto Imai2, Masako Okawa3, Tomiyasu Miyaura4 and Soichiro Miyazaki3
Abstract
Background: Sleep disturbance is a major health issue in Japan. This before-after study aimed to evaluate the
immediate effects of forest walking in a community-based population with sleep complaints.
Methods: Participants were 71 healthy volunteers (43 men and 28 women). Two-hour forest-walking sessions were
conducted on 8 different weekend days from September through December 2005. Sleep conditions were
compared between the nights before and after walking in a forest by self-administered questionnaire and
actigraphy data.
Results: Two hours of forest walking improved sleep characteristics; impacting actual sleep time, immobile
minutes, self-rated depth of sleep, and sleep quality. Mean actual sleep time estimated by actigraphy on the night
after forest walking was 419.8 ± 128.7 (S.D.) minutes whereas that the night before was 365.9 ± 89.4 minutes (n =
42). Forest walking in the afternoon improved actual sleep time and immobile minutes compared with forest
walking in the forenoon. Mean actual sleep times did not increase after forenoon walks (n = 26) (the night before
and after forenoon walks, 380.0 ± 99.6 and 385.6 ± 101.7 minutes, respectively), whereas afternoon walks (n = 16)
increased mean actual sleep times from 342.9 ± 66.2 to 475.4 ± 150.5 minutes. The trend of mean immobile
minutes was similar to the abovementioned trend of mean actual sleep times.
Conclusions: Forest walking improved nocturnal sleep conditions for individuals with sleep complaints, possibly as
a result of exercise and emotional improvement. Furthermore, extension of sleep duration was greater after an
afternoon walk compared to a forenoon walk. Further study of a forest-walking program in a randomized
controlled trial is warranted to clarify its effect on people with insomnia.
Keywords: forest walking (Shinrin-yoku), actual sleep time, actigraphy, St. Mary’s Hospital Sleep Questionnaire, cir-
cadian phase
Introduction
Sleep disturbance is a major health issue in Japan. In the
general population, a national survey in 1997 showed
that the prevalence of insomnia, including difficulty
initiating sleep, difficulty maintaining sleep, and early
morning awakening, was 21.4% [1]. Sleep disturbances
have been reported to be a risk factor for depression
and suicide [2-7]. Therefore to obtain good mental
health among the general population, it is important to
* Correspondence: emorita@med.nagoya-u.ac.jp
1Department of Preventive Medicine, Nagoya University Graduate School of
Medicine, 65 Tsurumai-Cho, Showa-Ku, Nagoya, 466-8550, Japan
Full list of author information is available at the end of the article
improve sleep among those who have sleep complaints,
rather than only among insomnia patients. Concrete and
practical methods to improve sleep that are applicable in
daily life are necessary. For example, habitual exercise
was associated with sleep condition in the general popu-
lation and exercise programs improved self-rated quality
of sleep in the elderly [1,8,9].
It is known that natural environments have various ben-
eficial effects on human health. European countries and
Japan have a long tradition of health resort programs to
optimize health conditions, with a natural environment
recognized as relevant to such facilities [10]. A green
environment has been reported to have beneficial effects
© 2011 Morita et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons
Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in
any medium, provided the original work is properly cited.

Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
Page 2 of 7
on human health. Mitchell and Popham [11] reported an
association between the amount of green spaces in resi-
dential areas and health status in a population study in the
UK. All-cause mortality and mortality from circulatory
diseases were lower in populations living in the greenest
areas. Ulrich [12] reported that surgical patients assigned
to rooms with windows looking out on natural scenery
with trees had shorter postoperative hospital stays,
received fewer negative evaluative comments in nurses’
notes, and took fewer potent analgesics than those in simi-
lar rooms with windows facing a brick wall. Moreover,
Kuo and Taylor [13] reported that green outdoor settings
appear to reduce attention-deficit/hyperactivity disorder
symptoms in children.
In Japan, forests cover 68.2% of the land area [14]. For-
est walking is a common recreational activity in Japan
because it is considered to promote both physical and
mental health by breathing in the substances released
from trees and through exercise and/or other healing fac-
tors associated with forest environments [15,16]. Indeed,
according to an opinion poll conducted in Japan in 2007,
36.2% of respondents had participated in forest walking
in the previous 1 year [17]. Recent studies revealed that
the physiological and psychological benefits of forest
walking are due mainly to stress reduction. Forest walk-
ing was shown to increase natural killer (NK) cell activity
and immunoglobulin levels [16]. Blood pressure, pulse
rate, and salivary cortisol concentration were lower in
people in a forest compared with a city area [18]. More-
over, Multiple Mood Scale-Short Form (MMS) [19,20]
scores of friendliness and wellbeing were higher, and
MMS score of depression and State-Trait Anxiety Inven-
tory-State Scale (STAI-S) [21] scores were lower on the
forest-walking day compared with the control day, espe-
cially in individuals who felt chronic mental stress [22].
