
International Journal of
Environmental Research
and Public Health
Study Protocol
Simulated Forest Immersion Therapy: Methods Development
Amy Miner Ross * and Reo Jane Francesca Jones
School of Nursing, Oregon Health and Science University (OHSU), 3455 S. W. US Veterans Hospital Road,
Portland, OR 97239, USA; jonesre@ohsu.edu
* Correspondence: rossam@ohsu.edu; Tel.: +1-503-494-2123
Citation: Ross, A.M.; Jones, R.J.F.
Simulated Forest Immersion Therapy:
Methods Development. Int. J.
Environ. Res. Public Health 2022, 19,
5373. https://doi.org/10.3390/
ijerph19095373
Abstract: Shinrin-yoku, forest bathing, may provide relief from chronic and breakthrough pain in
patients with axial spondyloarthritis and improve immune function through increasing NK cell
numbers and activity and their downstream effectors, perforin and granulysin, after chemo- or
radiation therapy in breast and prostate cancer patients. The aim of this paper is to describe the study
protocol for a simulated forest immersion therapy using virtual reality and atomized phytoncides,
volatile organic compounds found in forested areas designed to effect positive change for these two
patient populations. The setting, including the room set up and samples with inclusion/exclusion
specific to this type of intervention, is outlined. Measures and calibration procedures pertinent to
determining the feasibility of simulated forest immersion therapy are presented and include: ambient
and surface room temperatures and relative humidity in real time, ambient ultrafine particulate
matter, ambient droplet measurement that coincides with volatile organic compounds, specific
phytoncides, and virtual reality and atomization of phytoncide set up. Particular lessons learned
while training and setting up the equipment are presented. Simulated forest immersion therapy is
possible with attention to detail during this early phase when development of methods, equipment
testing, and feasibility in deploying the intervention become operational. The expected outcome
of the development of the methods for this study is the creation of a standardized approach to
simulating forest therapy in a controlled laboratory space.
Keywords: shinrin-yoku; virtual reality; phytoncides; exposure science methods; NK cells; Visual
Analog Scale; DASS; BASDAI
Academic Editors: Amber L.
Vermeesch, Andrew Lafrenz and
Chloé Littzen
Received: 28 February 2022
Accepted: 27 April 2022
Published: 28 April 2022
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2022 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
1. Introduction
Shinrin-yoku, roughly translated as forest bathing, is the traditional Japanese practice
of immersing oneself in nature by mindfully using our senses, such as sight and smell [1,2].
Shinrin-yoku practices range from sitting quietly and enjoying the forest to walking or hik-
ing through forested areas [3]. The key to shinrin-yoku is connecting with the atmosphere
of the forest, taking in forest aerosols, volatile organic compounds known phytoncides [4].
Phytoncides are inhaled airborne particles that trees naturally emit during different stages
of development [5–9].
In 1982, the Japanese Ministry of Agriculture, Forestry and Fisheries began researching
the health benefits of shinrin-yoku [2]. There are several therapeutic effects of shinrin-
yoku in the context of depression, including improving immune system function, such as
decreased pro-inflammatory cytokine activity and increased in anti-inflammatory cells,
decreased depressive symptoms, stress, and anxiety, improved mental relaxation and at-
tentional focus, and increased feelings of awe, gratitude, and selflessness [4,9–16]. The
benefit of forested greenspaces for human psychology and physiology is a reduction in
stress [14,17], which in turn positively impacts mood [18] and further reduces inflam-
mation [19]. In the context of normal male subjects, after both shinrin-yoku forest im-
mersion and hotel/sleep-based phytoncide humidification with α-pinene, β-pinene, and
d-limonene, the following immune system improvements were found: natural killer T-cell
numbers and activity increased, as did perforin and granulysin [6,20,21].
Int. J. Environ. Res. Public Health 2022, 19, 5373. https://doi.org/10.3390/ijerph19095373
https://www.mdpi.com/journal/ijerph

Int. J. Environ. Res. Public Health 2022, 19, 5373
2 of 17
In 2017, a research agenda for nature contact and health was published with several
research domains, including the mechanistic biomedical studies domain (1.0) for future
research development [17]. We developed a simulated forest immersion therapy (SFIT)
that includes both forest aerosols and virtual reality based on this research agenda. We are
interested in psychological and physiological variables that suit our differing populations
of interest (i.e., axial spondyloarthritis patients with chronic or breakthrough pain or
breast and prostate cancer patients who have undergone chemo- or radiation therapy and
have NK cell depletion), and these align with the mechanistic biomedical domain [17].
Specifically, our research objectives are to elucidate 1.1: to what extent stress reduction
mediates observed health benefits of nature contact; 1.1b: which natural elements are most
associated with stress reduction; 1.2: to what extent improved immune function mediates
observed health benefits of nature contact; 1.2b which natural elements are most associated
with improved immune function; and 1.2c which markers of immune function are the most
useful for studying this effect [17]. If there are health effects of forest immersion, then could
the same health benefits be achieved with simulated forest immersion as a way of providing
therapy to patients not able to exercise or move in outdoor forests or greenspaces due to
debility or frailty from chronic illness (i.e., chronic and breakthrough pain) or acute illness
(i.e., recovery of immune system function after chemo- or radiation therapy in cancer)?
1.1. Significance
An estimated 1,806,590 new cases of cancer will be diagnosed in the United States
each year, of which 281,550 will be breast cancer and an estimated 248,530 will be prostate
cancer [22]. Additionally, up to 1% of the population of the United States, an estimated
2.7 million people, may have axial spondyloarthritis [23], and 50% of them suffer from
chronic widespread pain [24,25] and breakthrough pain after standard treatment in approx-
imately 60% of people [26]. Using complementary interventions to improve outcomes in
patients who are seriously ill is paramount to extending healthcare to vulnerable popu-
lations. We hope to accelerate the translation of findings for healthy individuals for the
implementation of a novel minimally invasive immune therapy for cancer patients with
solid tumors where NK cells are depleted, both in number and activity [27,28], and to deter-
mine clinically meaningful protocols for the management of pain, and comorbid symptoms
of pain, in patients with axial spondyloarthritis with chronic and breakthrough pain.
Forest bathing, virtual reality (VR), the use of phytoncides, and their separate or
combined effects constitute a new research avenue. It is intriguing to explore the effects
of nature-based interventions on chronic and breakthrough pain in patients with axial
spondyloarthritis, as well as the effects on the immune system, and how we might harness
them to benefit acutely ill patients who are immunocompromised.
1.2. Background
1.2.1. Psychological Pathways of Interest
Contemporary theories, such as Kaplan’s Attention Restoration Theory [29,30], Ul-
rich’s Stress Reduction Theory [31–33], and Kellert and Wilson’s Biophilia Hypothe-
sis [34,35] provide a conceptual framework for the practice of shinrin-yoku and engaging
with nature in various forms of nature therapy. Shinrin-yoku researchers Song, Ikei, and
Miyazaki (2016) developed a conceptual framework based on an extensive review that de-
scribes how the restorative effects of nature increase physiologic immune system recovery
from stress as well as physiologic relaxation [36].
Kaplan and Kaplan hypothesized that exposure to natural settings through the five
senses has a direct effect on parasympathetic nervous system activation, thus leading to
states of greater awareness achieved through relaxation [29]. Ulrich’s Stress Reduction
Theory [31] was developed from observational studies wherein patients in hospitals with
patient room windows facing nature-laden scenery (e.g., trees, green foliage) experienced
marked improvement in health and recovery with shortened hospital stays compared to
patients in rooms with an urban view [31,32]. Wilson’s Biophilia Hypothesis [35], suggests

Int. J. Environ. Res. Public Health 2022, 19, 5373
3 of 17
that humans have a developmental affinity for natural surroundings, and being immersed
in nature is therefore innately appealing. This research suggests that a disconnect from
nature has adverse health impacts [34], and therefore finding effective means for individuals
to access nature is crucial [37,38].
1.2.2. Pain
Pain reduction is an emerging field of study in greenspace interventions [39], particu-
larly the relationships between pain, stress, and the burden of chronic illness [40–44]. To
date, several studies describe the pain-reducing effects of viewing nature (e.g., simulated
greenspaces) in clinical settings for acute and chronic pain populations [37,41,45–49].
Simulated nature and greenspace exposure has been applied in clinical settings for
the treatment of acute [41,46,47] and chronic pain [37,44,50]. Virtual reality (VR)-based
therapies for pain reduction are not new, and several theories for how and why VR-based
therapies improve pain outcomes center on the element of “distraction”, such that the
virtual viewing experiencing distracts an individual from feeling their pain [51–54]. This
is largely based on the Gate Control Theory proposed by Melzack and Wall [55], which
suggests that the attention paid to the pain experience, as well as the emotion tied to
the experience of pain, which includes past emotional memories, play a role in pain
interpretation; therefore, directing attention away from the experience of pain may reduce
the sensation of pain [47,53,56–59].
Research on VR-based greenspaces or nature exposure for pain reduction describes
VR as a tool for delivering nature, and that nature is the crucial element within the inter-
ventional design [47]. In a repeated-measures design, 50 patients attending chemotherapy
sessions were evaluated for pain and stress during intravenous port access. While findings
were insignificant after one nature-based VR session, participants reported feeling relaxed,
peaceful, and distracted by positive thoughts [47]. Potential benefits of virtual nature di-
rectly link to the theories describing the health effects of shinrin-yoku, including improved
relaxation, restoration, and alertness, improved functioning of the immune system, and
reduced exposure to air pollution and urbanicity [37]. Exposure to greenspaces can induce
relaxation via psychoendocrine pathways, including the function of the hypothalamic–
pituitary–adrenal (HPA) axis and resulting cortisol secretion [60,61]. Further, exposure to
greenspaces, which include greenery in the form of foliage, trees, and vistas, such as with
shinrin-yoku, improves health outcomes whether the exposure involves “live” nature or
virtual nature [62,63].