Another study showed that walking in a forest is more
effective for decreasing blood glucose levels than other
activities, such as exercise on a cycle ergometer or tread-
mill or underwater exercise [15]. Forest walking and pre-
sence in a natural environment may improve sleep
because of their efficacy in stress reduction and the phy-
sical exercise involved. However, few studies have evalu-
ated the effect of forest walking on sleep.
The aims of this before-after study were to evaluate
the acute effects of forest walking for a community-
based population with sleep complaints and to compare
the effects between forenoon and afternoon forest walk-
ing, because the time of day when exercise is underta-
ken is one factor related to sleep response [23].
Method
Participants and Location
Participants were community-based adults who had self-
rated sleep complaint(s). They were recruited mainly
through personal communications, regional advertise-
ments, and the Internet. Eighty-three healthy volunteers
agreed to participate in this study. Twelve participants
who did not complete St. Mary’s Hospital Sleep Ques-
tionnaire (SMHSQ) twice and did not wear a wrist acti-
graph were excluded from the analysis. Therefore,
suitable data were available for 71 participants (M/F, 43/
28; aged in their 10 s, n = 3; 20 s, n = 7; 30 s, n = 13;
40 s, n = 6; 50 s, n = 17; 60 s, n = 17; 70 s, n = 5; no
data, n = 3). The mean ± SD score of the Pittsburgh
Sleep Quality Index (PSQI) was 6.4 ± 3.3 (n = 49). The
score for 28 participants (57.1% of those available) was
≥6, which is above the cutoff point. Forty-one partici-
pants took part in a forenoon session whereas 30 did so
in an afternoon session. Only one participant took a
sleeping drug the night after forest walking. Of the par-
ticipants, 49 individuals wore wrist actigraphs (see
below), 42 of whom were included in the analysis (M/F,
24/17; no data, n = 1; aged in their 10 s, n = 1; 20 s, n
= 5; 30 s, n = 8; 40 s, n = 4; 50 s, n = 9; 60 s, n = 10;
70 s, n = 4; no data, n = 1).
The study was carried out in the “Ryukoku Forest” of
Ryukoku University in Shiga Prefecture, located in the
western part of Honshu, the main island of Japan. The
elevation differential over the walking areas within the
forest was approximately 35 meters. The forest-walking
program was conducted on eight separate weekend days
from September to December 2005, and was held in
two daily sessions: a forenoon session between 10:00
and 12:00 and an afternoon session between 14:00 and
16:00. Participants voluntarily took part in either of the
two sessions. Each walking program lasted approxi-
mately 2 hours. We provided two types of program: a
2500-meter walking program and a 900-meter walk with
some light work such as felling small trees using a hand
saw within the forest program. The participants were
accompanied by 2-3 guides from Ryukoku University.
We obtained informed consent from all participants.
This study was approved by the ethics committee of
Shiga University of Medical Science.
Outcome Measures
The time schedule of the questionnaire survey is pre-
sented in Table 1. Sleep characteristics were compared
between the nights before and after walking in the forest
to evaluate the immediate effects of forest walking. All
participants were required to fill in the Japanese version
of SMHSQ on the night before and the night after forest
walking [24-27]. The questionnaire consisted of self-
rated sleep depth (1 = very light to 7 = deep), number
of awakenings (0 = not at all to 7 = more than six
times); sleep quality ("How well did you sleep last
night?” 1 = very badly to 6 = very well); alertness on
waking ("How clear-headed did you feel after getting up
Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
Page 3 of 7
Table 1 Time schedule of questionnaire
Day of forest walking
Before
After
Next day
SMHSQ
X
PSQI
X
STAI-S
X
X (in the morning)
X
Borg Scale
X
SMHSQ: St. Mary’s Hospital Sleep Questionnaire; PSQI: Pittsburgh Sleep Quality
Index; STAI-S: State-Trait Anxiety Inventory-State.
this morning?” 1 = very drowsy to 6 = very alert); satis-
faction with sleep (1 = very unsatisfied to 5 = comple-
tely satisfied); early morning awakening (yes/no); and
difficulty falling asleep (1 = none or very little to 4 =
extreme difficulty). The questionnaire for the night
before forest walking was collected at the forest walking
session whereas that for the night after forest walking
was collected by mail.
Among participants in the 8 survey days, those who
took part in 4 specific survey days were also requested
to wear a wrist actigraph (Actiwatch-64; Mini Mitter
Company, Inc, OR, USA) to estimate actual sleep time,
sleep efficiency, immobile minutes, and sleep latency in
addition to completing the above self-rated question-
naires [28-30]. Actigraphy measurement was carried out
for a period totaling 6 days, from 3 days before to 2
days after forest walking. The epoch length of the acti-
graphy was set at 2 minutes. Data were analyzed by
Actiware-Sleep version 5.0 (Mini Mitter).
Other Measurements
Besides socio-demographic characteristics, all partici-
pants were required to complete the Japanese version of
the Pittsburgh Sleep Quality Index (PSQI) questionnaire
related to self-rated sleep quality during the past 1
month [31-34]. The cutoff point of PSQI is 5.5. Higher
scores are associated with worse quality of sleep. Partici-
pants were also requested to provide information on
exercise habits (1 = rarely to 5 = > 20 minutes every
day). We defined habitual exercise as exercising for 20
minutes more than once a week, but without taking into
account the intensity of the exercise [35,36].
STAI-S (score range, 20-80) evaluations were per-
formed just before and immediately after 2 hours of for-
est walking to investigate the effects of forest walking
on perceived psychological states [21,37]. Participants
also completed the Borg scale to examine perceived
exertion immediately after forest walking [38].
Statistical Analysis
Participants who completed SMHSQ both the night
before and the night after forest walking or who wore a
wrist actigraph were included in the analysis. Although
actigraphy was carried out for a total of 6 nights, the
night just before and that immediately after forest walk-
ing were compared by paired-Student’s t test. SMHSQ
item scores from the nights before and after forest walk-
ing were also compared by paired Wilcoxon signed-rank
test, or McNemar’s test. In addition, STAI-S scores
before and those immediately after 2 hours of forest
walking were compared by paired-Student’s t test.
To compare the effects on sleep between forenoon
and afternoon sessions, repeated measures analysis of
variance (ANOVA) was conducted using the measure-
ment points (repeated factor: the night before forest
walking vs. that after) × the forest walking session
(between-subject factor: forenoon vs. afternoon). To
explore other relevant factors related to the immediate
measurable effects on sleep after forest walking, repeated
measures analysis of variance (ANOVA) was conducted
using the measurement points of outcome items
observed as significant in the above analysis (repeated
factor: the night before forest walking vs. that after) × a
between-subject factor such as sex, age (< 60/≥60 years),
exercise habits, daily disturbances of sleep (PSQI, < 5.5/
≥5.5), score of STAI-S decreased by forest walking
(below/above average), Borg scale after forest walking
(below/above average), forest walking on Saturday vs.
Sunday, and forest walking alone vs. forest walking with
light work.
Additional repeated measures ANOVA were con-
ducted. The repeated factor was one of the relevant
sleep parameters identified in above analysis (sleep
depth, sleep quality of SMHSQ, and actual sleep time
and immobile time by actigraphy), and between-subject
factors were the decrease in score of STAI-S by forest
walking (below/above average) and forest walking ses-
sion (forenoon vs. afternoon). SPSS 14.0J for Windows
and IBM SPSS Statistics 19 were used for statistical ana-
lysis; significance level was set at 5%.
Results
Comparison of sleep between the nights before and after
forest walking
The results of self-rated sleep conditions measured by
SMHSQ comparing the night before to that after forest
walking are shown in Table 2. The scores of self-rated
depth of sleep and sleep quality were significantly
improved the night after forest walking. The results of
objective sleep analysis by actigraphy are shown in
Table 2. Actual sleep time and immobile minutes the
night after forest walking were significantly longer than
the night before. Mean actual sleep time the night
before was 365.9 ± 89.4 (S.D.) minutes whereas the
night after was 419.8 ± 128.7 minutes. Mean immobile
time the night before forest walking was 356.3 ± 89.1
Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
Page 4 of 7
Table 2 Sleep characteristics for the night before and the night after forest walking
n
Actual sleep time (min)
Actual sleep (%)
Sleep latency (min)
Immobile time (min
Sleep start time (median)
Sleep end time (median)
St. Mary’s Hospital Sleep Questionnaire
Self-rated depth of sleep (score)
Number of awakenings (times)
Sleep quality (score)
Alertness on waking (score)
Satisfaction with sleep (score)
Early morning awakening (n, % yes)
Difficultly falling asleep (score)
Night before Night after
Statistical test Comment
forest walking forest walking
42
365.9 ± 89.4
419.8 ± 128.7
p = 0.02a
42
86.9 ± 7.4
88.0 ± 6.9
p = 0.4a
42
20.1 ± 32.7
10.4 ± 9.7
p = 0.07a
42
356.3 ± 89.1
410.2 ± 127.7
p = 0.02a
42
23:48
23:46
42
6:58
7:18
64
4.7 ± 1.4
66
1.48 ± 1.24
63
4.0 ± 1.1
62
3.4 ± 1.2
63
3.3 ± 1.0
60
10, 16.7%
64
1.3 ± 0.5
5.1 ± 1.5
1.45 ± 1.34
4.3 ± 1.2
3.6 ± 1.3
3.4 ± 1.1
8, 13.3%
1.2 ± 0.5
p = 0.03b 1: Very light
7: Deep
p = 0.7b 0: Not at all
7: More than six times
p = 0.04b 1: Very badly
6: Very well
p = 0.054b 1: Very drowsy 6: Very alert
p = 0.3b 1: Very unsatisfied 5: Completely satisfied
p = 0.7c 1: No
2: Yes
p = 0.3b 1: None or very little 4: Extreme difficulty
Mean ± SD, a: Paired-Student’s t-test, b: Paired Wilcoxon signed-rank test, c: McNemar’s test.
minutes whereas the night after was 410.2 ± 127.7 min-
utes. Median sleep start time did not change (23:48 vs.