1.2.3. Biological Pathways of Interest
Immune suppression is a major issue for adults with a cancer diagnosis receiving
chemo- and/or radiation therapy. In particular, NK cell suppression in this population is
problematic as NK cells are the major immune cell type surveilling foreign or infectious
antigens and eliminating them [64]. Thus, implementation of a novel minimally invasive
immune therapy in cancer patients with solid tumors where NK cells are depleted, both
in number and activity, is crucial [27,28]. Patients with solid tumors that have activated
NK cells within the tumor have longer overall survival [65,66]. Blood levels of NK cells are
essential to the movement of NK cells into tumor tissue.
Research shows positive effects of forest bathing on NK cell numbers and activ-
ity [67] (NK CD3−/CD56+/ and NK CD3−/CD56+/CD69+, respectively) and on expressed
proteins, such as perforin and granulysin [6,20,68,69]. NK cells use pattern recognition
molecules (epitope) on the surface of transformed or stressed cells to accelerate detection
and elimination of problematic cells. Perforin and granulysin are key to enabling the
natural killing mechanism of the NK cell [70]. Perforin is a downstream effector related to
the number and activity of the NK cells [64]. Perforin creates a pore in the target cell once
the target cell’s epitope is recognized [64]. The pore allows granulysin to enter the cell and
effect apoptosis of the intracellular structures; the cell lyses and dies [5,64]. Perforin and

Int. J. Environ. Res. Public Health 2022, 19, 5373
4 of 17
granulysin are needed to maintain normal immune surveillance and reduction in infection,
specifically in immunocompromised cancer patients [27,28].
Two proof-of-principle studies were conducted in middle-to-older-aged healthy men.
These two studies, a 3-day forest experience (immersion experience) and a 3-night hotel
experience, measured or used humidified-forest-derived volatile organic compounds,
known as phytoncides, respectively. Of the phytoncides tested, humidified α- and β-pinene
and limonene in combination produced an increased number of NK cells and elevated
activity [6,20].
1.3. Purpose
If forest immersion can provide immune system benefits in healthy men (i.e., improved
NK cell numbers and activity, increased perforin and granulysin), can dispersal of three
phytoncides (α- and β-pinene and limonene in combination) paired with a greenspace
virtual reality provide the same positive effects on NK cells in patients with solid tumor
cancer who have completed cancer therapy? Additionally, can humidified limonene
paired with virtual reality reduce pain and psychological stress in patients with axial
spondyloarthritis? Our purpose is to deploy a standardized study protocol for simulated
forest immersion intervention in cancer patients with NK cell depletion and patients with
axial spondyloarthritis with chronic and breakthrough pain to test its feasibility and rigor.
The simulated forest immersion intervention will provide greenspace/forest experience
through three of the five senses. Virtual reality will provide visual and auditory stimuli.
Humidified aromatic forest oils will provide olfactory stimuli. Virtual reality and atomized
forest oils may be used in combination or alone [71]. Two distinct studies will use this
standardized protocol for (1) cancer patients and (2) patients with axial spondyloarthritis.
The purpose of this paper is to outline the development of the study protocol for the
intervention and the control conditions of the clinical lab setting.
2. Methods/Approach
2.1. Research Design
We will use a two-arm study design with concurrent controls selected from the breast
and prostate cancer clinics and from the arthritis clinic with two measurement time periods
to test the proposed simulated forest exposure intervention. In the SFIT study with patients
with axial spondyloarthritis who have chronic or breakthrough pain, the two-time points
were before and immediately after the intervention. In the SFIT study with patients with
either breast or prostate cancer, the two time periods were before and on Day 3 after the
intervention.
2.2. Study Sample
The study sample for study #1 will be recruited from cancer patients with solid tumors
(HR + HER2- breast, or prostate cancer) who have completed cancer therapy (hormone
therapy excepted) as this population may benefit the most from increases in NK cell number
and activity, perforin, and granulysin to prevent infection as patients become relatively
immunocompromised after chemo- or radiation therapy. For study #2, the study sample
will be recruited from axial spondyloarthritis patients who have chronic or breakthrough
pain, as virtual reality has been shown to reduce pain, and d-limonene administration
in animals has shown pain reduction. Since the two studies are set in the future and are
pilot studies, we expect for study #1 to recruit and enroll 25 participants and for study #2
to recruit and enroll 25 participants. For study #1, the participant number is limited by
budget and the cost of pre-clinical and clinical laboratory tests. For study #2, the participant
number is limited by budget and the cost of paper-based tools. Concurrent controls for both
studies will be identified by the clinicians in either the cancer clinics or the arthritis clinic.
Concurrent controls will meet the same study inclusion and exclusion criteria as those
who are enrolled in the study interventions. We expect to have 4 of each of the assigned
genders in the control groups. The control groups will be randomized to receive neither
Int. J. Environ. Res. Public Health 2022, 19, 5373
5 of 17
SFIT intervention, VR, or atomized phytoncides. They will be exposed to atomized water
dispersal for 1 h, the same length of time as the study participants who will receive the SFIT
interventions. All the same data will be collected for both study #1 and study #2 on these
control participants. At the end of the studies, should an effect of the SFIT intervention be
noted, the control participants will have the opportunity to complete the same intervention.
Clinicians will lead the recruitment of these patients, followed by a phone screening for
inclusion and exclusion conducted by the principal investigator and research associate.
2.2.1. Inclusion and Exclusion for SFIT—General Considerations
Since we will be using atomized phytoncides as well as virtual reality, either in
combination or separately, several exclusion criteria apply, as seen in Table 1.
Table 1. General exclusion criteria related to intervention only.
Exclusion Criterion
History of asthma [72]
Inability to detect common odors from
commercial fragrances [73]
History of smoking within 15 min before the
start of SFIT [74]
Allergy to pine or citrus aroma [74,75]
History of intractable seasickness [76]
History of seizures [77]
Limitations of vision and hearing not corrected
by eye lenses or hearing aids
Inability to complete study requisites
Rationale
Inhaled phytoncides may produce airway
irritation, asthma exacerbation, or
bronchoconstriction
Inhaled phytoncides provide half of the
intervention and smell of the forest
Smoking within 15 min before therapy will
alter the ability of the participant to detect
commercial fragrances or the aroma of the
phytoncides
Inhaled phytoncide aromas are pine and citrus
and may cause dermatitis
VR may cause nausea/vomiting without relief
after 5–10 min
VR may heighten susceptibility to
photosensitive seizure due to changing light in
the forest video
VR requires good vision and hearing correction
with eye lenses or hearing aids
Intervention directions must be followed;
specific to follow up measurements
Inclusion and Exclusion for SFIT for Breast and Prostate Patients
Participants will be included if they are willing and able to provide informed consent,
are of either biological sex, older than 18 years of age, and have completed cancer therapy
for HR + HER2 breast cancer or prostate cancer, Stage I–III, with no evidence of metastasis.
Participants will be excluded if they have a history of autoimmune disease, are on immune
modulating therapies (endocrine therapy allowed), have had surgery or an invasive proce-
dure in the past two months, and recent infection in the past two weeks (these are known
confounding variables in immune system measures of interest).
Inclusion and Exclusion for SFIT for Axial Spondyloarthritis Patients
Participants diagnosed with axial spondyloarthritis (axSpA) will be included if they
are willing and able to provide informed consent and are at least 18 years of age or older,
and they may be any sex or gender. Additional inclusion criteria are: a score of 4 or higher
on the 10-point Bath Ankylosing Spondylosis Disease Activity Index (BASDAI) (a standard
criterion for suboptimal control of symptoms and disease [78] with a correlation between
patient-reported BASDAI scores and measurable disease) [79], and a rheumatologist over-
seeing their care. Participants will be excluded if they are in an active phase of treatment
with biologic cytokine inhibitors (which may confound the effects of the intervention on

Int. J. Environ. Res. Public Health 2022, 19, 5373
6 of 17
outcomes measures) [80]. Use of commonly prescribed painkillers is acceptable, and we
will control for their use in the analysis.
2.3. Setting
The SFIT Lab is located in our Integrated Bio-Behavioral Lab space within our school.
The lab room, where the instrumentation for the SFIT is set up, is 20 feet × 15 feet with a
12-foot ceiling. The room has temperature control, so a consistent temperature between
deployments of SFIT with participants can be maintained, as well as lighting control, so the
lights can be dimmed when patients are using VR.
2.4. Intervention—Procedure
Our two studies are novel as no one to date has used simulated forest immersion
in patients with acute or chronic morbid conditions. The principal investigator (PI) and
research associate (RA) will implement SFIT in a separate room from the room used to
cross-check inclusion and exclusion, obtain informed consent, collect baseline measures,
and allow the participant to rest. Prior to the arrival of the participant, the SFIT intervention
space will be prepared. Preparation of the intervention space includes calibration of the
instruments that will measure volatile organic compound particles (phytoncides are volatile
organic compounds) and droplets, room temperature and humidity, and room surface
temperatures, followed by measurement of the ambient particles and droplets and room
temperature and humidity prior to the implementation of the atomized phytoncides [71,81].