23:46; n = 42), whereas median sleep end time delayed
approximately 20 minutes the night after forest walking
compared with the night before (6:58 vs. 7:18). Among
participants with actigraphy, 38.5% in the forenoon ses-
sion (10 of 26) reported in their sleep diary that they
had a nap(s) after forest walking whereas 28.6% of parti-
cipants (4 of 14) in the afternoon session reported
napping.
Psychological effects of 2-hours forest walking based on
changing STAI-S scores just before and immediately after
forest walking
The psychological effects of forest walks were based on
comparison of STAI-S given just before and immedi-
ately after a 2-hour walk. The STAI-S scores signifi-
cantly decreased with 2 hours of forest walking, from
37.2 ± 9.3 to 30.2 ± 6.1 (Student’s paired-t test: p <
0.001; n = 47). Mean Borg scale score immediately after
forest walking was 11.6 ± 2.3. Given that 11 points is
considered fairly light, the intensity of the forest walking
in this study was considered light exercise [38].
Comparison of effects between forenoon and afternoon
participation
The sleep conditions estimated by actigraph and
SMHSQ between forenoon and afternoon sessions are
presented in Table 3. Regarding objective sleep para-
meters measured by actigraphy, the interactions between
measurement points (the night before forest walking vs.
the night after) and the forest walking session (forenoon
vs. afternoon) on actual sleep time (p = 0.005) and
immobile minutes (p = 0.006) were significant. Mean
actual sleep times and mean immobile minutes did not
increase after forenoon walks whereas they increased
after afternoon walks.
Regarding self-rated sleep by SMHSQ, no significant
interaction was observed for any of the items. Since the
main effects of time (the night before forest walking vs.
the night after) were significant in self-rated depth of
sleep (p = 0.03) and sleep quality (p = 0.04), these two
items were improved regardless of timing of the session
(forenoon or afternoon). The self-rated depth of sleep
score increased after forest walking in both session
groups (4.5 ± 1.4 to 4.9 ± 1.4 in the forenoon session;
4.9 ± 1.3 to 5.2 ± 1.6 in the afternoon session). The
sleep quality score was also similarly increased regard-
less of the timing of the session (3.9 ± 1.1 to 4.2 ± 1.2
in the forenoon session; 4.1 ± 1.0 to 4.3 ± 1.2 in the
afternoon session).
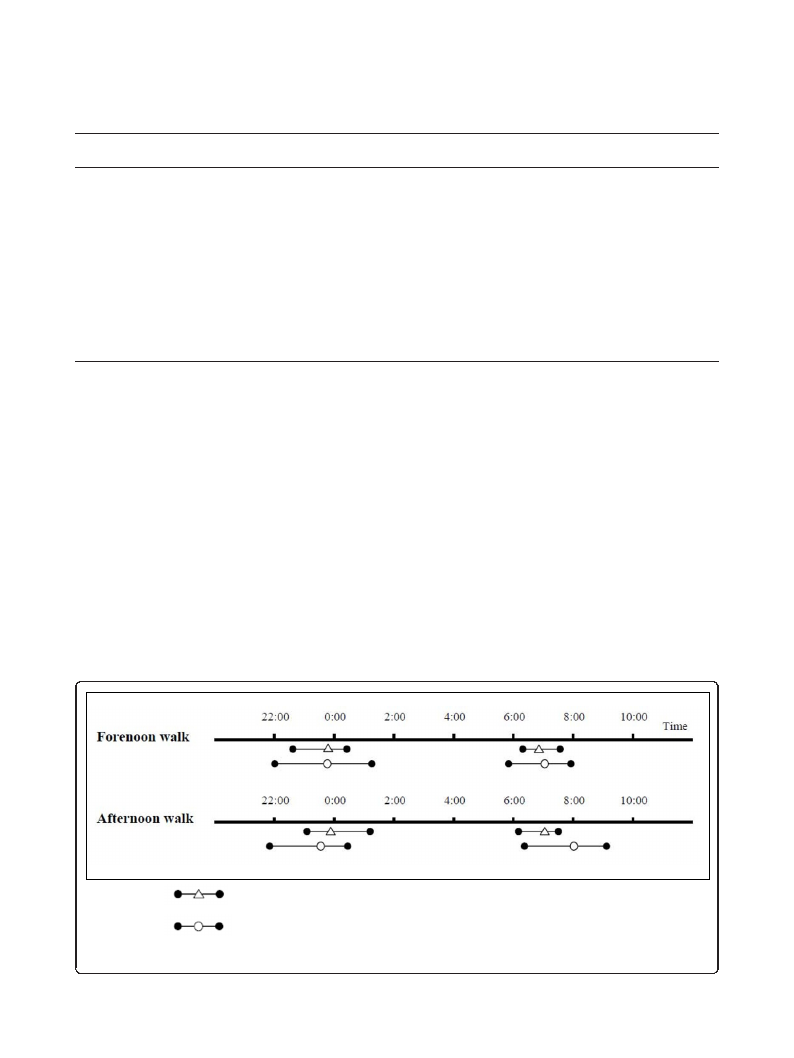
As presented in Figure 1, median sleep start time was
less changed the night after forest walking compared
with the night before for participants walking in the
forenoon (23:48 to 23:46; n = 26) and participants walk-
ing in the afternoon (23:54 to 23:34, n = 16). Median
sleep end time was delayed the night after forest walking
compared with the night before for participants walking
in the afternoon (7:04 to 8:01) whereas there was less
extension for forenoon participants (6:52 to 7:04).
Other relevant factors related to sleep improvement
Exploratory analysis revealed that a relevant factor
related to sleep is decreased STAI-S scores (below or
above average decrease) due to forest walking on sleep
depth (interaction between decreased STAI-S scores and
sleep depth, p = 0.002). In subgroups that had a greater
than average decrease in STAI-S score after forest
Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
Page 5 of 7
Table 3 Comparison of effects on forenoon and afternoon walking
Forenoon session
Afternoon session
n
Beforea
Afterb
n
Beforea
Actual sleep time (min)
26
380.0 ± 99.6
385.6 ± 101.7
16
342.9 ± 66.2
Actual sleep (%)
26
88.8 ± 5.1
88.9 ± 5.5
16
83.9 ± 9.6
Sleep latency (min)
26
22.8 ± 40.2
11.1 ± 10.9
16
15.6 ± 14.3
Immobile time (min)
26
372.2 ± 95.7
377.5 ± 98.2
16 330.6 ± 72.8
St. Mary’s Hospital Sleep Questionnaire
Self-rated depth of sleep (score)
35
4.5 ± 1.4
4.9 ± 1.4
29
4.9 ± 1.3
Number of awakenings (times)
37
1.46 ± 1.26
1.49 ± 1.22
29
1.52 ± 1.24
Sleep quality (score)
34
3.9 ± 1.1
4.2 ± 1.2
29
4.1 ± 1.0
Alertness on waking (score)
34
3.4 ± 1.2
3.6 ± 1.4
28
3.4 ± 1.2
Satisfaction with sleep (score)
34
3.2 ± 1.0
3.2 ± 1.1
29
3.3 ± 1.1
Early morning awakening (n, % yes) 34
5, 14.7%
5, 14.7%
26
5, 19.2%
Difficultly falling asleep (score)
35
1.2 ± 0.5
1.2 ± 0.5
29
1.3 ± 0.6
Mean ± SD, a: night before forest walking, b: night after forest walking, c: repeated analysis of variance.
Afterb
Interactionc
475.4 ± 150.5
0.005
86.6 ± 8.7
0.28
9.4 ± 7.3
0.61
463.4 ± 153.6
0.006
5.2 ± 1.6
0.57
1.41 ± 1.50
0.63
4.3 ± 1.2
0.87
3.8 ± 1.1
0.64
3.6 ± 0.9
0.30
3, 11.5%
1.2 ± 0.5
0.23
walking, the self-rated sleep depth score increased. By
contrast, the score did not change in subgroups with a
smaller than average decrease in STAI-S score after for-
est walking. Other factors were not relevant. Even if the
model of repeated-measures ANOVA with both score
change of STAI-S due to forest walking and forest walk-
ing session (forenoon and afternoon), the interaction
between the score change of STAI-S by forest walking
and sleep depth was also significant (p = 0.002).
Discussion
This study suggests that 2 hours forest walking signifi-
cantly lengthened mean actual sleep time and mean
immobile time estimated by actigraphy and that sleep
depth and sleep quality were improved, as evaluated by
SMHSQ. In addition, some participants had a nap(s) after
forest walking. Forest walking may contribute to improve-
ment of subsequent sleep for individuals with sleep com-
plaints. Exercise and emotional improvement initiated by
walking in forested areas may bring both increased sleep-
ing hours and improved subjective sleep quality.
Regarding objective sleep parameters, a previous
review suggested that exercise increased total sleep time
(TST) but did not significantly affect sleep onset latency
(SOL) [39]; our results come close to supporting this.
Recent studies reported that sleep emerges locally and is
regulated in a use-dependent (homeostatic) manner
[40,41]. The study showed that arm immobilization
locally decreased slow wave activity in subsequent sleep;
slow wave activity is thought to reflect sleep need [41].