Phytoncides α-pinene, β-pinene, and d-limonene (Floraplex Terpenes, Ypsilanti, MI, USA)
will be prepared for atomization with a commercially available atomizer (Asakuki 500 mL
Premium Atomizer, Tronhon Co., Ltd., Chongqing, China) that can emit phytoncides for
up to 3 h. Once the dose expected (0.80 ppm) reaches the dose published by Li [6], the
participant will be brought into the intervention room. To date, the Li study, which was
conducted with healthy men, has been the only study to record phytoncide dose in a
controlled setting. We will use this concentration as the target dose for our humidified
phytoncide set up. Both at the beginning and at the end of 1 h of exposure to the simulated
forest immersion therapy intervention, ambient phytoncide in the contained space will
be measured indirectly by measuring both the increase in ambient air particle mass and
number, as well as by measuring the change in total volatile organic compounds (VOCs).
Total particle numbers will be measured with a continuous ultrafine particle counter (P-Trak
8525, TSI, Shoreview, MN, USA), and the total VOCs will be measured with the portable
handheld monitor (Mini ppbRAE 3000, Honeywell International INC.; San Jose, CA, USA).
The P-Trak and Mini ppbRAE 3000 will measure the increase in particle numbers and
water droplets (aerosol), respectively, which will serve as a surrogate of relative exposure
to phytoncide. Continuous monitoring of room temperature and relative humidity will
be measured by the HOBO MX2301 Temperature/RH Data Logger (ONSET, Bourne, MA,
USA). Room surface temperature will be measured by ADC Adtemp Mini 432 Non-Contact
Infrared Thermometer (American Diagnostic Corporation, Hauppauge, NY, USA). VR
will be provided by VIVE Pro Eye, HTC (high-tech computer) Corporation, (New Taipei
City, Taiwan) with digital rendering of forested greenspace. Once 1 h of SFIT concludes,
the participant will be removed to the preparation area and given instructions related to
reporting unanticipated problems, adverse events, and serious adverse events, and an
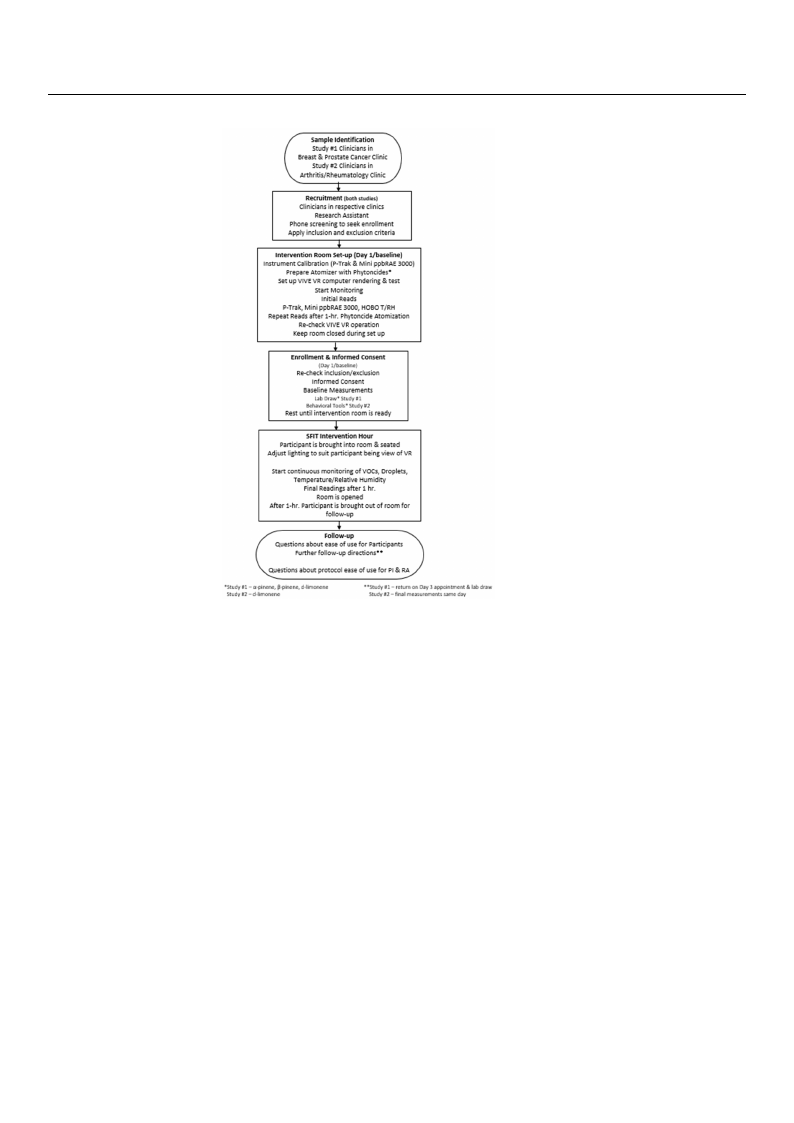
appointment to return for follow up on Day 3. See Figure 1, which illustrates the SFIT
process/procedure.
Int. J. Environ. RReess.. PPuubblliiccHHeeaalltthh 22002222,, 1199,, x53F7O3R PEER REVIEW
7 7ooff 117
Figure 1. SFIT process//pprroocceedduurree..
22..44..11.. IInntteerrvveennttiioonn——EEqquuiippmmeenntt aanndd CCaalliibbrraattiioonn
AAllll iinnssttrruummeennttss wwiillll bbee ppllaacceedd hhoorriizzoonnttaallllyy oonn aa ttaabbllee iinn tthhee cceenntteerr ooff tthheerroooomm aaggaaiinnsstt
oonnee wwaallll wwiitthh ssaammpplliinngg ppoorrttss ddiirreecctteedd ttoowwaarrddss tthhee ppaarrttiicciippaanntt ffoorr ooppttiimmaall mmeeaassuurreemmeenntt
aanndd ddiissppeerrssaall ooff pphhyyttoonncciiddeess..
PP--TTrraakk 88552255,, TTSSII,, SShhoorreevviieeww,, MMNN,, UUSSAA
bpaisalsibotiyclTTiiotahhyfteeimooPPfne--TsmaTrsrweauaakikrtsihinuissgrsaiapnpcecgaocorniptnfitiaictcnirlnethuisueocolaaueuslsstshsuamulestlfartsfalremlfaciafintassnlel1[-e8pa0-2p0as]ra.1ntri0mTtc0ilhc.elenUe(mUPF(U-FP.TPsFrU)aPaFkcr)oPecwusocniuualtlrrnerebtreee.cnrTuz.thlreyTrerehosPnte--uctTlPadyrl-iiaTebskrdtrauahktdtoaeishdefatidnhfsodettrohcaeaefisapsnccoaadh---
cuisaetiuonsisnwg iathchsapreccoiafilcfihlteearl.thBoetfhfedctusri[n82g].thTehceaPli-bTrraatkiown ialnl dbesuzrevroe-ycamliobdraet,erdesfeoarrceha-cghraudsee
uissoipnrgoapyclhaalrccoohaol lfiwltielrl.bBeouthsedduirninagsmthaellcaallciborhaotliocnaratrniddgseurcvheaymmbeordien, trheeseinarsctrhu-gmreandte. Tishoe-
pPr-Torpaykl halacsoahodlawtailllobgethuastedupindaatesms eavlleraylcmohinoluctearatnriddgheaschaammibneimr iunmthaenidnsmtrauxmimenutm. TrhaengPe-
Tthraatkihs ansoateddawtahleong tthheatinusptdruatmesenetveisryinmsiunruvteeyamndodhea.s Tahmeidnaimtaulmogawndillmbaexdimowumnloraadnegde
tohnattoias cnoomtepduwtehreunsitnhge sinofsttwruamreesnpt eicsifiinc sfourrvtheye Pm-Tordaek. [T8h3e].dAaltlasloofgtwwairlel wbeilldboewanclcoeasdseedd
ofrnotmo athceomP-pTuratkerwuesbinsgiteso[8ft1w].are specific for the P-Trak [83]. All software will be accessed
from the P-Trak website [81].
Mini ppbRAE 3000, Honeywell International Inc., San Jose, CA, USA
MiniTphpebpRpAbERA30E003,0H00omneeyawsuerlelsInvtoelrantialetioonrgaalnINicCco.;mSpanouJonsdes, (CVAOCs) related to the phyton-
cidesTtheatpwpebRarAeEat3o0m00izminega. sTuhreespvpoblRaAtilEe3o0r0g0anwiicllcboemzpeorou-ncadlsib(rVaOteCdsu)srienlgataedchtaorcthoaelpzheyro-
tfiolntecridaensdthIsaotbwuetyalreenaetoAmirizBianlga.nTchede pspabnRAgaEs3[08040].wFoilrl btwe oze-proo-icnatlicbarlaibterdatuiosnin, gisaobcuhtayrlceonael
zaetr1o0fpilptemr aannddI1so0b0uptpymlenweiAllibreBualsaendce[8d5s].pDanugriansg[8tw4]o. -Fpooritnwt oca-pliobirnatticoanli,bwraetiwonil,liusosebuatysel-t
e0n.5eLaPt M10rpepgumlaatnord. 1T0h0isprpemguwlatilolrbceanusheadn[d8l5e].uDputorin50g0twpsoi,-pwohinicthciaslitbhreatpisoino, fwtheewsipllaunsgeaas
sceytli0n.5deLrPsManrdegaulsloatwori.thTihnisthregtouleartaotriocannlihmaintdolfetuhpe ptop5b0R0ApEsi3, 0w0h0ircehgiasrtdhiengpspiroefssthuerespanand
gflaoswc.yIltinisdiemrspaonrdtaanltstohwatithiengtahsectyolienrdateironcolnimneitctoifotnhies pCpGbARA6E003a0n00d rceograrredspinognpdrsetsosuthre

Int. J. Environ. Res. Public Health 2022, 19, 5373
8 of 17
connection on the regulator, meaning that the threading has to be compatible between the
cylinder and the regulator. If 500 psi is exceeded during calibration or survey mode, the
diaphragm within the RAE 3000 may be damaged, leading to inaccurate data collection. In
survey mode, data will be updated every 60 s and a data log will be created. The data log
will be downloaded using software specific to the ppbRAE 3000 and found online [82].
HOBO MX2301 Temperature/RH Data Logger, ONSET, Bourne, MA, USA
The HOBO temperature and relative humidity (HOBO T/RH) data logger, which
is suitable for both indoor and outdoor application, is a small portable unit that uses an
application (HOBOConnect) loaded onto a mobile device. The app will use a Bluetooth
connection to the HOBO T/RH that is easily configurable and logs temperature and relative
humidity in real time that you will view on our mobile device, in this case an iPhone. The
HOBO T/RH will be placed within a 30 m line of sight towards the participant. Due to
the size of the room within which we will set up the intervention, we will use one HOBO
T/RH. Data download will be accomplished when the iPhone (mobile device) is within
100 m of the HOBO T/RH unit. Data updates every 2 min with an accuracy of ±0.2 ◦C and
±3.5% RH [86]. Data software will be downloaded online [84].
Measurement of Ambient Room Conditions
Room temperature and humidity may alter the overall measurement of particle num-
ber and droplets. Measuring all four of these ambient conditions will allow for consistency
in the experimental condition between participants. The room has a set temperature of
70 ◦F, and since the room is located against a foundation wall, humidity may vary; there-
fore, it is important to monitor both of these ambient conditions and use cutoff criteria
based on average temperature and humidity of the controlled lab setting. We will also use
a non-contact infrared surface thermometer to measure radiant heat of room surfaces that
may add to the perceived comfort of the SFIT intervention room [81]. The ADC Adtemp
Mini 432 Non-Contact Infrared Thermometer (American Diagnostic Corporation, Haup-
pauge, NY, USA) with a range of 59–77 ◦F will be used for this purpose. The ambient room
air temperature, humidity, and surface temperature date will be collected as a mean prior
to, during, and at the end of the intervention.
Asakuki 500 mL Premium Atomizer, Tronhon Co., Ltd., Chongqing, China
The atomizer holds 500 mL of liquid that can be atomized over 3 h. Of that 500 mL, a
portion will be reduced that coincides with the amount of phytoncide that will be added.
We expect that we will add 30 mL per phytoncide to the atomizer to achieve the detectable
published amount [6,21]. Mist will be created by an ultrasonic plate within the atomizer,
and the mist will be adjusted for a weak mist or a strong mist. Choice of weak or strong
mist will be adjusted to fit the published detectable amount of phytoncide. Mist time can
be regulated to maintain 60, 120, and 180 min of operation. We will use a 60 min mist time
with the participants of study #1 and study #2. A fan within the atomizer will disperse the
mist into the room. Room temperature and humidity will be monitored continuously as
low temperature and high humidity may condense the mist into water droplets [87], which
is to be avoided to allow for accurate dose calculations.
Phytoncides, Floraplex Terpenes, Ypsilanti, MI, USA
α-pinene, β-pinene, and d-limonene are the phytoncides (forest oils) of interest for
SFIT. Interestingly, all three in combination have been tested in normal males in both
forest immersion and hotel/sleep contexts and have shown effective elevations in NK cell
numbers and activity as well as increased expression of perforin and granulysin [5,6,20,21].
However, these three phytoncides have not been tested in the SFIT context with breast
and prostate cancer patients. D-limonene alone has been tested in the context of pain
and shown to be effective in an animal model when not paired with VR [88]. All three
phytoncides are available as purified isolates in containers of 4, 8, or 32 ounces. The

Int. J. Environ. Res. Public Health 2022, 19, 5373
9 of 17
phytoncides will be added to the Asakuki atomizer with an easy calculation of ounces to
ml, and that amount will be subtracted from the 500 mL total container in the atomizer so
as to maintain a standardized addition of phytoncides:water ratio. Measurement of this
mixed mist by ultrafine particulate and VOC survey will be the method of determining the
dose of the phytoncide.
VIVE Pro Eye, HTC (High-Tech Computer) Corporation, New Taipei City, Taiwan
The VIVE Pro Eye is capable of delivering digitally rendered greenspace visual record-
ings from forested or park-like greenspaces. The headset has sensors that coordinate the
virtual greenspace with the participants’ visual gaze (native eye tracking) to move the
surroundings of the digital greenspace through interaction with the base stations using
motion sensors mounted on tripods in front of the participant [89,90]. Set up will include
downloading the VIVE and SteamVR software onto a computer specifically dedicated for
the VIVE system (e.g., using Windows 10 operating system). Tracking will be performed
on the computer software and saved for later review during data entry [91]. The computer
will be located behind the chair in which the participant will be sitting. Sounds will be
adjusted for those that are a part of the virtual greenspace; ambient sounds in the room
will be muted. Although software comes with the purchase of the VIVE system, training
videos can be found online and will be completed before use [87–89].
2.5. Baseline Fidelity Measures—Linkages to Equipment
Perception of air quality prior to introduction of phytoncides into the room’s air will
be evaluated repeatedly prior to each intervention day using two healthy individuals of
both assigned sexes each time to assess the air quality of the room at the set temperature of
70 ◦F while monitoring the relative humidity. We will use the facial exposure method as
described by Fang, Clausen, and Fanger [92]. In order to ensure fidelity of the measures of
phytoncide dose prior to, during, and at the end of the intervention period, the equipment
mentioned above will be zero and span-calibrated before introduction of phytoncides into
the room’s air. Recording temperature and humidity using the HOBO T/RH before and
during the intervention will ensure that the reliability of the survey data from the P-Trak
and the ppbRAE 3000 has not been affected by changes in temperature and humidity.
Feasibility and Reliability of Intervention Stability
We expect to determine the ease of use of VR and phytoncide atomization, the drop off
of phytoncide over the intervention period, and engagement in VR leading to a standard-
ization of the procedure and protocol. Data will be collected from the participant, and the
research associate and principal investigator will use field notes and will include challenges
and facilitators related to the delivery method of VR and phytoncides and the ability of
the participant to engage in VR for the duration of the study intervention. Atomized
phytoncides prior to and after 1 h of dose delivery will be used to measure by the P-trak
and the Mini ppbRAE3000 to determine dose drop off during the intervention delivery.
Quantitative data related to dose drop off will be analyzed by t-test with an α level of 0.05.
We will collect deviations from the standardized procedures, including the deployment
of VR and atomized phytoncides. We will monitor the timing, preservation, and delivery
of specimens to specialized labs on the academic healthcare campus in order to track the
ability to maintain the expected optimized rigor in testing immune cells.
2.6. Data Collection
Since the participants will be recruited from the breast and prostate cancer clinics
and the rheumatology clinic, the medical history that appears in the EPIC electronic
medical record will be available for review prior to enrollment per IRB approval (OHSU
IRB#00023183) and cross-checked with the participants after we have obtained informed
consent on the day of the SFIT intervention. This will serve as the start of the data collection
process for determining inclusion/exclusion of participants (see Section 2.2.1, Table 1; In-

Int. J. Environ. Res. Public Health 2022, 19, 5373
10 of 17
clusion and Exclusion for SFIT for Breast and Prostate Patients and Inclusion and Exclusion
for SFIT for Axial Spondyloarthritis Patients) and baseline data collection (see Section 2.6.1,
Section 2.7, and its subsections, and Section 2.8 and its subsections). Case report forms will
be used to capture participant baseline and data collected at all pertinent time points per
protocol and will serve as a hard-copy record of data, which we will enter into a research
electronic data capture system, as required by our university.
2.6.1. Baseline
Demographic data collection will occur prior to the start of both SFIT intervention
studies and will be specific to each population of interest [93]. The behavioral/psychological
measures, biological measures, and feasibility measures will be collected prior to placement
of the participant in the SFIT intervention room.
2.6.2. Follow Up
Follow-up data collection will be within the 3–4-day period after the SFIT intervention
and in study #1 participants with breast or prostate cancer and will include blood specimens
for CBC with differential counts of leukocytes, NK cell phenotyping and plasma for perforin
and granulysin ELISAs [6]. We will survey the participants on events that might affect
immune response. Every effort will be made to minimize the amount of blood drawn.
Data collection will occur immediately after the intervention for study #2 participants
with AxSpA and include the same measures as baseline as well as the intervention fidelity
measures. Follow up will also include collection of adverse events, serious adverse events,
and unanticipated problems, per IRB protocol for intervention studies.
2.7. Measures—Behavioral/Psychological
To measure the impact of SFIT on patients with chronic or breakthrough pain due
to axial spondyloarthritis (axSpA), scales which interpret the direct effect on symptoms
of pain, psychological distress, and physical functionality specific to axSpA will be used.
These include the Visual Analog Scale for pain [94,95], the Depression, Anxiety, and Stress
Scale [96,97], and the Bath Ankylosing Spondylitis Disease Activity Scale [98].