Exercise during the prior wake period therefore might
induce sleep.
Median and interquartile range in the night before forest walking
Median and interquartile range in the night after forest walking
Figure 1 Sleep start time (median and interquartile range) and sleep end time (median and interquartile range) the nights before and
after forest walking for forenoon and afternoon walk subgroups.

Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
Page 6 of 7
Regarding emotional effects, this study suggests that 2
hours’ forest walking significantly improved anxiety as
measured by STAI-S. Furthermore, self-rated sleep
depth for individuals whose STAI-S scores decreased by
more than the average was much improved versus in
individuals who had STAI-S scores decreased by less
than the average–even when adjusted by forest walking
session, which was a relevant factor for sleep improve-
ment. From these results, it appears that improvement
of self-rated sleep depth may depend on not only exer-
cise but also improvement of psychological factors.
Since forest walking, which does not require specific
techniques, is a widely available activity, walking in
forested areas may be a practical method to improve
sleep that is easily applicable in daily life.
Our study suggests that afternoon forest walks had a
greater effect on actual sleep time and immobile min-
utes than those taken in the forenoon. The time of day
when exercise is undertaken is one factor related to the
subsequent sleep response [23,39]. Youngstedt et al. [39]
reported that SOL and wakefulness after sleep onset
(WASO) were influenced by the time of day when exer-
cise was completed, whereas TST was not influenced by
the time of day. However, this study revealed that forest
walking in the afternoon much improved actual sleep
time and immobile minutes but not SOL compared with
forest walking in the forenoon.
According to a two-process model [42,43] sleep and
waking are regulated by circadian rhythms (Process C)
and homeostasis (Process S). To examine why the after-
noon session causes improvements in actual sleep time
and immobile minutes, the core body temperature
should be measured to determine the change of circa-
dian phase (Process C) [42]. Since the measurement was
not available in this study, we cannot conclude why the
afternoon session caused improvements in actual sleep
time and immobile minutes. However, one possible rea-
son that the afternoon session brought improvements
could be by homeostatic mechanism recovery after exer-
cise (Process S). Exercise may amplify core body tem-
perature. A steep decline of core body temperature
before nocturnal sleep was reported to induce sleep
[44]. The afternoon session, with a shorter interval
between the end of walking and the onset of nocturnal
sleep compared with the forenoon session, might be
profitable for sleep improvements. On the other hand,
because both forenoon and afternoon sessions are con-
ducted in the daytime, they might not affect the circa-
dian phase (Process C), as shown by the sleep start
times of the forenoon and afternoon session participants
which did not change on the nights before and after for-
est walking. Furthermore, the possibility still remains
that the higher percentage of participants taking a nap
(s) after forest walking in a forenoon session compared
with an afternoon session was related to an apparent
extension of nocturnal sleep duration in the participants
in the afternoon sessions.
Intensity of exercise is also a factor related to subse-
quent sleep [23]. The intensity of forest walking in this
study was considered light exercise on the Borg scale
because the study was conducted in a forested area with
few steep mountain paths. Since this study suggests that
forest walking improved some sleep conditions, the
intensity of exercise can be seen as appropriate.
This study has some limitations. First, there was no
control group for walking in non-forested areas adjusted
by exercise strength and light intensity. Therefore we
cannot claim with certainty whether immediate
improvements in the characteristics of sleep were
brought on by walking only or by walking specifically
carried out in forested areas. However, a previous study
showed that STAI-S score was lower on a forest-walk-
ing day compared with another day with exercise in
non-forested areas [22]. Furthermore, the present study
suggests that improvement of anxiety measured by
STAI-S was associated with self-rated sleep depth, even
after adjusting for the timing of forest walking (fore-
noon vs. afternoon). From these two results, walking in
forested areas, where emotional effects would be
expected, might produce much improvement of sleep
compared with walking in non-forested areas. Second,
we evaluated only the immediately discernable effects of
sleep.
The conclusions of this study are that 2 hours forest
walking lengthened actual sleeping hours and immobile
minutes and that it improved self-rated depth of sleep
and sleep quality for individuals who had sleep com-
plaints. The self-rated depth of sleep depended on emo-
tional improvements. Forest walking in the afternoon
prolonged actual sleeping hours and immobile minutes.
Further studies using a randomized controlled trial
design need to be carried out to evaluate whether a ser-
ies of forest walks improves slight insomnia and slight
sleep complaints. Such a study should reveal what fac-
tors in forest walking are responsible for improving
sleep complaints.
Acknowledgements
The study was supported by the Ministry of Economy,
Trade and Industry of Japan.
Author details
1Department of Preventive Medicine, Nagoya University Graduate School of
Medicine, 65 Tsurumai-Cho, Showa-Ku, Nagoya, 466-8550, Japan.