2.7.1. Demographics
Demographic characteristics of participants will include clinically relevant ethno-
graphic details specific to assigned sex (male or female), race, and ethnicity. Diagnostic
information specific to axSpA, including date of diagnosis and onset of symptoms (date),
chronicity of symptoms (in months), and non-biologic medication management (name
of medication/last date of use), will be ascertained. Since culture, religion, and personal
belief systems influence perception of pain, depression, stress, and functionality, we will
include questions about these three pertinent individual characteristics in our baseline
demographic data collection [99].
2.7.2. Visual Analog Scale (VAS)
The VAS is a widely used self-reported tool measuring present-state perceived pain
intensity [100]. Patients will be asked to indicate their perceived pain intensity along a
10 cm horizontal line (which can be on paper or computerized), and this rating will then
be measured from the left edge up to the indicated marking to represent the level of pain
intensity. The line represents a continuum between “no pain” and “worst pain”. The VAS
is often used in clinical settings and is sensitive in determining the effect of comfort or
pharmacological interventions [94]. The VAS has performed well on psychometric tests of
validity (for example, η2 = 0.47; F = 0.44 [94,101]), and reliability (rs,VAS = 0.52–0.89 [102])
for measuring pain clinically. VAS scores will be treated as ratio data [103].

Int. J. Environ. Res. Public Health 2022, 19, 5373
11 of 17
2.7.3. Depression, Anxiety, and Stress Scale (DASS)
The DASS comprises a set of three self-report scales, which are intended to measure
clinically significant symptoms of emotional states of depression, anxiety, and stress [96,104].
Each of the three DASS scales (depression, anxiety, and stress) contains 14 items, divided
into subscales of 2–5 items measuring the same construct, for a total of 42 items. The
participants will be asked to complete the DASS prior to and immediately after the SFIT
intervention. The DASS, which is intended to measure symptom severity of self-reported
negative emotional states, including depression, anxiety, and stress, shows good psychome-
tric validity and reliability (Cronbach’s α = 0.89; test–retest and split-half reliability scores
are rDASS = 0.99 and 0.96, respectively [96]) as a dimensional measurement of psychological
distress associated with chronic conditions [104].
2.7.4. Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)
The BASDAI is commonly used to measure clinical symptoms of AS and axSpA,
including fatigue, spinal pain, joint pain related to swelling, and enthesitis, or inflammation
of the tendons and ligaments, as well as morning stiffness duration and severity [105]. It
consists of 6 self-report questions, with each question scored from 1, representing “none” or
no symptoms, to 10, representing “the worst”, with the score from the questions pertaining
to morning stiffness and duration averaged such that 5 questions in total are scored. The
participants will be asked to complete the BASDAI prior to and immediately after the SFIT
intervention. The resulting score (from 0 to 50) is divided by 5 to give a final BASDAI score
of 0–10, with scores of 4 or greater indicating significant disease [106]. The BASDAI has
demonstrated extraordinary reliability at p < 0.001 [105]. In a test of validity of the BASDAI
for AS patients, Cronbach’s α = 0.786 [98].
2.8. Measures—Biological/Immune System
We will use established pre-clinical and clinical measures to characterize the immune
responses before and after the simulated forest exposure intervention.
2.8.1. Demographics
Demographic characteristics of participants will include clinically relevant ethno-
graphic details specific to age, assigned sex (male or female), race, and ethnicity, and history
of smoking.
2.8.2. CBC and Differential Cell Count
Complete blood count (CBC) and differential cell counts will be measured at baseline
(prior to implementation of the simulated forest exposure intervention) and at Day 3.
Correlation between this clinical measure and the data from flow cytometry and ELISA
(outlined below) will be conducted to translate the pre-clinical findings into clinical use. A
whole blood sample for a CBC with a differential cell count will be collected two times using
a 4 mL EDTA tube, prior to the SFIT intervention and on Day 3 after the SFIT intervention.
This measure will include WBC count and percentages of 100 cell counts and absolute
counts for neutrophils, lymphocytes, and monocytes. The clinical core laboratory at OHSU
complies with established inter- and intra-assay parameters as it is accredited by Clinical
Laboratory Improvement Amendments.
2.8.3. Flow Cytometry for NK Cell Number and Activity
Flow cytometry is used to monitor immune system changes tied to specific dis-
ease states, which makes it ideal for defining cellular responses of interest [107]. NK
CD3−/CD56+ and NK CD3−/CD56+/CD69+, (i.e., NK number and activity, respectively)
will be measured by flow cytometry immunophenotyping using freshly collected periph-
eral whole blood (approximately 4 mL). Cells will be prepared for flow cytometry using
the standard fluorescence-activated cell sorting method. Data analysis will be performed

Int. J. Environ. Res. Public Health 2022, 19, 5373
12 of 17
by gating on live cells based on forward versus side scatter profiles, then on singlets using
forward scatter area versus height, followed by cell-subset-specific gating [107].
2.8.4. Perforin Expression
Perforin expression will be measured by an enzyme-linked immunosorbent assay
(ELISA) and will be used to monitor downstream perforin secretion due to NK cell activ-
ity [27]. Perforin will be measured using plasma extracted from whole blood, which will
be frozen at −80 ◦C and stored until needed for the assay. Optimized ELISA kits from
ThermoFisher Scientific, Waltham, MA, USA, will be used per manufacturer instructions to
detect perforin levels. The enzyme-dependent color change will be read out on a Multi-
Mode Mircroplate Reader. Perforin concentration will be extrapolated from the standard
curve [108].
2.8.5. Granulysin Expression
Granulysin expression will be measured by an enzyme-linked immunosorbent assay
(ELISA), which will be used to monitor downstream granulysin secretion due to NK cell
activity [27]. Granulysin will be measured using plasma extracted from whole blood, which
will be frozen at −80 ◦C and stored until needed for the assay. Optimized ELISA kits
from AbCam, Cambridge, MA, USA, will be used per manufacturer instructions to detect
granulysin levels. The enzyme-dependent color change will be read out on a Multi-Mode
Mircroplate Reader. Granulysin concentration will be extrapolated from the standard
curve. For both perforin and granulysin expression, we will need 4 mL of freshly collected
peripheral whole blood [108].
2.9. Follow-Up Measures Day 3
In addition to collecting whole-blood specimens for CBC with differential, NK cell
number and activity, perforin, and granulysin, we will note any unanticipated problems,
adverse events and serious adverse events affecting the participants per IRB protocol for
intervention studies. Unanticipated problems will be determined with the assistance of
the clinicians and the study team as these are determined through a ranking procedure
specified by our university’s Office of Human Research Protections. Adverse events will
include subjective or objective symptoms occurring spontaneously, significant clinical lab
abnormalities, a worsening of the participants condition from baseline, are recurrence or
increase in signs and symptoms of original disease that occur after the SFIT intervention
and are worsened or changed in quality. Serious adverse events will include death, life-
threatening adverse event, new hospitalization or prolongation of current hospitalization, or
a new significant incapacity or new substantial inability to complete activities of daily living.
3. Discussion
We have presented our lab set up for the SFIT intervention. The SFIT intervention as
described may be used in a multi-arm design with a control group, using VR only, phyton-
cide atomization only, or both in combination. We expect to use whatever combination is
proven to be most effective as a minimally invasive intervention for all of the following
designs in a stepwise progression: longer intervention duration to optimize dose effect;
intermittent, but repeated intervention to optimize dose effect drop off; and home use
application to move the optimized intervention into practical use.
An intervention using VR and humidified phytoncides, α- and β-pinene, and limonene,
in a simulated forest exposure intervention as a substitute for forest bathing in AXSpA
patients with chronic or breakthrough pain and cancer patients with early-stage solid
tumors (HR + HER2- breast cancer and prostate cancer) who have completed surgery or
chemo- and/or radiation therapy (exclusive of hormone therapy) is possible in a lab setting.
Moving SFIT to a home setting may be challenging, but not insurmountable.

Int. J. Environ. Res. Public Health 2022, 19, 5373
13 of 17
3.1. Expected Outcomes
The expected outcome for the future two studies is the creation of a standardized
protocol for deploying SFIT. This will include calibration and measurement set points,
cutoff criteria and describing how to maintain a consistent dose of phytoncide and ease the
use of VR for participants. We expect to uncover pertinent adverse events, severe adverse
events, and unanticipated problems. For study #1, we expect that the combined use of our
three phytoncides of interest and VR will improve NK cell numbers and activity and blood
levels of perforin and granulysin in patients with breast or prostate cancer. For study #2,
we expect that the use of d-limonene and VR will reduce pain, stress, and depression in
patients with axial spondyloarthritis.
3.2. Lessons Learned
We have had challenges with procurement of supplies during the current development
and delivery backlog produced by delays in shipping due to COVID-19 conditions in our
current world state. Some of these were delivered relatively quickly, within one week;
however, we procured span gas of the wrong concentration, and the next week all span
gas was out of stock nationwide with a delay in the expected delivery of 1–2 months.
Phlebotomy supplies have been challenging to obtain through our medical supply process
within the university due to the increased usage of the supplies to care for COVID-19
patients. At times, our academic medical center announced requests for a reduction in the
usage of various supplies for laboratory work. The lesson learned here is to start early
after IRB approval and be aware of potential delays that might encumber grant funding
previously awarded.
The cylinder containing the span gas connection and the fitting to the regulator must
match. If the cylinder has a male threading and the regulator has female threading, these
may match, but care needs to be taken in looking at the specification of the cylinder
connection with respect to the regulator connection. In our case, we needed to have male
threading on the replacement span gas with a connection that was a CGA 600 specification
in order to match our existing regulator. The replacement price differential is 12:1 with the
regulator being much more expensive than the span gas cylinder.
4. Conclusions
We have presented the theoretical conceptions and established the foundation for the
move to the pragmatic operations of the SFIT intervention. SFIT is in its early stages as a
potential therapy in the two populations of interest to us presented here. We expect further
development in building this novel lab set up in the immediate foreseeable future as we
work to move this therapy into the home setting under the control of patients needing
this minimally invasive therapy. This is relevant to healthcare science because healthcare
providers are responsible for optimizing patient healing and recovery, while reducing the
harmful effects of therapies that deleteriously affect the patient’s ability to thrive with their
chronic or temporarily morbid conditions.
Author Contributions: Conceptualization, A.M.R. and R.J.F.J.; methodology, A.M.R.; writing—
original draft preparation, A.M.R. and R.J.F.J.; writing—review and editing, A.M.R.; funding acquisi-
tion, A.M.R. All authors have read and agreed to the published version of the manuscript.
Funding: This research is funded by Sigma Theta Tau International, Beta Psi Chapter, under grant
number GSONO0529A; the OHSU School of Nursing Small Grants Program—Innovation Grants,
under grant number GSONO0530A; and Hartford Center of Nursing Excellence—Hartford Award
for Research and Practice, under grant number GSONO0531A.
Institutional Review Board Statement: The OHSU Institutional Review Board approved this study,
10.4.21, IRB#00023183.
Informed Consent Statement: Informed consent will be obtained from all subjects involved in the
study, once we are enrolling participants.

Int. J. Environ. Res. Public Health 2022, 19, 5373
14 of 17
Data Availability Statement: Not applicable.
Acknowledgments: Equipment was donated in kind by Hector A. Olvera-Alvarez from the OHSU
School of Nursing Integrated Bio-behavioral Laboratory.
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Li, Q. Shinrin-Yoku: The Art and Science of Forest Bathing; Penguin: London, UK, 2018.
2. Miyazaki, Y. Shinrin Yoku: The Japanese Art of Forest Bathing; Timber Press: Portland, OR, USA, 2018.
3. Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in
forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 71–82. [CrossRef]
4. Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest
atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15,
18–26. [CrossRef]
5. Li, Q.; Kobayashi, M.; Inagaki, H.; Wakayama, Y.; Katsumata, M.; Hirata, Y.; Li, Y.; Hirata, K.; Shimizu, K.; Nakadai, A.; et al.
Effect of phytoncides from forest environments on immune function. In Forest Medicine; Nova Science Publishers, Inc.: New York,
NY, USA, 2013; pp. 159–169.
6. Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, K.; Kawada, T.; Park, B.J.; et al.
Effect of phytoncide from trees on human natural killer cell function. Int. J. Immunopathol. Pharmacol. 2009, 22, 951–959. [CrossRef]
7. Andersen, L.; Corazon, S.S.S.; Stigsdotter, U.K. Nature Exposure and Its Effects on Immune System Functioning: A Systematic
Review. Int. J. Environ. Res. Public Health 2021, 18, 1416. [CrossRef]
8. Cho, K.S.; Lim, Y.R.; Lee, K.; Lee, J.; Lee, J.H.; Lee, I.S. Terpenes from Forests and Human Health. Toxicol. Res. 2017, 33, 97–106.
[CrossRef]
9. Tsunetsugu, Y.; Park, B.J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the
atmosphere of the forest) in an old-growth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142.
[CrossRef]
10. Antonelli, M.; Donelli, D.; Carlone, L.; Maggini, V.; Firenzuoli, F.; Bedeschi, E. Effects of forest bathing (shinrin-yoku) on individual
well-being: An umbrella review. Int. J. Environ. Health Res. 2021, 1–26. [CrossRef]
11. Muro AFeliu-Soler ACanals, J.; Parrado, E.; Sanz, A. Psychological benefits of Forest Bathing during the COVID-19 pandemic: A
pilot study in a Mediterranean forest close to urban areas. J. For. Res. 2021, 27, 71–75.
12. Hansen, M.M.; Jones, R. The Interrelationship of Shinrin-Yoku and Spirituality: A Scoping Review. J. Altern. Complement. Med.
2020, 26, 1093–1104. [CrossRef]
13. Timko Olson, E.R.; Hansen, M.M.; Vermeesch, A. Mindfulness and Shinrin-Yoku, potential for Physiological and Psychological
Interventions during Uncertain Times. Int. J. Environ. Res. Public Health 2020, 17, 9340. [CrossRef]
14. Wen, Y.; Yan, Q.; Pan, Y.; Gu, X.; Liu, Y. Medical empirical research on forest bathing (Shinrin-yoku): A systematic review. Environ.
Health Prev. Med. 2019, 24, 70–91. [CrossRef]
15. Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku
(Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409–421. [CrossRef]
16. Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J.
Environ. Res. Public Health 2017, 14, 851. [CrossRef]
17. Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H., Jr.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf,
K.L.; et al. Nature contact and human health: A research agenda. Environ. Health Perspect. 2017, 125, 075001–075019. [CrossRef]
18. Furuyashiki, A.; Tabuchi, K.; Norikoshi, K.; Kobayashi, T.; Oriyama, S. A comparative study of the physiological and psychological
effects of forest bathing (Shinrin-yoku) on working age people with and without depressive tendencies. Environ. Health Prev. Med.
2019, 24, 46. [CrossRef]
19. Maydych, V. The Interplay Between Stress, Inflammation, and Emotional Attention: Relevance for Depression. Front. Neurosci.
2019, 13, 384. [CrossRef]
20. Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [CrossRef]
21. Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.; Wakayama, Y.; et al.
Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol.
Pharmacol. 2008, 22, 117–127. [CrossRef]
22. Institute, N.C. Statistics at a Glance: The Burden of Cancer in the United States. 2020. Available online: https://www.cancer.gov/
about-cancer/understanding/statistics (accessed on 22 February 2022).
23. Reveille, J.D.; Witter, J.P.; Weisman, H.M. Prevalence of Axial Spondylarthritis in the United States: Estimates From a Cross-
Sectional Survey. Arthritis Care Res. 2012, 64, 905–910. [CrossRef]
24. Mogard, E.; Olofsson, T.; Bergman, S.; Bremander, A.; Kristensen, L.E.; Olsen, J.K.; Wallman, J.K.; Lindqvist, E. Chronic Pain and
Assessment of Pain Sensitivity in Patients With Axial Spondyloarthritis: Results From the SPARTAKUS Cohort. J. Rheumatol.
2021, 48, 1672–1679. [CrossRef]

Int. J. Environ. Res. Public Health 2022, 19, 5373
15 of 17
25. Magrey, M.N.; Mease, P.J. Pain in Axial Spondyloarthritis: More to It Than Just Inflammation. J. Rheumatol. 2021, 48, 1632.
[CrossRef] [PubMed]
26. Nowell, W.B.; Gavigan, K.; Hunter, T.; Bolce, R.J.; Lisse, J.R.; Himelein, C.; Dubey, S.; Curtis, J.R.; Walsh, J.A. Patient Perspectives
of Biologic Treatments for Axial Spondyloarthritis: Satisfaction, wear-off between doses, and use of supplemental medications.
Ann. Rheum. Dis. 2021, 80 (Suppl. 1), 1034. [CrossRef]
27. Huntington, N.G.; Cursons, J.; Rautela, J. The cancer–natural killer cell immunity cycle. Nat. Rev. Cancer 2020, 20, 437–454.
[CrossRef] [PubMed]
28. Shimasaki, N.; Jain, A.; Campana, D. NK cells for cancer immunotherapy. Nat. Rev. Drug Discov. 2020, 19, 200–218. [CrossRef]
29. Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [CrossRef]
30. Kaplan, R.; Kaplan, S. The experience of nature: A psychological perspective. In The Experience of Nature: A Psychological Perspective;
Cambridge University Press: New York, NY, USA, 1989; Volume xii, p. 340.
31. Ulrich, R.S.; Simmons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban
environments. J. Environ. Psychol. 1991, 11, 201–230. [CrossRef]
32. Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [CrossRef]
33. Ulrich, R.S. Aesthetic and Affective Response to Natural Environment. In Behavior and the Natural Environment; Altman, I.,
Wohlwill, J.F., Eds.; Springer: Boston, MA, USA, 1983; pp. 85–125.
34. Kellert, S.R.; Case, D.D.; Escher, D.; Witter, D.J.; Mikels-Carrasco, J.; Seng, P.T. The Nature of Americans: Disconnection and
Recommendations for Reconnection; The Nature of Americans National Report; DJ Case and Associates: Mishawaka, IN, USA, 2017;
Volume 11, p. 2018.
35. Wilson, E.O. Biophilia: The Human Bond with Other Species; Harvard University Press: Cambridge, MA, USA, 1984.
36. Song, C.; Ikei, H.; Miyazaki, Y. Physiological Effects of Nature Therapy: A Review of the Research in Japan. Int. J. Environ. Res.
Public Health 2016, 13, 781. [CrossRef]
37. White, M.P.; Yeo, N.L.; Vassiljev, P.; Lundstedt, R.; Wallergård, M.; Albin, M.; Lõhmus, M.A. A prescription for “nature”—The
potential of using virtual nature in therapeutics. Neuropsychiatr. Dis. Treat. 2018, 14, 3001–3013. [CrossRef]
38. Hunter, R.F.; Cleland, C.; Cleary, A.; Droomers, M.; Wheeler, B.W.; Sinnett, D.; Nieuwenhuijsen, M.J.; Braubach, M. Environmental,
health, wellbeing, social and equity effects of urban green space interventions: A meta-narrative evidence synthesis. Environ. Int.