2Department of Psychiatry, Shiga University of Medical Science, Seta
Tsukinowa-cho, Otsu, Shiga 520-2192, Japan. 3Department of Sleep Medicine,
Shiga University of Medical Science, Seta Tsukinowa-cho, Otsu, Shiga, 520-
2192, Japan. 4Faculty of Science and Technology, Ryukoku University, 1-5
Yokotani, Seta Oe-cho, Otsu, Shiga, 520-2194, Japan.
Morita et al. BioPsychoSocial Medicine 2011, 5:13
http://www.bpsmedicine.com/content/5/1/13
Page 7 of 7
Authors’ contributions
SM and TM deigned the study and collected the data. EM analyzed the data
and MI provided advice on the data analysis. EM, MI, and MO interpreted
the data. EM drafted the manuscript. MI, MO, and SM participated in revision
of the manuscript. All authors have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Received: 2 June 2011 Accepted: 14 October 2011
Published: 14 October 2011
References
1. Kim K, Uchiyama M, Okawa M, Liu X, Ogihara R: An epidemiological study
of insomnia among the Japanese general population. Sleep 2000, 23:41-7.
2. Ford DE, Kamerow DB: Epidemiologic study of sleep disturbances and
psychiatric disorders. An opportunity for prevention? JAMA 1989,
262:1479-84.
3. Livingston G, Blizard B, Mann A: Does sleep disturbance predict
depression in elderly people? A study in inner London. Br J Gen Pract
1993, 43:445-8.
4. Breslau N, Roth T, Rosenthal L, Andreski P: Sleep disturbance and
psychiatric disorders: a longitudinal epidemiological study of young
adults. Biol Psychiatry 1996, 39:411-8.
5. Chang PP, Ford DE, Mead LA, Cooper-Patrick L, Klag MJ: Insomnia in
young men and subsequent depression. The Johns Hopkins Precursors
Study. Am J Epidemiol 1997, 146:105-14.
6. Roberts RE, Shema SJ, Kaplan GA, Strawbridge WJ: Sleep complaints and
depression in an aging cohort: A prospective perspective. Am J Psychiatry
2000, 157:81-8.
7. Fujino Y, Mizoue T, Tokui N, Yoshimura T: Prospective cohort study of
stress, life satisfaction, self-rated health, insomnia, and suicide death in
Japan. Suicide Life. Threat Behav 2005, 35:227-37.
8. King AC, Oman RF, Brassington GS, Bliwise DL, Haskell WL: Moderate-
intensity exercise and self-rated quality of sleep in older adults. A
randomized controlled trial. JAMA 1997, 277(1):32-7.
9. Sherrill DL, Kotchou K, Quan SF: Association of physical activity and
human sleep disorders. Arch Intern Med 1998, 158:1894-8.
10. Morita E, Weigl M, Schuh A, Stucki G: Identification of relevant ICF
categories for indication, intervention planning and evaluation of health
resort programs: a Delphi exercise. Int J Biometeorol 2006, 50:183-91.
11. Mitchell R, Popham F: Effect of exposure to natural environment on
health inequalities: an observational population study. Lancet 2008,
372:1655-60.
12. Ulrich RS: View through a window may influence recovery from surgery.
Science 1984, 224:420-1.
13. Kuo FE, Taylor AF: A potential natural treatment for attention-deficit/
hyperactivity disorder: evidence from a national study. Am J Public Health
2004, 94:1580-6.
14. Food and Agriculture Organization of the United Nations: State of the
World’s Forests, 2007. Rome: Food and Agriculture Organization of the
United Nations; 2007, 111.
15. Ohtsuka Y, Yabunaka N, Takayama S: Shinrin-yoku (forest-air bathing and
walking) effectively decreases blood glucose levels in diabetic patients.
Int J Biometeorol 1998, 41:125-7.
16. Ohira H, Takagi S, Masui K, Oishi M, Obata A: Effects on shinrin-yoku
(forest-air bathing and walking) on mental and physical health. Bull Tokai
Women Univ 1999, 19:217-232, (in Japanse).
17. Cabinet Office of Government of Japan: The opinion poll on forests and
life 2007. Tokyo: Cabinet Office of Government of Japan; 2007, (in
Japanese).
18. Tsunetsugu Y, Park BJ, Ishii H, Hirano H, Kagawa T, Miyazaki Y: Physiological
effects of Shinrin-yoku (taking in the atmosphere of the forest) in an
old-growth broadleaf forest in Yamagata Prefecture, Japan. J Physiol
Anthropol 2007, 26:135-42.
19. Terasaki M, Kishimoto Y, Koga A: Construction of a multiple mood scale.
Shinrigaku Kenkyu 1992, 62:350-6, (in Japanese).
20. Terasaki M, Koga A, Kishimoto Y: Construction of the multiple mood scale-
short form. Proceedings of the 55th annual conversation of Japanese
psychological association 1991, (in Japanese).