2019, 130, 104923. [CrossRef]
39. Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.;
Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ.
Res. 2017, 158, 301–317. [CrossRef] [PubMed]
40. Shanahan, D.F.; Astell-Burt, T.; Barber, E.A.; Brymer, E.; Cox, D.; Dean, J.; Depledge, M.; Fuller, R.A.; Hartig, T.; Irvine, K.N.; et al.
Nature-Based Interventions for Improving Health and Wellbeing: The Purpose, the People and the Outcomes. Sports 2019, 7, 141.
[CrossRef] [PubMed]
41. Tashjian, V.C.; Mosadeghi, S.; Howard, A.R.; Lopez, M.; Dupuy, T.; Reid, M.; Martinez, B.; Ahmed, S.; Dailey, F.; Robbins, K.; et al.
Virtual Reality for Management of Pain in Hospitalized Patients: Results of a Controlled Trial. JMIR Ment. Health 2017, 4, e9.
[CrossRef] [PubMed]
42. Kang, B.; Kim, T.; Kim, M.J.; Lee, K.H.; Choi, S.; Lee, D.H.; Kim, H.R.; Jun, B.; Park, S.Y.; Lee, S.J.; et al. Relief of–Chronic Posterior
Neck Pain Depending on the Type of Forest Therapy: Comparison of the Therapeutic Effect of Forest Bathing Alone Versus Forest
Bathing With Exercise. Ann. Rehabil. Med. 2015, 39, 957–963. [CrossRef] [PubMed]
43. Stanhope, J.; Breed, M.F.; Weinstein, P. Exposure to greenspaces could reduce the high global burden of pain. Environ. Res. 2020,
187, 109641–109651. [CrossRef]
44. Li, H.; Zhang, X.; Bi, S.; Cao, Y.; Zhang, G. Can Residential Greenspace Exposure Improve Pain Experience? A Comparison
between Physical Visit and Image Viewing. Healthcare 2021, 9, 918. [CrossRef]
45. Ali Khan, M.; Amin, N.; Khan, A.; Imtias, M.; Khan, F.; Ahmad, I.; Ali, A.; Islam, B. Plant Therapy: A Nonpharmacological and
Noninvasive Treatment Approach Medically Beneficial to the Wellbeing of Hospital Patients. Gesunde Pflanz. 2016, 68, 191–200.
[CrossRef]
46. Lechtzin, N.; Busse, A.M.; Smith, M.T.; Grossman, S.; Nesbit, S.; Diette, G.B. A Randomized Trial of Nature Scenery and Sounds
Versus Urban Scenery and Sounds to Reduce Pain in Adults Undergoing Bone Marrow Aspirate and Biopsy. J. Altern. Complement.
Med. 2010, 16, 965–972. [CrossRef]
47. Scates, D.; Dickinson, J.I.; Sullivan, K.; Cline, H.; Balaraman, R. Using Nature-Inspired Virtual Reality as a Distraction to Reduce
Stress and Pain Among Cancer Patients. Environ. Behav. 2020, 52, 895–918. [CrossRef]
48. Sjölander, A.; Jakobsson Ung, E.; Theorell, T.; Nilsson, Å.; Ung, K.A. Hospital Design with Nature Films Reduces Stress-Related
Variables in Patients Undergoing Colonoscopy. Health Environ. Res. Des. J. 2019, 12, 186–196. [CrossRef]
49. Wells, N.M.; Rollings, K.A.; Ong, A.D.; Carrinton Reid, M. Nearby Nature Buffers the Pain Catastrophizing–Pain Intensity
Relation Among Urban Residents With Chronic Pain. Front. Built Environ. 2019, 5, 142. [CrossRef]
50. Tanja-Dijkstra, K.; Pahl, S.; White, M.P.; Auvray, M.; Stone, R.J.; Andrade, J.; May, J.; Mills, I.; Moles, D.R. The Soothing Sea: A
Virtual Coastal Walk Can Reduce Experienced and Recollected Pain. Environ. Behav. 2017, 50, 599–625. [CrossRef]
51. Trost, Z.; France, C.; Anam, M.; Shum, C. Virtual reality approaches to pain: Toward a state of the science. Pain 2021, 162, 325–331.
[CrossRef]

Int. J. Environ. Res. Public Health 2022, 19, 5373
16 of 17
52. Lambert, V.; Boylan, P.; Boran, L.; Hicks, P.; Kirubakaran, R.; Devane, D.; Matthews, A. Virtual reality distraction for acute pain in
children. Cochrane Database Syst. Rev. 2020, 10, Cd010686.
53. Bani Mohammad, E.; Ahmad, M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer:
A randomized control trial. Palliat. Support. Care 2019, 17, 29–34. [CrossRef]
54. Malloy, K.M.; Milling, L.S. The effectiveness of virtual reality distraction for pain reduction: A systematic review. Clin. Psychol.
Rev. 2010, 30, 1011–1018. [CrossRef]
55. Melzack, R.; Wall, P.D. Pain Mechanisms: A New Theory. Science 1965, 150, 971–979. [CrossRef]
56. Ropero Peláez, F.J.; Taniguchi, S. The Gate Theory of Pain Revisited: Modeling Different Pain Conditions with a Parsimonious
Neurocomputational Model. Neural Plast. 2016, 2016, 4131395. [CrossRef]
57. Perrot, S.; Cohen, M.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.D. IASP Taskforce for the Classification of Chronic Pain. The IASP
classification of chronic pain for ICD-11: Chronic secondary musculoskeletal pain. Pain 2019, 160, 77–82. [CrossRef]
58. Johnson, M.H. How does distraction work in the management of pain? Curr. Pain Headache Rep. 2005, 9, 90–95. [CrossRef]
59. Rischer, K.M.; González-Roldán, A.M.; Montoya, P.; Gigl, S.; Anton, F.; van der Meulen, M. Distraction from pain: The role of
selective attention and pain catastrophizing. Eur. J. Pain 2020, 24, 1880–1891. [CrossRef]
60. Jones, R.; Tarter, R.; Ross, A.M. Greenspace Interventions, Stress and Cortisol: A Scoping Review. Int. J. Environ. Res. Public Health
2021, 18, 2802. [CrossRef]
61. Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace
exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [CrossRef]
62. Gao, T.; Zhang, T.; Zhu, L.; Gao, Y.; Qui, L. Exploring Psychophysiological Restoration and Individual Preference in the Different
Environments Based on Virtual Reality. Int. J. Environ. Res. Public Health 2019, 16, 3102. [CrossRef]
63. Reese, G.; Stahlberg, J.; Menzel, C. Digital shinrin-yoku: Do nature experiences in virtual reality reduce stress and increase
well-being as stongly as similar experiences in a physical forest? Virtual Real. 2022, 1–11. [CrossRef]
64. Janeway, C.J.; Travers, P.; Walport, M.; Shlomchik, M.J. Immunobiology: The Immune System in Health and Disease, 5th ed.; Garland
Science: New York, NY, USA, 2001.
65. Muntasell, A.; Rojo, F.; Servitja, S.; Rubio-Perez, C.; Cabo, M.; Tamborero, D.; Costa-García, M.; Martínez-Garcia, M.; Menéndez, S.;
Vazquez, I.; et al. NK Cell infiltrates and HLA Class I expression in primary HER2+ breast cancer predict and uncouple
pathological response in disease-free survival. Clin. Cancer Res. 2018, 25, 1535–1545. [CrossRef]
66. Nersesian, S.; Schwartz, S.L.; Grantham, S.R.; MacLean, L.K.; Lee, S.N.; Pugh-Toole, M.; Boudreau, J.E. NK cell infiltration is
associated with improved overall survival in solid cancers: A systematic review and meta-analysis. Transl. Oncol. 2021, 14, 100930.
[CrossRef]
67. Antonelli, M.; Donelli, D.; Barbieri, G.; Valussi, M.; Maggini, V.; Firenzuoli, F. Forest volatile organic compounds and their effects
on human health: A state-of-the-art review. Int. J. Environ. Res. Public Health 2020, 17, 6505. [CrossRef]
68. Kishi, A.; Takamori, Y.; Ogawa, K.; Takano, S.; Tomita, S.; Tanigawa, M.; Niman, M.; Kishida, T.; Fujita, S. Differential expression
of granulysin and perforin by NK cells in cancer patients and correlation of impaired granulysin experssion with progression of
cancer. Cancer Immunol. Immunother. 2002, 50, 604–614. [CrossRef]
69. Okada, S.; Morishita, T. The role of granulysin in cancer immunology. Int. Sch. Res. Netw. ISRN Immunol. 2012, 2012, 876203.
[CrossRef]
70. Tsao, T.-M.; Tsao, T.M.; Tsai, M.J.; Hwang, J.S.; Cheng, W.F.; Wu, C.F.; Chou, C.K.; Su, T.C. Health effects of a forest environment
on natural killer cells in humans: An observational pilot study. Oncotarget 2018, 9, 16501–16511. [CrossRef]
71. Brattoli, M.; de Gennaro, G.; de Pinto, V.; Loiotile, A.D.; Lovascio, S.; Penza, M. Odour detection methods: Olfactometry and
chemical sensors. Sensors 2011, 11, 5290–5322. [CrossRef]
72. Kim, J.-C.; Dinh, T.-V.; Oh, H.-K.; Son, Y.-S.; Ahn, J.-W.; Song, K.-Y.; Choi, I.-Y.; Park, C.-R.; Szulejko, J.; Kim, K.-H. The potential
benefits of therapeutic treatment using gaseous terpenes at ambient low levels. Appl. Sci. 2019, 9, 4507. [CrossRef]
73. Kim, M.; Sowndhararajan, K.; Park, S.J.; Kim, S. Effect of inhalation of isomers of (+)-alpha-pinene and (+)-beta pinene on human
electroencephalographic activity according to gender difference. Eur. J. Integr. Med. 2018, 17, 33–39. [CrossRef]
74. Audrain, H.; Kenward, C.; Lovell, C.R.; Green, C.; Ormerod, A.D.; Sansom, J.; Chowdhury, M.M.U.; Cooper, S.M.; Johnston, G.A.;
Wilkinson, M.; et al. Allergy to oxidized limonene and linalook is frequent in the U. K. Br. J. Dermatol. 2014, 171, 292–297.
[CrossRef]
75. Filipsson, A.F. Short term infalation exposure to turpentine: Toxicokinetics and acute effects in men. Occup. Environ. Med. 1996,
53, 100–105. [CrossRef]
76. O’Connor, S. Virtual Reality and Avatars in Health care. Clin. Nurs. Res. 2019, 28, 523–528. [CrossRef]
77. Fisher, R.S.; Acharya, J.N.; Baumer, F.M.; French, J.A.; Parisi, P.; Solodar, J.H.; Szaflarski, J.P.; Thio, L.L.; Tolchin, B.; Wilkins, A.J.;
et al. Visually sensitive seizures: An updated review by the Epilepsy Foundation. Epilepsia 2022, 63, 739–768. [CrossRef]
78. Hunter, T.; Sandoval, D.; Booth, N.; Holdsworth, E.; Deodhar, A. Comparing symptoms, treatment patterns, and quality of
life of ankylosing spondylitis and non-radiographic axial spondyloarthritis patients in the USA: Findings from a patient and
rheumatologist Survey. Clin. Rheumatol. 2021, 40, 3161–3167. [CrossRef]
79. Byravan, S.; Jain, N.; Stairs, J.; Rennie, W.; Moorthy, A. Is There a Correlation Between Patient-Reported Bath Ankylosing
Spondylitis Disease Activity Index (BASDAI) Score and MRI Findings in Axial Spondyloarthropathy in Routine Clinical Practice?
Cureus 2021, 13, e19626. [CrossRef]

Int. J. Environ. Res. Public Health 2022, 19, 5373
17 of 17
80. Fragoulis, G.E.; Siebert, S. Treatment strategies in axial spondyloarthritis: What, when and how? Rheumatology 2020, 59 (Suppl. 4),
iv79–iv89. [CrossRef] [PubMed]
81. Guo, H.; Ferrara, M.; Coleman, J.; Loyola, M.; Meggers, F. Air temperature and mean radiant temperature data, collected and
simulated across a radiantly-heated high-bay laboratory. Data Brief 2020, 30, 105192. [CrossRef] [PubMed]
82. TSI. P-Trak™ Quick Guide for Indoor Air Quality Investigations; TSI: Shoreview, MN, USA, 2008.
83. Laboratories, G. TSI P-Trak Ultrafine Particle Counter. 2010. Available online: www.tsi.com (accessed on 5 January 2022).
84. Library, A.-H.T.V. RAE Systems ppbRAE Calibration. 2015. Available online: Argus-hazco.com (accessed on 5 January 2022).
85. Honeywell, R.S.B. ppbRAE 3000 User’s Guide; RAE Systems: San Jose, CA, USA, 2016.
86. Corporation, O.C. Onset HOBO MX2300 Temp RH Data Loggers; Bourne, MA, USA. Available online: https://www.onsetcomp.
com/products/software/hoboconnect (accessed on 5 January 2022).
87. Tronhon Co., Ltd. Asakuki 500 mL Premium Atomizer. Tronhon Co., Ltd.: Chongqing, China, 2022.
88. Araújo-Filho, H.G.; Pereira, E.W.M.; Rezende, M.M.; Menezes, P.P.; Araújo, A.A.S.; Barreto, R.S.S.; Martins, A.O.B.P.B.;
Albuquerque, T.R.; Silva, B.A.F.; Alcantara, I.S.; et al. D-limonene exhibits superior antihyperalgesic effects in a β-cyclodextrin-
complexed form in chronic musculoskeletal pain reducing Fos protein expression on spinal cord in mice. Neuroscience 2017, 358,
158–169. [CrossRef] [PubMed]
89. The Verge, VOX Media, LLC. HTC VIVE Pro Eye Hands-on with Eye Tracking; VOX Media: Washington, DC, USA, 2019.
90. VIVE HTC Corporation. VIVE Pro Eye User’s Guide; VIVE High-Tech Computer Corporation: Washington, DC, USA, 2020.
91. VIVE HTC Corporation. VIVE Support; VIVE High-Tech Computer Corporation: New Taipei City, Taiwan, 2022.
92. Fang, L.; Clausen, G.; Fanger, P.O. Temperature and humidity: Important factors for perception of air quality and for ventilation
requirements. ASHRAE Trans. 2000, 106, 503–510.
93. Li, Q.; Morimoto, K.; Nakadai, A.; Qu, T.; Matsushima, H.; Katsumata, M.; Shimizu, T.; Inagaki, H.; Hirata, Y.; Hirata, K.; et al.
Healthy lifestyles are associated with higher levels of perforin, granulysin, and granzymes A/B-expressing cells in peripheral
blood lymphocytes. Prev. Med. 2007, 44, 117–123. [CrossRef]
94. Lati, C.; Guthrie, L.C.; Ward, M.M. Comparison of the Construct Validity and Sensitivity to Change of the Visual Analog Scale and
a Modified Rating Scale as Measures of Patient Global Assessment in Rheumatoid Arthritis. J. Rheumatol. 2010, 37, 717. [CrossRef]
95. Callahan, L.F.; Brooks, R.H.; Summey, J.A.; Pincus, T. Quantitative pain assessment for routine care of rheumatoid arthritis
patients, using a pain scale based on activities of daily living and a visual analog pain scale. Arthritis Rheum. 1987, 30, 630–636.
[CrossRef]
96. Akin, A.; Çetın, B. The Depression Anxiety and Stress Scale (DASS): The study of validity and reliability. Educ. Sci. Theory Pract.
2007, 7, 260–268.
97. Nieuwenhuijsen, K.; de Boer, A.G.; Verbeek, J.H.; Blonk, R.W.; van Dijk, F.J. The Depression Anxiety Stress Scales (DASS):
Detecting anxiety disorder and depression in employees absent from work because of mental health problems. Occup. Environ.
Med. 2003, 60 (Suppl. 1), i77–i82. [CrossRef]
98. Fernández-Sueiro, J.L.; Willisch, A.; Pértega-Díaz, S.; Tasende, J.A.; Fernández-López, J.C.; Villar, N.O.; Galdo, F.; Blanco, F.J.
Validity of the bath ankylosing spondylitis disease activity index for the evaluation of disease activity in axial psoriatic arthritis.
Arthritis Care Res 2010, 62, 78–85. [CrossRef]
99. World Health Organization. WHOQOL and Spirituality, Religiousness and Personal Beliefs (SRPB). In Department of Mental
Health; Wrold Health Organization, Ed.; World Health Organization: Geneva, Switzerland, 1998; pp. 1–162.
100. Boonstra, A.; Schiphorst Preuper, H.R.; Reneman, M.F.; Posthumus, J.B.; Stewart, R.E. Reliability and validity of the visual
analogue scale for disability in patients with chronic musculoskeletal pain. Int. J. Rehabil. Res. 2008, 31, 165–169. [CrossRef]
[PubMed]
101. Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404.
[CrossRef] [PubMed]
102. Sendlbeck, M.; Araujo, E.G.; Schett, G.; Englbrecht, M. Psychometric properties of three single-item pain scales in patients with
rheumatoid arthritis seen during routine clinical care: A comparative perspective on construct validity, reproducibility and
internal responsiveness. RMD Open 2015, 1, e000140. [CrossRef]
103. Myles, P.S.; Troedel, S.; Boquest, M.; Reeves, M. The Pain Visual Analog Scale: Is It Linear or Nonlinear? Anesth. Analg. 1999, 89,
1517–1520. [CrossRef] [PubMed]
104. Brown, T.A.; Chorpita, B.F.; Korotitsch, W.; Barlow, D.H. Psychometric properties of the Depression Anxiety Stress Scales (DASS)
in clinical samples. Behav. Res. Ther. 1997, 35, 79–89. [CrossRef]
105. Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A new approach to defining disease status in
ankylosing spondylitis: The Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 1994, 21, 2286–2291.
106. Gossec, L. Chapter 5—Monitoring of Disease and Treatment of Patients with Rheumatic Disease. In Handbook of Systemic
Autoimmune Diseases; Atzeni, F., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 97–125.
107. Maecker, H.T.; McCoy, J.P.; Nussenblatt, R. Standardizing immunophenotyping for the Human Immunology Project. Nat. Rev.
Immunol. 2012, 12, 191–200. [CrossRef]
108. Horlock, C. Enzyme-Linked Immunosorbent Assay (ELISA); British Society for Immunology: London, UK, 2016.