21. Spielberger CD, Gorsuch RL, Lushene RE: Manual for the State-Trait
Anxiety Inventory (self-evaluation questionnaire). Palo Alto, CA:
Consulting Psychologists Press; 1970.
22. Morita E, Fukuda S, Nagano J, Hamajima N, Yamamoto H, Iwai Y,
Nakashima T, Ohira H, Shirakawa T: Psychological effects of forest
environments on healthy adults: Shinrin-yoku (forest-air bathing,
walking) as a possible method of stress reduction. Public Health 2007,
121:54-63.
23. Driver HS, Taylor SR: Exercise and sleep. Sleep Med Rev 2000, 4:387-402.
24. Ellis BW, Johns MW, Lancaster R, Raptopoulos P, Angelopoulos N, Priest RG:
The St. Mary’s Hospital sleep questionnaire: a study of reliability. Sleep
1981, 4:93-7.
25. Leigh TJ, Bird HA, Hindmarch I, Constable PD, Wright V: Factor analysis of
the St. Mary’s Hospital Sleep Questionnaire. Sleep 1988, 11:448-53.
26. Uchiyama M, Ohta K, Okawa M: Evaluation of sleep condition and sleep
disturbance.Edited by: Ohta T, Okawa M. Sleep disorder, Encycropedia of
Clinical Psychiary. Tokyo: Nakayama Shoten; 1999:489-98, (in Japanese).
27. Oyefeso A, Sedgwick P, Ghodse H: Subjective sleep-wake parameters in
treatment-seeking opiate addicts. Drug Alcohol Depend 1997, 48:9-16.
28. Sadeh A, Hauri PJ, Kripke DF, Lavie P: The role of actigraphy in the
evaluation of sleep disorders. Sleep 1995, 18:288-302.
29. van Hilten JJ, Braat EA, van der Velde EA, Middelkoop HA, Kerkhof GA,
Kamphuisen HA: Ambulatory activity monitoring during sleep: an
evaluation of internight and intrasubject variability in healthy persons
aged 50-98 years. Sleep 1993, 16:146-50.
30. Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC: Automatic sleep/wake
identification from wrist activity. Sleep 1992, 15:461-9.
31. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ: The Pittsburgh
Sleep Quality Index: a new instrument for psychiatric practice and
research. Psychiatry Res 1989, 28:193-213.
32. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F: Test-retest
reliability and validity of the Pittsburgh Sleep Quality Index in primary
insomnia. J Psychosom Res 2002, 53:737-40.
33. Doi Y, Minowa M, Uchiyama M, Okawa M, Kim K, Shibui K, Kamei Y:
Psychometric assessment of subjective sleep quality using the Japanese
version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric
disordered and control subjects. Psychiatry Res 2000, 97:165-72.
34. Doi Y, Minowa M, Utiyama S, Okawa M: Development of the Japanese
version of the Pittsburgh Sleep Quality Index. Japanese Journal of
Psychiatry Treatment 1998, 13:755-763, (in Japanese).
35. Belloc NB, Breslow L: Relationship of physical health status and health
practices. Prev Med 1972, 1:409-21.
36. Belloc NB: Relationship of health practices and mortality. Prev Med 1973,
2:67-81.
37. Shimizu H, Imaei K: Construction of a Japanese version of the State-Trait
Anxiety Inventory. Jap J Educ Psychol 1981, 29:348-53, (in Japanese).
38. Borg GA: Psychophysical bases of perceived exertion. Med Sci Sports Exerc
1982, 14:377-381.
39. Youngstedt SD, O’Connor PJ, Dishman RK: The effects of acute exercise on
sleep: a quantitative synthesis. Sleep 1997, 20:203-14.
40. Vassalli A, Dijk DJ: Sleep function: current questions and new approaches.
Eur J Neurosci 2009, 29:1830-41.
41. Huber R, Ghilardi MF, Massimini M, Ferrarelli F, Riedner BA, Peterson MJ,
Tononi G: Arm immobilization causes cortical plastic changes and locally
decreases sleep slow wave activity. Nat Neurosci 2006, 9:1169-76.
42. Borbély AA: A two process model of sleep regulation. Hum Neurobiol
1982, 1:195-204.
43. Daan S, Beersma DG, Borbély AA: Timing of human sleep: recovery
process gated by a circadian pacemaker. Am J Physiol 1984, 246(2 Pt 2):
R161-83.
44. Kräuchi K, Wirz-Justice A: Circadian clues to sleep onset mechanisms.
Neuropsychopharmacology 2001, 25(5 Suppl):S92-6.
doi:10.1186/1751-0759-5-13
Cite this article as: Morita et al.: A before and after comparison of the
effects of forest walking on the sleep of a community-based sample of
people with sleep complaints. BioPsychoSocial Medicine 2011 5:13.